External quality assessment of molecular detection and variant typing of SARS-CoV-2 in European expert laboratories in 2023
Kim C. Heimsch, Kamelia R. Stanoeva, Ramona Mögling, Annette Kraus, Eeva K. Broberg, Jan Felix Drexler, Chantal B. E. M. Reusken, Adam Meijer, Christian Drosten, Victor M. Corman

TL;DR
European laboratories improved their SARS-CoV-2 detection accuracy over time through regular quality assessments.
Contribution
Demonstrates improved diagnostic accuracy and standardization of SARS-CoV-2 testing in European labs via repeated external quality assessments.
Findings
34 out of 38 (90%) laboratories correctly detected all SARS-CoV-2 samples in 2023, up from 12% in 2020.
Commercial assays became more widely used compared to in-house methods over time.
Routine external quality assessments are shown to enhance diagnostic reliability and standardization.
Abstract
The COVID-19 pandemic highlighted the importance of laboratory preparedness. Regular monitoring of diagnostic tools via external quality assessments (EQAs) is key to maintaining robust public health response service. We hereby conducted a third SARS-CoV-2 EQA assessing the diagnostic capabilities of European expert public health laboratories. A 10 samples panel containing Alpha (used in previous EQA), BA.4, BA.5, and BQ.1.18 variants along with human seasonal coronaviruses and negative controls was produced and validated. Participants were invited by the European Centre for Disease Prevention and Control (ECDC) and asked to submit results and assay details via electronic forms. Thirty-eight laboratories from 31 European countries participated. Most (n = 32, 84%) identified all panel samples correctly and used in-house (11, 29%), commercial assays (22, 58%), or both (5, 13%). Compared to…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
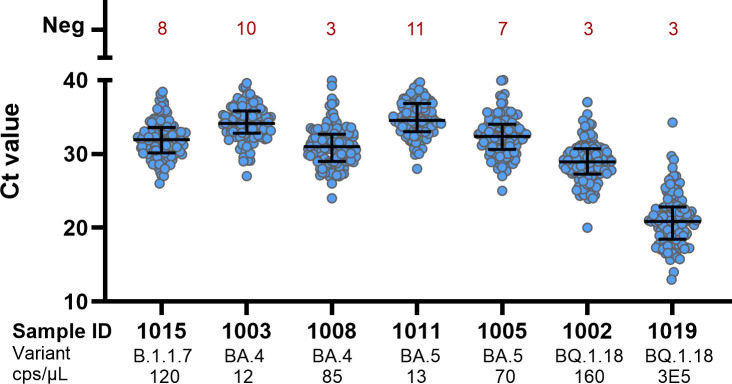 Fig 1
Fig 1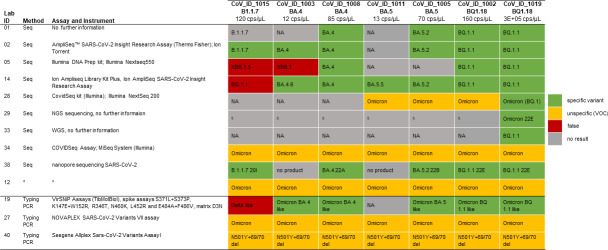 Fig 2
Fig 2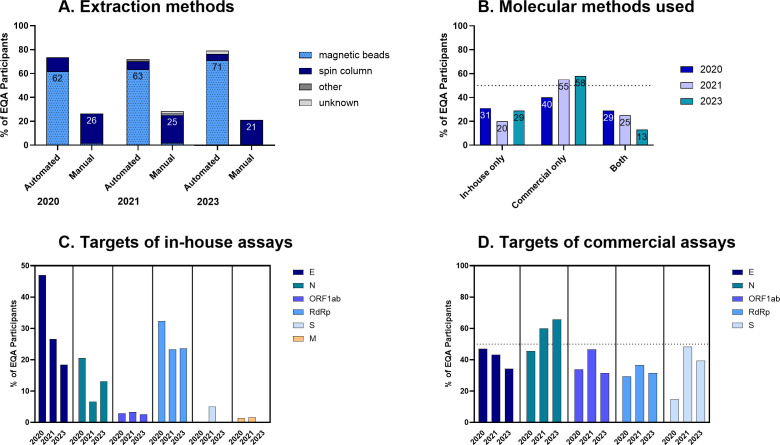 Fig 3
Fig 3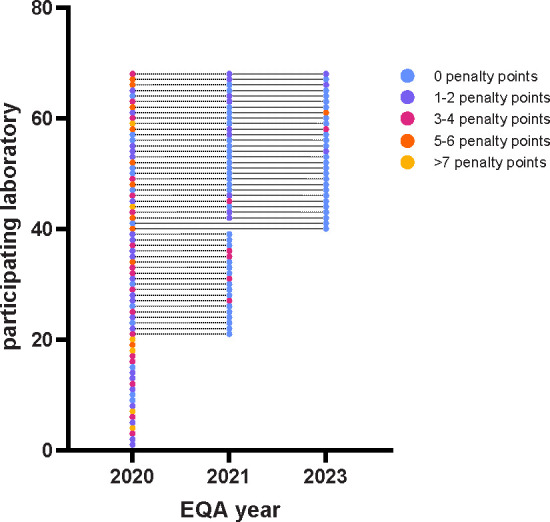 Fig 4
Fig 4| Sample ID | Virus | Lineage | Mutations | Copies/µL | Correct molecular detection | Correct SARS-CoV-2 variant determination | ||
|---|---|---|---|---|---|---|---|---|
| % | No./total labs | % | No./total labs | |||||
| CoV_ID_1015 | SARS-CoV-2 | B.1.1.7 | H69/V70 del Y144 del N501Y A570D P681H T716I S982A D1118H | 120 | 97 | 37/38 | 31 | 4/13 |
