Direct thin-layer agar for bedaquiline-susceptibility testing of Mycobacterium tuberculosis at BSL2 level yields high accuracy in 15 days from sputum processing
I. Cuella-Martin, D. Runyambo, S. De Bock, M. Diels, H. Niyompano, F. Hakizayezu, J. Keysers, W. B. De Rijk, Y. M. Habimana, N. Gahamanyi, E. Ardizzoni, C. M. Muvunyi, B. C. de Jong, J. C. S. Ngabonziza, L. Rigouts

TL;DR
A new method using thin-layer agar for testing drug resistance in tuberculosis from sputum samples is shown to be fast and accurate, especially for bedaquiline.
Contribution
The study introduces a faster and safer (BSL2) direct DST method using thin-layer agar for bedaquiline and other anti-TB drugs from sputum.
Findings
TLA correctly classified all wild-type strains as bedaquiline-susceptible and detected 9 out of 10 resistant strains.
Direct-TLA-DST had a median time to result of 15 days for smear-positive samples, faster than WHO-endorsed methods.
The method achieved high sensitivity and specificity for rifampicin and isoniazid, with no resistance detected for bedaquiline or levofloxacin.
Abstract
This study evaluated thin-layer agar (TLA) as a faster alternative for both indirect minimum inhibitory concentration (MIC) determination of bedaquiline (BDQ) from culture isolates and direct drug-susceptibility testing (DST) from sputum samples. Indirect BDQ-MIC results from TLA were compared to the established 7H11 solid DST. Direct-TLA-DST performance was assessed using 143 baseline sputum samples from rifampicin-resistant TB cases. Direct-TLA tested susceptibility to rifampicin, isoniazid, levofloxacin, and BDQ, with results compared to Löwenstein-Jensen (LJ) and MGIT. For indirect BDQ-MIC determination, TLA accurately identified H37Rv MICs within the WHO control range (0.015–0.12μg/mL). Optimal results were obtained with standard incubation and day 7 reading of the plates. TLA correctly classified all wild-type clinical strains as BDQ-susceptible and detected 9 out of 10…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
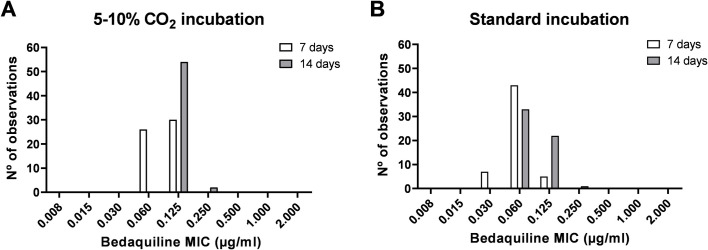 Fig 1
Fig 1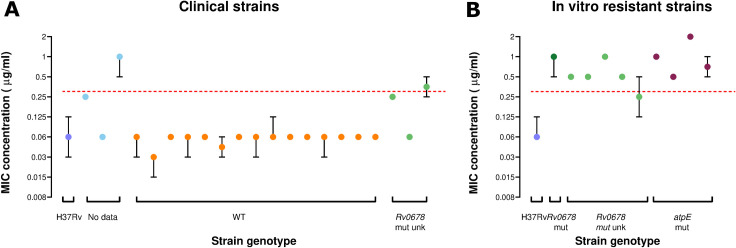 Fig 2
Fig 2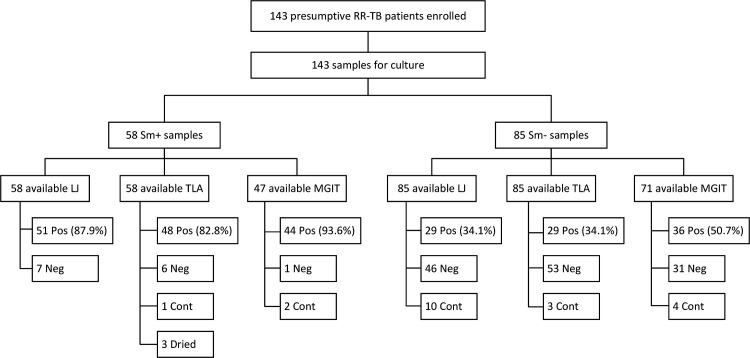 Fig 3
Fig 3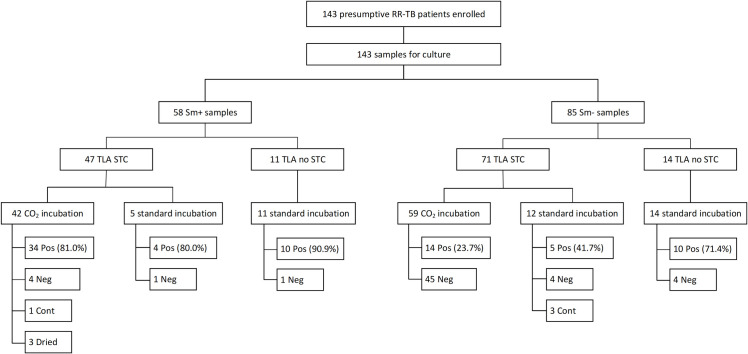 Fig 4
Fig 4| Number (%) of plates with MIC results relative to the 7H11 tube-based testing | ||||||
|---|---|---|---|---|---|---|
| 5-10% CO2 incubator | Standard incubator | |||||
