“Terrible Triad” Injury in an Adolescent Patient With a High-Energy Femoral Shaft Fracture: A Case Report
Alexandros E Koskiniotis, Nikolaos Stefanou, Efstathios Konstantinou, Efstratios D Athanaselis, Sokratis Varitimidis

TL;DR
A young patient with a femur fracture and multiple complications is described, highlighting a rare sequence of injuries and surgical challenges.
Contribution
The paper introduces the concept of a 'terrible triad injury' in femoral shaft fractures involving implant failure and patellar tendon rupture.
Findings
The patient required multiple surgeries due to implant failure and complications.
A 'terrible triad injury' sequence was identified involving femoral fracture fixation, revision, and patellar tendon rupture.
Current guidelines for surgical fixation in polytrauma patients with respiratory dysfunction are lacking.
Abstract
Although femoral shaft fractures are typically treated with intramedullary nailing, alternative fixation methods like plating are required in select cases, particularly when nailing may be contraindicated due to respiratory complications or other patient-specific factors. Currently, there are no established guidelines for the optimal surgical fixation method of femoral shaft fractures in polytrauma patients with respiratory dysfunction. We present the case of a young patient with a diaphyseal femur fracture who underwent multiple surgical interventions within three months due to recurrent injuries and complications, primarily resulting from non-adherence to postoperative guidelines. We describe this sequence as a "terrible triad injury", consisting of primary fixation of the femoral fracture, revision of the first osteosynthesis due to recurrent trauma and implant failure, and a…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
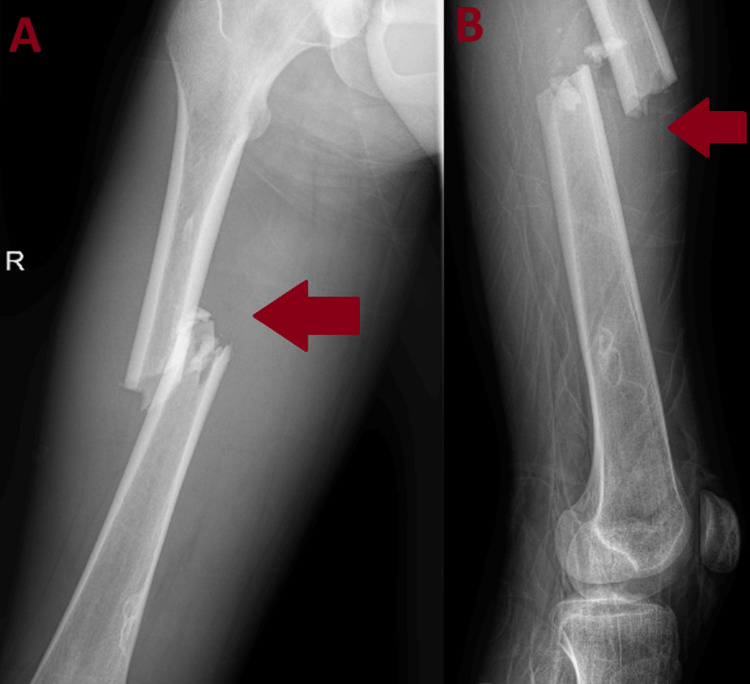 Figure 1
Figure 1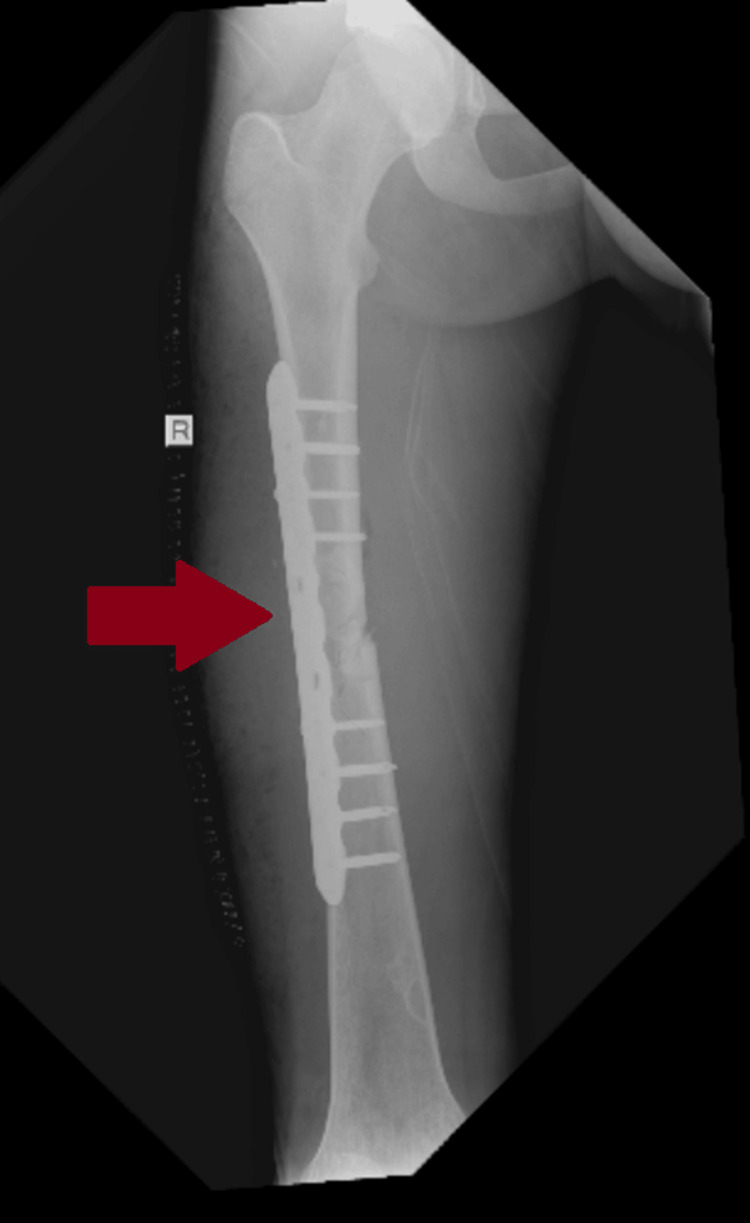 Figure 2
Figure 2 Figure 3
Figure 3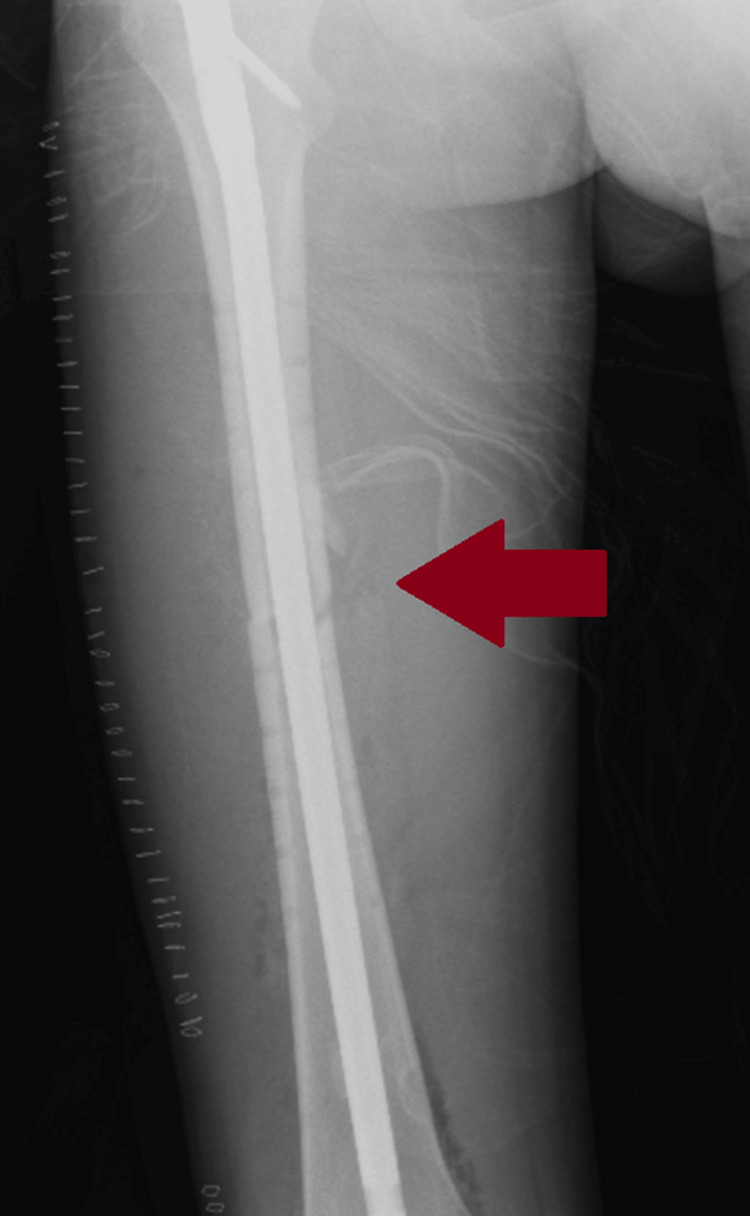 Figure 4
Figure 4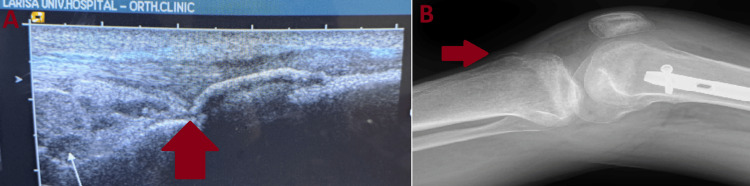 Figure 5
Figure 5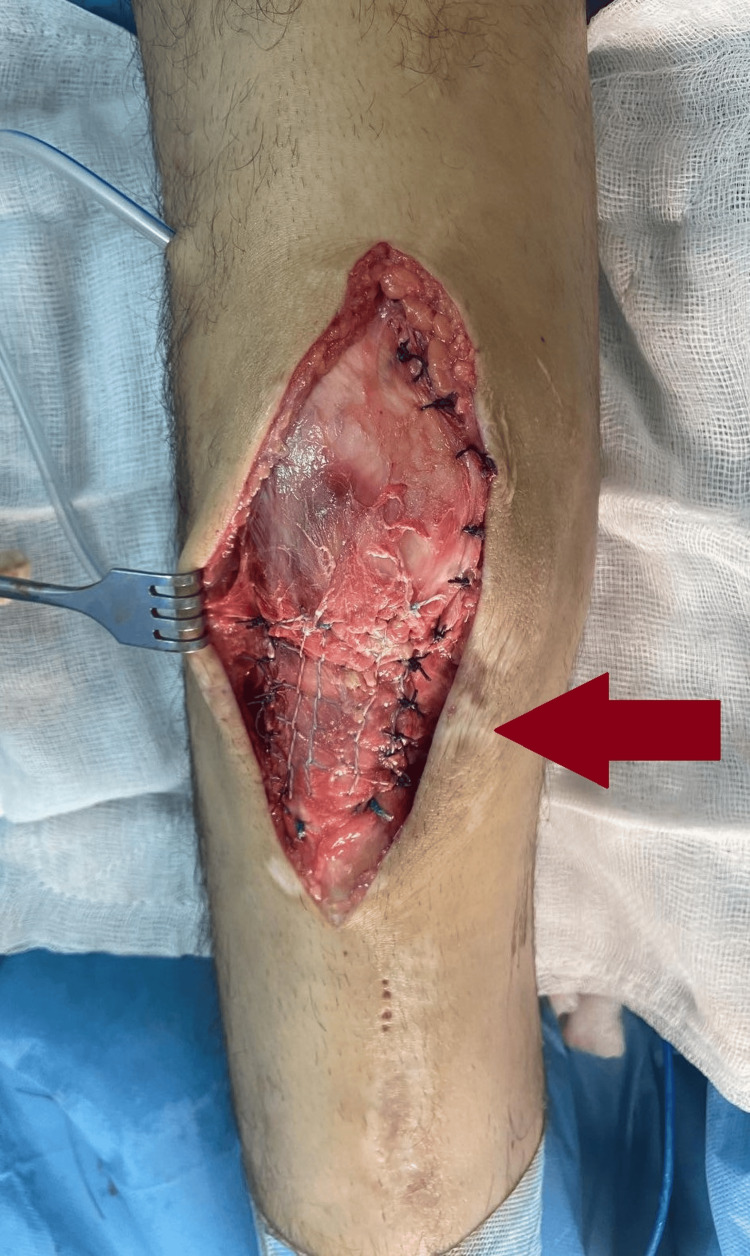 Figure 6
Figure 6 Figure 7
Figure 7Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsBone fractures and treatments · Hip and Femur Fractures · Orthopedic Infections and Treatments
Introduction
Femoral shaft fractures are common orthopedic injuries with a bimodal age distribution. They often occur in younger patients due to high-energy trauma, which may be associated with life-threatening injuries (e.g., pulmonary or cerebral), or in older patients due to low-energy mechanisms, such as simple falls [1]. Intramedullary nailing is the gold standard treatment for these fractures, providing excellent functional outcomes and advantages such as early weight-bearing and minimal soft tissue damage, thereby reducing surgical site