| CoV_ID_1003 | SARS-CoV-2 | BA.4 | T19I L24/P25/P26 del A27S H69/V70 del G142D V213G G339D S371F S373P S375F T376A D405N R408S K417N N440K L452R S477N T478K E484A F486V Q498R N501Y Y505H H655Y N679K P681H N764K D796Y Q954H N969K | 12 | 95 | 36/38 | 27 | 3/13 |
| CoV_ID_1008 | SARS-CoV-2 | BA.4 | T19I L24/P25/P26 del A27S H69/V70 del G142D V213G G339D S371F S373P S375F T376A D405N R408S K417N N440K L452R S477N T478K E484A F486V Q498R N501Y Y505H H655Y N679K P681H N764K D796Y Q954H N969K | 85 | 100 | 38/38 | 46 | 6/13 |
| CoV_ID_1011 | SARS-CoV-2 | BA.5 | T19I L24/P25/P26 del A27S H69/V70 del G142D V213G G339D S371F S373P S375F T376A D405N R408S K417N N440K L452R S477N T478K E484A F486V Q498R N501Y Y505H H655Y N679K P681H N764K D796Y Q954H N969K | 13 | 95 | 36/38 | 8 | 1/113 |
| CoV_ID_1005 | SARS-CoV-2 | BA.5 | T19I L24/P25/P26 del A27S H69/V70 del G142D V213G G339D S371F S373P S375F T376A D405N R408S K417N N440K L452R S477N T478K E484A F486V Q498R N501Y Y505H H655Y N679K P681H N764K D796Y Q954H N969K | 70 | 97 | 37/38 | 39 | 5/13 |
| CoV_ID_1002 | SARS-CoV-2 | BQ.1.18 | T19I L24/P25/P26 del A27S H69/V70 del G142D V213G G339D S371F S373P S375F T376A D405N R408S K417N N440K K444T L452R N460K S477N T478K E484A F486V Q493Q Q498R N501Y Y505H H655Y N679K P681H N764K D796Y Q954H N969K | 160 | 100 | 38/38 | 46 | 6/13 |
| CoV_ID_1019 | SARS-CoV-2 | BQ.1.18 | T19I L24/P25/P26 del A27S H69/V70 del G142D V213G G339D S371F S373P S375F T376A D405N R408S K417N N440K K444T L452R N460K S477N T478K E484A F486V Q493Q Q498R N501Y Y505H H655Y N679K P681H N764K D796Y Q954H N969K | 3E + 05 | 97 | 37/38 | 69 | 9/13 |
| CoV_ID_1004 | Human coronavirus 229E | 225 | 100 | 38/38 | ||||
| CoV_ID_1018 | Human coronavirus OC43 | 98 | 95 | 36/38 | ||||
| CoV_ID_1001 | - | 97 | 37/38 | |||||
| 1st EQA 2020 | 2nd EQA 2021 | 3rd EQA 2023 | |
|---|---|---|---|
| Participation | |||
| Participating laboratories ( | 68 | 60 | 38 |
| Represented countries ( | 35 | 34 | 31 |
| Represented EU/EEA countries ( | 28 | 28 | 27 |
| Represented pre-accession countries ( | 5 | 6 | 4 |
| Participating laboratories per country (average; min–max) | 2; 1–7 | 2; 1–7 | 1; 1–3 |
| Methods ( | |||
| Automated extraction | 50; 74% | 43; 72% | 30; 79% |
| Manual extraction | 18; 26% | 17; 28% | 8; 21% |
| Only in-house methods used | 21; 31% | 12; 20% | 11; 29% |
