LOWER-EXTREMITY CONSTRAINT-INDUCED MOVEMENT THERAPY IN INDIVIDUALS WITH STROKE – IMPROVEMENTS, EXPERIENCES AND HEALTH-RELATED QUALITY OF LIFE
Ingela Marklund

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
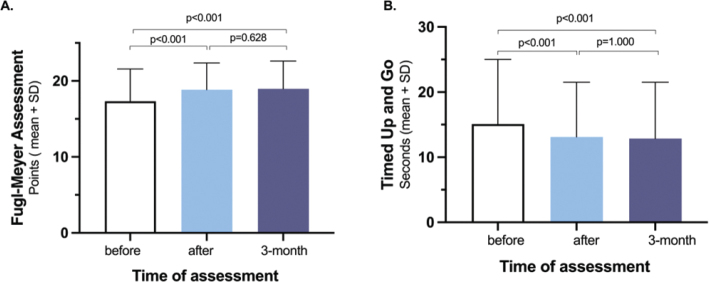 Figure 1
Figure 1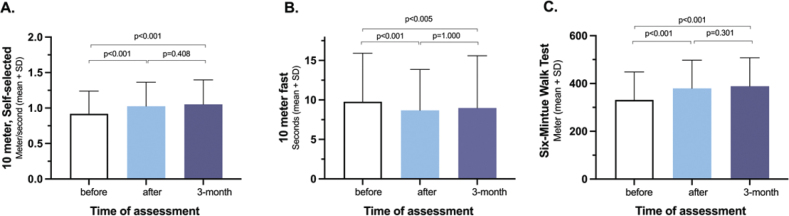 Figure 2
Figure 2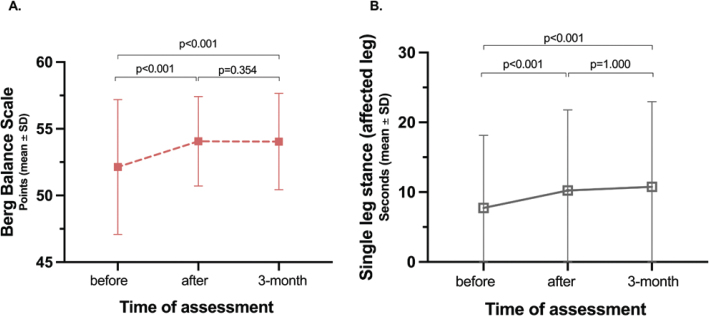 Figure 3
Figure 3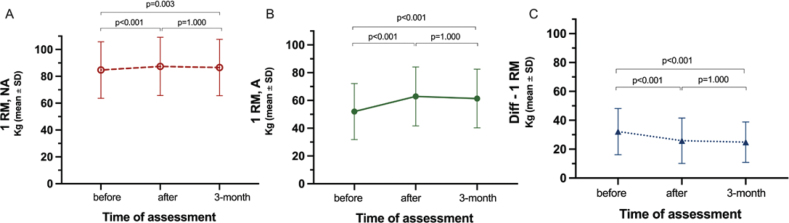 Figure 4
Figure 4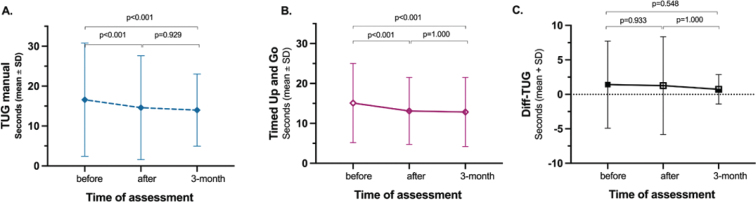 Figure 5
Figure 5 Figure 6
Figure 6Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsStroke Rehabilitation and Recovery · Cerebral Palsy and Movement Disorders · Musculoskeletal pain and rehabilitation
On November 24, 2023 Ingela Marklund defended her thesis Lower-extremity constraint-induced movement therapy in individuals with stroke – improvements, experiences and health-related quality of life at the Umeå University, Umeå, Sweden. Supervisors: Maria Klässbo, Brynjar Fure, Britt-Marie Stålnacke, Xiaolei Hu.