| Reading time | ≤1-fold dilution | ˃1-fold dilution | Not interpretable | ≤1-fold dilution | ˃1-fold dilution | Not interpretable |
| D7 | 112 (90.3%) | 11 (8.9%) | 1 (0.8%) | 121 (97.6%) | 3 (2.4%) | 0 |
| D14 | 91 (73.4%) | 31 (25%) | 2 (1.6%) | 118 (95.2%) | 5 (4%) | 1 (0.8%) |
| Sample ID | Drug tested | Indirect DST | TLA | Sequencing | Final result | In favor of direct-TLA testing |
|---|---|---|---|---|---|---|
| 183 | RIF | R | S | S | Yes | |
| 195 | RIF | S | R | R | Yes | |
| 201 | RIF | S | R | R | Yes | |
| 208 | RIF | R | S | S | Yes | |
| 018 | INH | S | R | R | Yes | |
| 024 | INH | S | R | R | Yes | |
| 100 | INH | R | S | R | No | |
| 143 | INH | S | R | R | Yes | |
| 147 | INH | R | S | R | No | |
| 183 | INH | R | S | WT | S | Yes |
| 200 | INH | R | S | R | No | |
| 201 | INH | S | R | WT | S | No |
| 208 | INH | R | S | NT | R | No |
| 210 | INH | R | S | NT | R | No |
| 143 | LFX | R | S | WT | S | Yes |
| 222 | LFX | R | S | NT | R | No |
| TLA | |||||
|---|---|---|---|---|---|
| DST | Resistant | Susceptible |
| Sensitivity | Specificity |
| RIF-resistant | 40 | 0 |
| 100 (91.2–100) | 100 (87.3–100) |
| INH-resistant | 36 | 5 |
| 87.8 (73.8–95.9) | 96.2 (80.4–99.9) |
| LFX-resistant | 0 | 1 |
| NA | 100 (90.5–100) |
| BDQ-resistant | 0 | 0 |
| NA | 100 (90.8–100) |
- —Fonds Wetenschappelijk Onderzoekhttp://dx.doi.org/10.13039/501100003130
- —Belgian Directorate General Development Coperation and Humanitarian Aid (DGD)
- —Flandre | Departement Economie, Wetenschap en Innovatie (EWI)
- —Belgian Federal Public Service of Development Cooperation (DGD)
- —Fonds Wetenschappelijk Onderzoekhttp://dx.doi.org/10.13039/501100003130
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsTuberculosis Research and Epidemiology · Mycobacterium research and diagnosis · Antibiotics Pharmacokinetics and Efficacy
INTRODUCTION
Management of multidrug-resistant tuberculosis (MDR-TB) is compromised by limited access to drug-susceptibility testing (DST), which is increasingly crucial to optimize care for MDR-TB patients. (1) Since 2020, the World Health Organization (WHO) has included bedaquiline (BDQ) as a core component of any MDR-TB regimen. (2) BDQ is a diarylquinoline antimycobacterial compound that exerts its bactericidal effect by blocking ATP synthesis. (3) Although BDQ is a relatively new drug, increasing rates of resistance are being reported, including among drug-naïve TB patients, which compromises these regimens (4, 5).