| Only commercial methods | 27; 40% | 33; 55% | 22; 58% |
| Both in-house and commercial methods | 20; 29% | 15; 25% | 5; 13% |
| Determination of virus variants by PCR or sequencing | NA | 37; 60% | 15; 39% |
| Sequencing performed | 2; 3% | 14; 23% | 7; 18% |
| Results ( | |||
| All SARS-CoV-2 containing samples correctly classified | 8; 12% | 45; 75% | 34; 90% |
| >50% of SARS-CoV-2 containing samples correctly classified | 23; 34% | 60; 100% | 38; 100% |
| All no SARS-CoV-2 containing control samples correctly classified | 37; 54% | 59; 98% | 35; 92% |
| All SARS-CoV-2 containing samples with variants and/or mutations identified | NA | 3; 8% | 1; 7% |
| >50% of SARS-CoV-2 containing samples with variants and/or mutations identified | NA | 26; 70% | 10; 67% |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsSARS-CoV-2 detection and testing · SARS-CoV-2 and COVID-19 Research · Biosensors and Analytical Detection
INTRODUCTION
The severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) pandemic highlighted the importance of laboratory preparedness and maintaining robust diagnostic and response services. Regular monitoring, via conducting external quality assessments (EQAs), is key to maintaining capacity and capability to rapidly and correctly detect pathogens and monitor their evolution (variant monitoring). In Europe, two EQAs of molecular detection and characterization of SARS-CoV-2 that were organized in 2020 and 2021 (1, 2) showed improvement in diagnostic sensitivity but still revealed detection issues with samples with low RNA concentrations. Here, we report on a follow-up EQA to assess again the performance of European expert laboratories, including testing capacities for recent strains in the aftermath of the COVID-19 pandemic.
MATERIALS AND METHODS
Participants
The European Centre for Disease Prevention and Control (ECDC) outsourced the implementation of this EQA to the AURORAE consortium (3) and invited operational contact points for the European COVID-19 reference laboratory network (ECOVID-LabNet) to register by the end of March 2023. The aim was to include all national reference laboratories or laboratories acting as such involved in the COVID-19 response, similar to the two previous European SARS-CoV-2 EQAs. The list of participating laboratories is given in the Acknowledgements.