complications [2]. However, complications like respiratory dysfunction due to fat embolism may contraindicate nailing, making open reduction and internal fixation (ORIF) with a plate a more suitable alternative [3]. This case report presents a young patient with a femoral shaft fracture who required multiple surgical interventions within three months due to consecutive injuries and complications, primarily resulting from non-adherence to postoperative guidelines. We describe this sequence as a "terrible triad injury", comprising primary fixation of the femoral fracture, revision of the first osteosynthesis due to recurrent trauma and implant failure, and a subsequent patellar tendon rupture.
Case presentation
A 17-year-old male with no significant medical history presented to our emergency department following a motorcycle accident. He had sustained a diaphyseal fracture of the right femur without significant soft tissue trauma and an ipsilateral sixth rib fracture (Figure 1).
Preoperative images of the right femoral shaft fractureA) Anteroposterior X-ray of the femur. B) Lateral X-ray of the femur
Despite being hemodynamically stable, the patient reported shortness of breath and chest pain unrelated to the rib fracture. His oxygen saturation (SpO₂) was 90%, accompanied by tachypnea. A clinical evaluation by a pulmonologist and a chest CT scan revealed no specific findings; however, a low-grade fat embolism was strongly suspected. Given this diagnosis, the use of reamed intramedullary nailing was avoided due to concerns about exacerbating respiratory symptoms. Instead, ORIF with a plate was performed to minimize operative time and potential complications (Figure 2).
Immediate anteroposterior postoperative X-ray after fixation of the diaphyseal femur fracture with a plate
Postoperatively, the patient was instructed to perform toe-touch weight-bearing and active and passive range-of-motion exercises. Three days after surgery, his respiratory condition improved, and he was discharged from the hospital.
Unfortunately, the patient sustained another fall 19 days later while bathing unsupervised. This resulted in plate failure and a re-fracture at the original femoral diaphysis site (Figure 3).
Failure of the osteosynthesis due to breakage of the plate after a second accident, resulting in a re-fracture at the operated site
Since his respiratory symptoms had resolved, the fracture was treated with an intramedullary nail during a second operation (Figure 4).
Removal of the plate and intramedullary nail fixation of the femoral shaft re-fracture
The patient was instructed on strict weight-bearing restrictions under supervision and prescribed a rehabilitation program. At his two-month follow-up, he demonstrated significant improvement, with a near-normal range of motion and the ability to walk unaided.