Only a few patients who start an all-oral BDQ-based regimen today will have resistance testing done for BDQ, as phenotypic testing requires a BSL3 laboratory, and genotypic testing has not yet been translated to a rapid molecular test, due to the imperfect correlation of a wide range of mutations with phenotypic resistance. Resistance to BDQ has been associated with genetic mutations or resistance-associated variants (RAVs) in the atpE, Rv0678, and pepQ genes (6, 7). In vitro studies indicate that mutations in atpE, the gene encoding BDQ’s direct target ATP synthase, lead to high-level BDQ resistance, although these mutations likely cause significant fitness loss and hence are rarely found in clinical isolates (8–10). By contrast, mutations in the Rv0678 efflux pump regulator gene are linked to low-level BDQ resistance, but only if the efflux pump remains functional (11–14). Mutations in pepQ generally result in a modest increase in BDQ minimum inhibitory concentration (MIC) (13, 15). Given these imperfect genotypic–phenotypic associations, phenotypic DST (pDST) remains the reference test to effectively guide treatment and monitor the emergence of BDQ resistance.
The current guidelines for phenotypic BDQ-susceptibility testing are based on limited evidence. (16) Although MIC determination using Middlebrook 7H10 or 7H11 agar and 7H9 broth microdilution method (BMD) has been validated in a multicountry study, solid media-based DST is restricted to polystyrene tubes, due to the strong binding of BDQ to polypropylene; and time-consuming, often requiring 3–4 weeks to yield results after a positive primary culture is obtained (17, 18). Liquid-based methods, such as the Mycobacteria Growth Indicator Tube (MGIT) system, are recommended for their higher sensitivity and faster turnaround times. (19) However, all these methods require BSL3 biosafety infrastructure and equipment, limiting decentralized access, particularly where specimen transport systems to centralized laboratories are inadequate.
Thin-layer agar (TLA) offers a simpler and more affordable alternative for isolating the Mycobacterium tuberculosis (MTB) complex and detecting drug resistance directly from sputum samples. TLA has demonstrated comparable performance to conventional methods, such as the MGIT system, for MTB isolation and sensitivity and specificity for the detection of rifampicin (RIF) and isoniazid (INH) resistance (20, 21). TLA’s one-step approach involves direct inoculation of processed sputum samples onto solid culture plates that are sealed and not reopened during the remainder of the procedure, minimizing the risk of aerosolization or leakage and making TLA, similar to other direct DST methods, a suitable option for use in moderate-risk (biosafety level 2, BSL2) laboratories (22, 23). However, the use of TLA for BDQ testing has not been documented.
This study aimed (1) to validate the performance of the TLA as an indirect method for BDQ-MIC determination, comparing it with the standard tube-based 7H11 MIC method and (2) to evaluate the performance of direct TLA-DST under various conditions for MTB isolation and pDST for BDQ, along with RIF, INH, and levofloxacin (LFX), in comparison to solid and liquid culture followed by indirect pDST.
MATERIALS AND METHODS
Indirect TLA-BDQ-MIC validation
Twenty-one clinical MTB isolates and 10 in vitro-selected strains obtained from the collection at the Institute of Tropical Medicine (ITM) in Antwerp, Belgium, were used for validation of indirect TLA-MIC determination for BDQ (TLA-BDQ-MIC) (Table S1). This selection included isolates with a wide range of MIC values. Of the 21 clinical isolates, WGS data were available for 18, of which all had a wild-type atpE gene, while three had a mutation in the Rv0678 gene. Four of the 10 in vitro-selected strains presented a mutation in atpE and six in Rv0687. The MTB H37Rv reference strain (ITM 500735) was included as a BDQ-susceptible control strain. All isolates were freshly subcultured on a Löwenstein-Jensen (LJ) medium before being tested.