Panel composition
The EQA panel contained 10 samples: seven with inactivated material of different SARS-CoV-2 lineages (Alpha variant B.1.1.7, and Omicron variants BA.4, BA.5, and BQ.1.18), two controls with inactivated material of two seasonal human coronaviruses (HCoV-229E and HCoV-OC43), and one negative control with phosphate-buffered saline (PBS) (Table 1). Two different concentrations of BA.4, BA.5, and BQ.1.18 were included in the panel to evaluate sensitivity. The lowest concentrations of BA.4 and BA.5 were 12 and 13 cps/µL, respectively (resuspended EQA vial). These variants were chosen to represent the circulating variants at the time the EQA was conducted (4). The Alpha (B.1.1.7) variant, in comparable concentration to the previous EQA (2), was included for consistency as it was part of the panel in the previous SARS-CoV-2 EQA (2). The panel was produced at Charité-Universitätsmedizin Berlin.
Panel preparation, validation, and dispatch
All SARS-CoV-2 samples were isolated from clinical specimens using Vero E6 cells cultivated in Dulbecco’s modified Eagle medium (DMEM), supplemented with 2% fetal calf serum (FCS). HCoV-229E BN_1 (7) was stocked using HUH-7 cells cultured in DMEM, supplemented with 2% FCS. The HCoV-OC43 sample was isolated from a clinical specimen using human bronchial epithelial cells cultivated at the air-liquid interface (ALI) using the PneumaCult ALI medium supplemented with Hydrocortisone, Heparin, Primocin, and Penicillin and Streptomycin.
Inactivation of all samples was performed using a final concentration of 0.05% betapropiolactone (BPL). The virus/BPL mixture was incubated at 4°C for 14–16 h, followed by an incubation at 37°C for 2 h. To confirm successful inactivation of SARS-CoV-2, the samples were passaged three times consecutively in Vero E6 cells, cultured in DMEM supplemented with 2% FCS.
Inactivated samples were diluted to the desired concentration with PBS. Aliquots of 500 µL of each sample were lyophilized in screw-cap vials. The lyophilized samples were shipped to participants at ambient temperature.
All SARS-CoV-2 samples were quantified using the E-gene target in an RT-PCR-based in-house assay (5). Samples positive for HCoV-229E and HCoV-OC43 were quantified using specific RT-PCR-based in-house protocols (6). RT-PCR-based validation of samples was performed at three institutions, namely Charité-Universitätsmedizin Berlin, the National Institute for Public Health and the Environment of the Netherlands, and the Robert Koch Institute, Berlin, independently. The samples were additionally sequenced by one of the institutes. All specimens performed as expected by all three laboratories and were valid for use in the panel.
Data collection
Results were reported via an online survey form (hosted on the EU survey platform). Participants were asked to score their samples (positive, negative, and inconclusive). Furthermore, participating laboratories were asked to give information about cycle threshold (ct) values, extraction method, and types of RT-PCRs (in-house protocol and/or commercial kit) for each target and each sample. In addition, participants could report the determined SARS-CoV-2 variant (by WHO label or Pango lineage) and/or signature mutations, together with information regarding sequencing methods used, if any. Identifying variants and their specific features was an optional activity in this EQA.
Evaluation of results
Results of the molecular detection were scored according to the following system: correctly reported samples (presence or absence of SARS-CoV-2 RNA): 0 points, inconclusive results: 1 point, and false negative or positive results: 2 points. For sequencing results, we differentiated between correctly determined variants/signature mutations, general identification as variant of concern (VOC), and false typing. Providing the correct variant name, Pango classification, or signature mutation(s) were all considered equally correct.
In addition, we compared this EQA with previous ones with regard to the number of participants, EQA participation for the first time, number and type of methods used, and overall performance.
Statistical analysis
Data cleaning and analysis were performed using R (version 4.3.0). Figures were prepared using GraphPad Prism (version 9.0) or R (version 4.3.0).