However, non-compliance with postoperative instructions once again led to complications. After growing over-confident due to his excellent recovery, the patient resumed motorbike riding, against medical advice, and sustained a low-velocity fall. This time, he ruptured the patellar tendon in his previously operated limb, though no new fractures were identified (Figure 5).
Ultrasound and X-ray imaging of the injured knee after the third traumatic incident of the patientA bony avulsion can be seen in both imagesA) Ultrasound image of the injured knee in longitudinal view. A partial rupture of the patellar tendon and a bone avulsion can be seen near the tibial tubercle. B) Lateral X-ray of the injured knee
Surgical repair of the ruptured tendon was performed, marking his third operation within three months (Figure 6).
Intraoperative image of surgical repair of the ruptured patellar tendon
After these setbacks, the patient adhered to his surgeon's instructions. Nine months after the initial surgery, the femoral fracture had fully healed, with excellent knee extension. However, the patient exhibited limited knee flexion (100 degrees) and noticeable atrophy in his multi-injured right thigh (Figure 7).
Obvious atrophy and limited flexion of the operated limb when compared with the healthy lower extremityA) Atrophy of the right quadriceps muscle. B) Limited flexion around 100 degrees in the operated limb
Discussion
Intramedullary nailing of femoral shaft fractures is a well-established method of indirect fixation, offering undeniable advantages over classic ORIF techniques. This has made it the preferred choice of treatment for the majority of orthopedic surgeons to stabilize shaft fractures of long bones. However, in some cases, intramedullary nailing may pose risks to the overall condition of the patient. Epidemiological studies indicate that approximately 30% of femoral shaft fractures occur in polytrauma patients, who may present with severe thoracic trauma and acute respiratory complications [4]. Fat embolism syndrome is another potential concern in polytrauma patients, particularly in the presence of a long bone fracture [5]. Recent studies investigating the impact of intramedullary nailing of long bone fractures on patients' respiratory function suggest that the increase in intramedullary pressure during nail insertion can raise the risk of fat embolism and pulmonary dysfunction [6]. Hence, although no established guidelines currently exist for the optimal surgical fixation method in these patients, many surgeons prefer alternative fixation techniques over nailing in cases of polytrauma patients with severe thoracic injuries and compromised cardiorespiratory function [7].
Most published studies on femoral shaft plating primarily focus on the pediatric population, as the widespread use of intramedullary nails has significantly reduced the frequency of open reduction and plate fixation in adults. Despite this trend, several studies suggest that techniques such as conventional single plate fixation, minimally invasive plate osteosynthesis (MIPO), and double plate fixation can serve as viable alternatives when nailing is contraindicated. These techniques have been shown to provide comparable final functional outcomes and support fast recovery [7-9]. However, while the overall results may be similar across these fixation methods, infection, malunion, and implant failure rates are reported to be higher with plate fixation compared to intramedullary nailing, according to the literature [10].
Another concern in our case is whether a revision fixation method, such as converting from ORIF with a plate to intramedullary nailing, yields similar functional outcomes and union rates compared to primary fixation. Studies specifically examining the functional outcomes of revision fixation methods for femoral diaphyseal fractures, in comparison to primary surgeries, are scarce. However, we can draw parallels to cases where patients have undergone a conversion from plate fixation to intramedullary nailing for femoral shaft non-unions. A systematic review by Somford et al. reported a union rate of 96% for failed plate constructs in femoral shaft non-unions, with excellent outcomes and recovery [11]. Our patient demonstrated excellent recovery following the second surgery before the patellar tendon rupture, with rapid imaging and clinical signs of union, as well as a great range of motion without any restrictions. It is undeniable though that a second operation, particularly when performed so soon after the primary procedure, significantly increases the risk of complications such as infection, delayed wound healing, and prolonged rehabilitation time [12].