A bacterial suspension prepared from fresh MTB growth on LJ was adjusted to a turbidity of McFarland standard No. 1 and further diluted 1:10 in sterile distilled water. Using a sterile transfer pipette, one drop (~50 µL) was inoculated into each of the 12 wells of an in-house prepared TLA plate (Corning Costar 3513; Sigma-Aldrich, USA), except for the negative control (NC) well. Two operators independently performed the inoculation in duplicate, starting from a different bacterial suspension, for a total of 4 replicates. Each plate consisted of one well for growth control (GC), one well for p-nitrobenzoic acid (PNB) at 500 µg/mL to differentiate between MTB complex and non-tuberculous mycobacteria (NTM), one well for the NC, and one well for each serial concentration of BDQ: 0.008, 0.015, 0.03, 0.06, 0.125, 0.25, 0.5, 1 and 2 µg/mL. BDQ powder was obtained from Janssen Pharmaceuticals, Belgium, batch 16175328. To prepare the plates, Middlebrook 7H11 agar base (212203, Becton Dickinson, USA) was mixed with glycerol 86%–89% and sterile distilled water as per the manufacturer’s instruction. After autoclaving and cooling down to 55°C, the medium was supplemented with oleic acid dextrose catalase (OADC, 212240, Becton Dickinson) plus the antibiotics amphotericin, piperacillin, and trimethoprim (Sigma-Aldrich), all at 4 µg/mL concentration. Parallel MIC determination on 7H11 agar medium enriched with OAD supplement in polystyrene tubes was performed, using the same BDQ concentrations. (19) After inoculation, parallel plates were placed in a 34°C–38°C incubator with ambient CO_2_ concentrations or supplemented with 5%–10% CO_2_, while tubes were always incubated with 5%–10% CO_2_. TLA plates were read on days 7 (D7) and 14 (D14) by two independent operators using a conventional light microscope (objective 10×). Growth in the GC well paired with the absence of growth in the PNB well was considered positive for MTB. The MIC was interpreted if at least 10 colonies were present in the GC. MIC results corresponded to the well with the lowest drug concentration that did not show growth, that is, 100% inhibition. For tube-based 7H11 MIC testing, reading was done at 4 weeks, and the MIC_99_ was determined as the highest concentration that had less growth than the 1/100 diluted GC tube.
Direct on sputum TLA-DST
We collected sputum samples from consecutive patients diagnosed with pulmonary rifampicin-resistant (RR-) TB by GeneXpert MTB/RIF (Ultra) who were registered in the MDR-TB Clinic in Kabutare between December 2021 and December 2023 and who consented to participate in the study. Three sputum samples were collected before starting RR-TB treatment: the first on the day of arrival (spot sample 1), the second collected overnight (sample 2; sputum accumulated in the same container throughout the night), and the third on the following day (spot sample 3). All three samples were sent together on the day the third sample was obtained, using a cool box maintained at approximately 4°C, to the National Reference Laboratory (NRL) in Kigali, Rwanda, for further genotypic and phenotypic testing. To minimize contamination risk, samples were processed promptly upon arrival. After NaOH-Nalc decontamination, the three samples underwent Auramine-O microscopy. In addition, sample 2 was used for primary culture on homemade LJ and in the automated MGIT, and sample three for a second primary culture (LJ and MGIT) and parallel direct-TLA-DST. To ensure consistency and comparability across methods, only results from sample 3 were included in the analysis of contamination and performance for LJ, MGIT, and TLA methods. This approach involved matching sample IDs across the methods to align the data set. Leftovers of the three sediments were stored at −20°C. Subsequent pDST for positive LJ or MGIT cultures was done either by the 1% proportion method on LJ medium against first-line TB drugs or, since October 2022, by MGIT-DST including first-line drugs, BDQ, and levofloxacin (LFX). Direct-TLA testing was performed using the same 12-well plates (Corning Costar 3513; Sigma-Aldrich, USA) and 7H11 agar medium supplemented with a broad-spectrum antibiotic mixture (i.e., OADC, amphotericin, piperacillin, and trimethoprim) to suppress contamination, mirroring the procedures previously detailed at ITM. In addition, some plates were prepared with the addition of the redox indicator 2,3-diphenyl-5-(2-thienyl) tetrazolium