RESULTS
Participation
Thirty-eight expert laboratories from 31 countries, covering 26 of the 30 EU/EEA countries and 5 of the 7 EU pre-accession countries, reported EQA results (Fig. S1).
Molecular detection of SARS-CoV-2
An overview of the results for the individual samples is shown in Table 1. Regarding the detection of SARS-CoV-2 RNA, 31 of 38 participating laboratories correctly classified all 10 samples, 11% (4/38) classified 9 samples correctly, and 8% (3/38) classified 8 or fewer samples correctly. Of all reported results, 3% (10/380) were incorrect. Among the SARS-CoV-2 containing samples, 1.1% (3/266) were reported as inconclusive and 1.5% (4/266) as negative. Three laboratories (7.9%; 3/38) showed inconclusive results for one or two samples. The three samples with the lowest concentrations (≤70 viral RNA copies [cps]/µL) were not reported as positive by one laboratory (2.6%; 1/38). Two laboratories had false positive results for one sample each (5.2%; 2/38), whereby one laboratory tested the negative control positive, and the other laboratory showed the OC43 containing samples as positive for SARS-CoV-2. Another laboratory indicated the OC43-containing sample as inconclusive.
The ct values of positively tested samples were in general lower with increasing SARS-CoV-2 RNA concentration (Fig. 1). The detected ct values for the individual sample varied depending on the detection target and tests used.
Ct values of SARS-CoV-2 containing samples. Multiple answers per laboratory are included. Shown are median ct values with interquartile range.
SARS-CoV-2 variant typing
Variant typing was reported by 13 participating laboratories. Three laboratories used typing PCRs to identify the variant. Nine laboratories performed sequencing. One laboratory did not specify the method used. The quality of sequencing results was better for samples with higher concentrations of viral RNA (Fig. 2; Table 1). Nine (69%) of 13 laboratories that performed typing identified the highest concentration sample correctly. The samples with the second highest concentration were reported correctly by 46% (6/13). The sample containing B.1.1.7 was correctly identified by three laboratories (27%). Six laboratories (46%) identified this sample as false and reported Omicron variants or mentioned “delta-like” for this sample. For the two samples with the lowest concentrations (12 and 13 cps/µL), 27% (3/13) and 8% (1/13) of the laboratories determined the variant correctly. One laboratory reported all samples to be VOCs without further identifying the specific virus variant (Fig. 2). This laboratory performed typing PCR using the Seegene Allplex SARS-CoV-2 Variants Assay I kit. In addition, two laboratories stated that NGS failed because the quality of the sequences was too low for interpretation. This was mentioned for all SARS-CoV-2 containing samples. Low quality of sequences was also the reason why some laboratories stated “no result” for some samples. For many samples, it was not further defined why typing failed. Different kits were used for sequencing, like the Ion AmpliSeq SARS-CoV-2 Insight Research Assay (Thermo Fisher), the DNA prep kit from Illumina, or the CovidSeq kit from Illumina.
*SARS-CoV-2 variant typing results and overview of typing methods of laboratories participating in the optional typing exercise, European SARS-CoV-2 EQA, 2023. VOC, variant of concern. Specific variant, the SARS-CoV-2 variant or specific mutations were named; unspecific, named as variant but not the specific sublineage; false, wrong VOC was named. , no information given.
Figure 2 provides an overview of used typing methods and the results of the lineage determination per sample by each laboratory.
Comparison with two previous European SARS-CoV-2 EQAs
The number of participating laboratories decreased over time from 68 participants in the first EQA, conducted in 2020, to 38 participants in this EQA. The same institutes were not consistently invited to the EQAs. There was an average of one participating laboratory per country, as compared to two in the previous EQAs (Table 2). In this EQA, 31 countries were represented in comparison to 35 and 34 in the first two EQAs. All participants of the current EQA also participated in the first and/or second EQAs.