Our brief review of the literature could not identify any studies linking femoral shaft fractures with late patellar tendon rupture as a postoperative complication. However, such injuries have been documented as concomitant injuries in high-energy traumatic events. A case report by Bek et al. [13] refers to a case of a neglected patellar tendon rupture in a patient who presented to the emergency department with an ipsilateral femoral shaft and tibial plateau fracture; the patellar tendon was reconstructed using semitendinosus and gracilis tendon grafts, resulting in a final range of motion of 5-110 degrees. Our patient demonstrated excellent knee extension but experienced restricted knee flexion, achieving a maximum of 100 degrees postoperatively. Similar outcomes are reported in recent literature, with authors noting high rates of patients returning to sports activities after primary patellar tendon repair, albeit with some degree of flexion loss when compared to the contralateral healthy knee [14,15]
Compliance with orthopedic surgeons' guidelines is crucial for achieving successful union and postoperative outcomes, particularly in cases of extremely comminuted lower extremity fractures where immediate weight-bearing might not be advised [16]. In a single-blinded study by Christopher et al., weight-bearing restrictions were tested using pressure-sensitive film embedded in short leg casts. The study revealed that a significant proportion of patients (approximately 27.5%) did not adhere to the non-weight-bearing guidelines. Interestingly, factors such as sex, age, language spoken, BMI, and the surgeon involved were not significant predictors of non-compliance. The only statistically significant factor associated with non-compliance was the time of year the cast was worn, with patients being more likely to stand on their injured limbs during warmer months than in colder months [17].
Conclusions
This report highlights the importance of adhering to postoperative guidelines for ensuring successful outcomes after surgical management of femoral shaft fractures. While intramedullary nailing remains the gold standard, alternative fixation methods like plating are essential when contraindications exist. Revision to intramedullary nailing after failed plate fixation generally provides promising functional outcomes, but patient compliance with the surgeon’s guidelines is crucial to optimize recovery and prevent further complications. Careful surgical decision-making, particularly in polytrauma patients, and thorough follow-up care are essential for successful outcomes in femoral diaphyseal fractures.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Management of traumatic femur fractures: a focus on the time to intramedullary nailing and clinical outcomes Diagnostics (Basel) Ghouri SI Mustafa F Kanbar A 141613202310.3390/diagnostics 13061147 PMC 1004742836980455 · doi ↗ · pubmed ↗
- 2Intramedullary nailing of the femur: current concepts concerning reaming J Orthop Trauma Rudloff MI Smith WR 0723200910.1097/BOT.0b 013e 31819 f 258a 19390369 · doi ↗ · pubmed ↗
- 3Fat embolism: the reaming controversy Injury Giannoudis PV Tzioupis C Pape HC 0837200610.1016/j.injury.2006.08.04016990061 · doi ↗ · pubmed ↗
- 4Population-based epidemiology of femur shaft fractures J Trauma Acute Care Surg Enninghorst N Mc Dougall D Evans JA Sisak K Balogh ZJ 151615207420132369488110.1097/TA.0b 013e 31828 c 3dc 9 · doi ↗ · pubmed ↗
- 5Emergency management of fat embolism syndrome J Emerg Trauma Shock Shaikh N 2933220091956195310.4103/0974-2700.44680 PMC 2700578 · doi ↗ · pubmed ↗
- 6Secondary effects of femoral instrumentation on pulmonary physiology in a standardised sheep model: what is the effect of lung contusion and reaming?Injury Hildebrand F Giannoudis P van Griensven M 5445553620051575543810.1016/j.injury.2004.10.017 · doi ↗ · pubmed ↗
- 7Comparison of two biological internal fixation techniques in the treatment of adult femur shaft fractures (plate-screws and locked intramedullary nail)Ulus Travma Acil Cerrahi Derg Köseoğlu E Durak K Bilgen MS Küçükalp A Bayyurt S 159165172011 https://pubmed.ncbi.nlm.nih.gov/21644095/21644095 · pubmed ↗
- 8Minimally invasive plate osteosynthesis (MIPO) in the treatment of the femoral shaft fracture where intramedullary nailing is not indicated Int Orthop Apivatthakakul T Chiewcharntanakit S 111911263320091859708710.1007/s 00264-008-0603-2PMC 2898967 · doi ↗ · pubmed ↗