Stroke is the third-leading cause of disability worldwide, and there are rehabilitation needs not only in the first year but also throughout the lifetime. The ability to walk is crucial in everyday life since it affects mobility, self-care and social activities. National guidelines recommend treating impairments with repetitive task- and goal-oriented exercises. One form of highly intensive and task-specific treatment is constraint-induced movement therapy (CIMT), a treatment method developed based on understanding brain plasticity with a behavioural explanatory model. There is insufficient evidence regarding CIMT for the lower extremities (LE-CIMT) since it has only been investigated in a few published studies involving only a small number of participants. The overall aims of this thesis were to explore the extent to which LE-CIMT (6 h per day for 2 weeks) can improve impaired body functions and limited activities, describe how the treatment is experienced by patients and investigate whether it affects the health-related quality of life (HRQoL) of individuals with stroke. This thesis contains 5 papers that analysed data from 2 study populations using quantitative and qualitative research methods (Table I).
The intervention consisted of individually tailored LE-CIMT in groups of 2–4 participants with intensive massed practice (6 h/day for 10 consecutive weekdays) supervised by a physiotherapist. The LE-CIMT included various training sessions focusing on motor function, balance, strength, locomotor training indoors and outdoors, functional training and stretching of short muscles. Training programmes were based on pre-test results and individual goals and were revised on a daily basis by the physiotherapist. More details about the intervention and data collection are described in the chapters Intervention and Data collection (Table II).
The results showed in paper I that LE-CIMT can improve motor function, dynamic balance, mobility and walking ability in individuals in the chronic stage of stroke recovery. Of the 30 variables measured in 5 subjects with 6 measuring instruments, 23 (77%) improved, with 12 (52%) improving significantly. The improvements remained at the long-term follow-ups (3 and 6 months after LE-CIMT) for 22 of the 23 variables. In addition, the weight-bearing distribution measured standing on 2 scales before, directly after and 3 and 6 months after LE-CIMT. All subjects increased the weight borne by their more affected leg after LE-CIMT, providing a more symmetric weight distribution, and the improvements persisted at the 3- and 6-month follow-ups.
In papers II and III, LE-CIMT significantly enhanced motor function, mobility, balance, dual-task ability, leg-strength and walking ability. These improvements remained at the 3-month follow-up (Figs 1–5). Those who completed the intervention 1–6 months after stroke onset showed significantly greater improvements in walking speed, measured with 10-m walk test during the follow-up than those who completed the intervention 7 months or more after stroke onset. In addition, balance measured using the Berg balance score scores decreased with age.
In the analysis of the interviews (Paper IV), 2 main categories emerged from the manifest content (the therapy and me and my body) with 4 and 3 subcategories, respectively. From these categories, an overall theme constituted the latent content of the material: knowledge of myself and my prospects for leading an easier life.
The main category (the therapy) included the informant’s experiences of the preparation before LE-CIMT, the actual intensive training and its improvements, and their views of the staff who conducted LE-CIMT. Preparation was considered vital for all participants undergoing LE-CIMT. Since LE-CIMT involves rigorous and intense training, it was crucial to mentally prepare for the challenges ahead.
The training was experienced as concentrated, intensive and challenging since each exercise was always at the limit of each individual’s ability and capacity. The restriction, with the whole-leg orthosis, of the less-affected leg during training forced the informants to use the more affected leg more than before. The training consisted mainly of learning, for example, how to walk in a new way without compensation and to do things they did not believe they would manage.
The physical improvements were experienced during and after LE-CIMT and described in various ways: stronger leg, better balance, better coping and greater use of the leg than before.
A feeling of freedom outweighed all the hard work, and the informants became aware of how fragile and exposed their situation was.
The informants reported that the physiotherapists were very professional, competent and sensitive to changes. They made demands, provided positive feedback and encouragement, participated in all activities during the day and “shared their lives.”
The second main category (me and my body) included the informants’ reflections on their importance in the treatment, how this has affected them and what insight it provided about their situation. The informants’ motivation, persistence and the fact that they decided to participate were critical aspects of completing LE-CIMT. They felt that they were specially chosen and made an effort since few had the opportunity to undergo this therapy.
The physical improvements changed the informants’ perspective of their capacity and provided a sense of human dignity, “not to be finished as a human being.” By succeeding in various exercises and achieving their goals, self-esteem was strengthened, and faith in the future was awakened. The knowledge that informants gained about their bodies during treatment gave them security in their everyday lives. Change is also about spreading knowledge and the experience they have gained. It was important for them to be able to talk about their experiences and thus influence the situation of others recovering after a stroke. They also perceived that others experienced them differently after LE-CIMT.