In line with increasingly streamlined diagnostics, a high number of laboratories used automated extraction over the course of the three EQAs (79% in the recent EQA). Automated extraction was predominantly done with a magnetic beads-based method, whereas manual extraction was almost entirely spin column-based (Fig. 3A). In all three EQA rounds, a higher number of participating laboratories used commercial (as opposed to in-house) methods for molecular diagnostics (Fig. 3B). The proportion of laboratories using only commercial methods for SARS-CoV-2 detection increased from 40% in 2020 to 55% in 2021, reaching 58% in the current EQA round. Conversely, laboratories using both in-house and commercial methods decreased to 13% in 2023, compared to 29% in 2020 and 25% in 2021, amounting to 71% of participants in 2023 who used commercial assays (Table 2; Fig. 3B). Laboratories used and reported on average a total of two different molecular methods (in-house and/or commercial) in each EQA, ranging from one to five in 2020 and one to four assays in 2021 and 2023, respectively. The targets for in-house assays were predominantly E gene and RdRp (Fig. 3C), whereas targets of commercial assays varied wider between E, N, ORF1ab, RdRp, and S (Fig. 3D). For this EQA, the target detected mostly via in-house assays was RdRp (23.7%) and via commercial assays N (65.8%) (Fig. 3C and D).
Comparison of three EQAs in terms of (A) extraction methods used, (B) molecular methods used, (C) targets detected using in-house assays, and (D) targets detected using commercial assays. Percentage of participating laboratories per corresponding EQA year is visualized.
An overall improvement in SARS-CoV-2 detection was observed over the course of the three EQAs (Table 2; Fig. 4). The percentage of laboratories correctly identifying all samples increased from 12% in 2020 to 75% in 2021, reaching 90% for the current EQA (Table 2). The detection of the variant that was included in the second and this EQA (B.1.1.7) was comparable between the 2021 and the current EQA (72.9–100%; 97%). In 2021, four B.1.1.7 containing samples with concentrations of 2.5, 3, 11, and 290 cps/µL were included in the panel. In the current EQA, one B.1.1.7 containing sample with 120 cps/µL was part of the panel. Other variants of the panel represented the variants circulating at the time of the respective EQA and therefore differed between the years.
Participating laboratories and their penalty points for three European SARS-CoV-2 EQAs. Laboratories participating in multiple EQAs are connected via dashed lines.
Figure 4 shows the number of participating laboratories for all three EQAs and their penalty points, respectively. Over time, the number of participating laboratories decreased. Roughly two-thirds of laboratories that participated in the first EQA also participated in the second EQA. A total of 27 laboratories from 25 countries participated in all three EQAs. Of these, 19 scored less than 100% in 2020. In 2021, 10 laboratories scored less than 100% and in 2023, only 4 laboratories scored below 100%. The evaluation of the individual laboratories over time can be seen in Fig. 4.
DISCUSSION
We hereby report the results of the third European EQA of molecular detection of SARS-CoV-2 and the second that included variant identification, conducted in 2023. Compared to the two previous EQAs (1, 2), fewer laboratories participated. In the first EQA, all EVD-Labnet laboratories as well as influenza contact points were invited. In the course of the pandemic, operational contact points for SARS-CoV-2 were identified. These were the institutes that were invited for the current EQA. Given only a slight decrease in the number of countries represented, now typically only one laboratory per country participated. All laboratories participating in this EQA also participated in the first and/or second EQAs.
Compared with former EQAs, an improvement in performance over time could be detected, starting with 12% of participating laboratories who classified all SARS-CoV-2 containing samples correctly as SARS-CoV-2 RNA positive in 2021 and 75% in 2022. In 2023, 90% of the participating laboratories correctly classified all SARS-CoV-2 containing samples. As expected, reduced molecular detection levels (95%) were only observed for SARS-CoV-2 containing samples with low RNA concentrations (≤13 cps/µL). This was already observed in previous EQAs (1, 2). Here, samples with comparable concentrations (11 and 12.5 cps/µL) were identified correctly by 91.5% and 90–99% of participants (1, 2). However, a lower diagnostic sensitivity for samples with such low SARS-CoV-2 RNA concertation is of limited clinical importance (8, 9). Although higher SARS-CoV-2 RNA concentration showed a lower ct value, it is, however, no quantitative measure. Different laboratories used different assays leading to different ct values for the same sample. To be able to compare the results of different laboratories, truly comparable measures like concentration of viral RNA based on standardized positive controls are indispensable. This fact demonstrates the urgent need for reference material, enabling the comparison between laboratories and quantitative statements.
One laboratory participating in the current EQA reported three SARS-CoV-2 containing samples as false negatives. This laboratory used an in-house assay and classified samples as negative if their ct value was above 42. Two laboratories identified four SARS-CoV-2 containing samples in total as inconclusive with ct values between 36 and 38. Of these laboratories, 50% used an in-house assay and 50% used a commercial kit. The commercial kit was also used by other participating laboratories correctly detecting all SARS-CoV-2-containing samples. Therefore, false negative or inconclusive results were most probably due to extraction procedures and/or pre-RT-PCR workflow. Two laboratories that reported false positive results, both used commercial kits that were also used error-free by other laboratories. As a result, false-positive test results were more likely a consequence of contamination during sample extraction, handling, admin error, or lot-specific contamination of rRT-PCR (real-time reverse transcription PCR) kits or oligonucleotides (1, 2) rather than non-specificity of the RT-PCR. In general, 27 laboratories used eleven different commercial kits. In the current EQA, variant typing of the SARS-CoV-2 positive samples was voluntary, and 34% (13/38) of participants performed typing. Unlike the detection aspect of the EQA, the typing results were quite diverse. Approximately half of the laboratories correctly identified most of the specific SARS-CoV-2 variants. Incorrect or no results were primarily reported for samples with low viral RNA concentrations. As viral load is a major factor influencing sequencing success (10), and low RNA concentrations can both lead to sequencing errors and increase the risk of general test failure (11), these outcomes were as expected. For future EQAs, the design of the samples and their viral load should be reconsidered. Nevertheless, these results indicate a performance gap between the labs especially for low viral content specimens that may need to be addressed, especially given the increasing importance of molecular surveillance of pathogens (12, 13). Genomic pathogen surveillance enables real-time tracking of infection spread across populations. Additionally, it allows for the detection of changes in the pathogen, and presents information that can be used to adjust measures to control a pandemic (14). The results of this EQA were discussed during the ECDC WHO Europe Laboratory Network meeting along with available training opportunities.
To specifically address the issues with variant typing repeated drylab EQAs could be performed. As demonstrated by a pilot EQA focusing on SARS-CoV-2 whole-genome sequencing that was published in early 2022, most participating laboratories generated whole-genome sequences and correctly identified all lineages and clusters; however, coverage across the genome was the most critical aspect, correlating with correct lineage and cluster assignments. Sequencing depths varied by as much as 100-fold and consistent with our EQA findings, many labs in the drylab EQA struggled with a sample that had a lower viral load (ct 28). The main causes of these inconsistencies were missing data, bioinformatic choices, and data interpretation (10).
Our results from three European SARS-CoV-2 EQAs suggest that repeated EQAs can contribute to improved detection capabilities of laboratories. We also observed a shift from in-house tests to more commercial tests and automated extraction systems, which aligns with the establishment of SARS-CoV-2 as an endemic pathogen. This trend might be strengthened by the European IVDR, which favors commercially available CE IVD products for diagnostics. However, such kits are often not available for rare or emerging viruses, nor during the initial phase of a pandemic.