The informants felt frustrated that few in healthcare knew about LE-CIMT. Reflecting on their earlier rehabilitation, the informants expressed a need to “raise the bar” and for an overarching programme that begins at acute stroke onset and encompasses lifelong rehabilitation so they can plan their future.
Despite their knowledge and experience of LE-CIMT, the informants felt they could not train intensively by themselves, and recurring periods of LE-CIMT were needed. The frustration that LE-CIMT is unavailable in healthcare and the experience that the county councils resist introducing new treatment methods became clear.
The informants experienced that LE-CIMT, through intensive repetition of training and information/education, gave them knowledge about themselves and how their body works, allowing them to live an easier life. They felt there was still hope and opportunity for functional improvements, which increased their independence and self-esteem.
In paper V, the respondents estimated lower HRQoL than norm-based data in every domain except pain where it was equal. The greatest differences were seen in the physical functioning and role-functioning physical domains. Comparisons between the sample’s means and norm-based reference data showed significantly decreased HRQoL for the participants in 4 out of 8 domains in the Swedish RAND-36 scale, physical functioning, role-functioning physical, social functioning and general health. There were no significant differences in HRQoL for the domains pain, energy/fatigue and role-functioning emotional well-being. In the univariable analysis adjusted for age and sex, the linear relationship between participants’ scores in the 8 RAND-36 domains and their previous result on walking distance measured with Six-minute Walk test (6MWT), time since treatment and living conditions were analysed. There was a significant association between 6MWT and physical functioning. For every 100-m increase in 6MWT after LE-CIMT, the physical functioning score increased by 6.45 points in RAND-36. No other significant associations were found. More details about the results in the various papers are described in the chapter Results.
Finally, Chapter Discussion provides a general discussion of the results of this thesis. The main conclusion is that LE-CIMT appears useful in improving impaired body functions and limited activities after a stroke and can be conducted in day hospital rehabilitation and outpatient clinics. It seems possible to achieve these improvements even a long time after stroke onset, regardless of age, sex, stroke type or affected side. Earlier treatment after stroke onset generates greater improvements in walking ability, and the improved dual-task ability might reduce the risk of falls. LE-CIMT also provides knowledge and how to live an easier life. The intensive treatment gave hope since the improvements showed the possibilities for change, which, in turn, increasing independence and self-esteem. Whilst LE-CIMT was hard and difficult, it was felt entirely necessary.
The general discussion examines the results in the thesis in relation to previous studies, methodological considerations, strengths and limitations during study design, data collection and statistical analysis. Finally, the thesis considers the clinical implications and possible directions for future research.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Marklund I, Klässbo M. Effects of lower limb intensive mass practice in poststroke patients: single-subject experimental design with long-term follow-up. Clin Rehabil 2006; 20: 568–576. 10.1191/0269215506 cr 973oa 16894799 · doi ↗ · pubmed ↗
- 2Marklund I, Sefastsson A, Fure B, Klässbo M, Liv P, Stålnacke BM, et al. Lower-extremity constraint-induced movement therapy improved motor function, mobility, and walking after stroke. Eur J Phys Rehabil Med 2023; 59: 136–144. 10.23736/S 1973-9087.23.07683-936892520 PMC 10171361 · doi ↗ · pubmed ↗
- 3Sefastsson A, Marklund I, Littbrand H, Wester P, Stålnacke BM, Sörlin A, et al. Positive effects of lower extremity constraint-induced movement therapy on balance, leg strength, and dual-task ability in stroke patients: a longitudinal cohort study. J Rehabil Med 2024; 56: jrm 24168. 10.2340/jrm.v 56.2416839360525 PMC 11462090 · doi ↗ · pubmed ↗
- 4Marklund I, Klässbo M, Hedelin B. “I got knowledge of myself and my prospects for leading an easier life”: Stroke patients’ experience of training with lower-limb CIMT. Adv Physiother 2010; 12: 134–141. 10.3109/14038190903141048 · doi ↗
- 5Marklund I, Fure B, Klässbo M, Liv P, Stålnacke BM, Hu X. Post-stroke health-related quality of life after lower-extremity constraint induced movement therapy: a cross-sectional survey study. Submitted.