To further improve SARS-CoV-2 genomic surveillance and variant typing, future EQAs should focus on sequencing, as part of wet-lab EQAs shown here, but also additionally via dedicated dry-lab exercises. Increasing the sensitivity of sequencing protocols and the correct interpretation of the sequencing data are crucial for proper variant typing.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Fischer C, Mögling R, Melidou A, Kühne A, Oliveira-Filho EF, Wolff T, Reiche J, Broberg E, Drosten C, Meijer A, Leitmeyer K, Drexler JF, Reusken C. 2021. Variable sensitivity of SARS-Co V-2 molecular detection in european expert laboratories: external quality assessment, June and July 2020. J Clin Microbiol 59:e 02676-20. doi:10.1128/JCM.02676-2033298612 PMC 8106723 · doi ↗ · pubmed ↗
- 2Mögling R, Fischer C, Stanoeva KR, Melidou A, Almeida Campos AC, Drosten C, Biere B, Meijer A, Kraus A, Reusken CBEM, Drexler JF. 2022. Sensitivity of detection and variant typing of SARS-Co V-2 in European laboratories. J Clin Microbiol 60:e 0126122. doi:10.1128/jcm.01261-2236445090 PMC 9769866 · doi ↗ · pubmed ↗
- 3AURORAE. 2024. Laboratory support for influenza and SARS-Co V-2 for Europe: AURORAE. Available from: https://www.rivm.nl/en/international-projects/aurorae
- 4O’Toole Á, Hill V, Pybus OG, Watts A, Bogoch II, Khan K, Messina JP, Tegally H, Lessells RR, Giandhari J, et al.. 2021. Tracking the international spread of SARS-Co V-2 lineages B.1.1.7 and B.1.351/501Y-V 2 with grinch. Wellcome Open Res 6:121. doi:10.12688/wellcomeopenres.16661.234095513 PMC 8176267 · doi ↗ · pubmed ↗
- 5Corman VM, Landt O, Kaiser M, Molenkamp R, Meijer A, Chu DK, Bleicker T, Brünink S, Schneider J, Schmidt ML, Mulders DG, Haagmans BL, van der Veer B, van den Brink S, Wijsman L, Goderski G, Romette J-L, Ellis J, Zambon M, Peiris M, Goossens H, Reusken C, Koopmans MP, Drosten C. 2020. Detection of 2019 novel coronavirus (2019-n Co V) by real-time RT-PCR. Euro Surveill 25:2000045. doi:10.2807/1560-7917.ES.2020.25.3.200004531992387 PMC 6988269 · doi ↗ · pubmed ↗
- 6Owusu M, Annan A, Corman VM, Larbi R, Anti P, Drexler JF, Agbenyega O, Adu-Sarkodie Y, Drosten C. 2014. Human coronaviruses associated with upper respiratory tract infections in three rural areas of Ghana. P Lo S One 9:e 99782. doi:10.1371/journal.pone.009978225080241 PMC 4117488 · doi ↗ · pubmed ↗
- 7Corman VM, Eckerle I, Memish ZA, Liljander AM, Dijkman R, Jonsdottir H, Juma Ngeiywa KJZ, Kamau E, Younan M, Al Masri M, Assiri A, Gluecks I, Musa BE, Meyer B, Müller MA, Hilali M, Bornstein S, Wernery U, Thiel V, Jores J, Drexler JF, Drosten C. 2016. Link of a ubiquitous human coronavirus to dromedary camels. Proc Natl Acad Sci U S A 113:9864–9869. doi:10.1073/pnas.160447211327528677 PMC 5024591 · doi ↗ · pubmed ↗
- 8Wölfel R, Corman VM, Guggemos W, Seilmaier M, Zange S, Müller MA, Niemeyer D, Jones TC, Vollmar P, Rothe C, Hoelscher M, Bleicker T, Brünink S, Schneider J, Ehmann R, Zwirglmaier K, Drosten C, Wendtner C. 2020. Virological assessment of hospitalized patients with COVID-2019. Nature New Biol 581:465–469. doi:10.1038/s 41586-020-2196-x 32235945 · doi ↗ · pubmed ↗