chloride (STC; Merck, USA) at a final concentration of 50 µg/mL, which was incorporated into the medium after cooling down to potentially facilitate plate reading and interpretation of observed (early) growth. (24) To ensure the quality and consistency of each batch of in-house prepared plates, a quality control check was performed by inoculating H37Rv and Mycobacterium fortuitum. Each 12-well plate could accommodate two samples with for each sample a drug-free GC and wells containing each PNB (500 µg /mL), RIF (1.0 µg /mL), INH (0.2 µg /mL), LFX (1.0 µg/mL), or BDQ (0.25 µg/mL). The processed sputum sediments were resuspended in 2 mL of phosphate-buffered saline (PBS). A sterile transfer pipette was used to inoculate approximately 50 µL (one drop) of the resuspended sample into each TLA well. Plates were incubated at 34°C–38°C in a CO_2_-enriched environment, generated using a candle jar, and visually examined without opening on days 7, 14, 21, 28, and 35, or the nearest available day if deviations from the schedule occurred. From May 2023 onward, TLA plates were incubated under standard incubation conditions without CO2 supplementation. Results were interpreted on the day of GC positivity. A positive result for MTB was defined by the absence of growth in the PNB well, while drug resistance was indicated by any growth in drug-containing wells. Discrepancies across all drug results between direct-TLA-DST and indirect DST performed on LJ or MGIT were resolved through gene sequencing. Sanger sequencing of the rpoB gene was conducted on residual sputum or sediment samples (second or third sample) that were shipped to the Institute of Tropical Medicine (Antwerp, Belgium). (25) In addition, sequencing of the katG and fabG-inhA genes was performed to assess isoniazid (INH) resistance. Whole-genome sequencing (WGS) was performed on genomic DNA extracted from isolates using the Illumina HiSeq platform (CD Genomics, USA) to further resolve discrepancies for INH, LVX, and BDQ(6). In cases where sequencing data were unavailable to resolve discrepancies, the results from indirect pDST were considered the definitive result.
Statistical analysis
A Chi-square test with Yates’ continuity correction was conducted to compare the accuracy of TLA-BDQ-MIC results across different incubation environments and reading times. In addition, a Z-test for proportions was employed to evaluate the significance of differences in result reliability when comparing standard incubator readings at day 7 to other conditions. The MTB positivity rate for direct TLA-DST was determined by dividing the number of samples exhibiting MTB by the total samples tested. Different conditions for the direct TLA method were compared by Fisher’s exact test using LJ results as a baseline through the Mantel-Haenszel chi-squared test. TLA results were compared with those from LJ or MGIT using matched sample IDs and the Z proportion method, which was adjusted for multiple comparisons with a Bonferroni post hoc correction. Sensitivity and specificity, along with their corresponding 95% confidence intervals (CI), were calculated for TLA in detecting resistance to RIF, INH, LFX, and BDQ, using LJ and MGIT as reference standards, based on availability. All statistical analyses were conducted using R software, version 4.1.0, with a significance level set at 0.05.
RESULTS
Indirect TLA-BDQ-MIC validation
For the H37Rv strain, BDQ-MIC values were slightly elevated under 5%–10% CO_2_ incubation with a mode of 0.125 μg/mL and a range of 0.060–0.125 μg/mL, compared to a mode of 0.060 μg/mL and a range of 0.030–0.125 μg/mL under standard incubation conditions (Fig. 1). In both incubation environments, a trend toward higher MIC values was observed at the D14 reading compared to D7. Notably, among all H37Rv replicates, only one plate exhibited contamination at day 7 in the standard incubator, accounting for 0.9% (1/112).
MIC distribution of bedaquiline for 56 replicates of the M. tuberculosis H37Rv reference strain on thin-layer agar plates incubated in parallel at various conditions, with readings after 7 days and 14 days.
For the 21 clinical isolates and 10 in vitro-resistant strains analyzed, TLA-BDQ-MIC determination was influenced by both the incubation environment and the reading time (Table 1). Results obtained from the standard incubator demonstrated significantly greater accuracy compared to the reference 7H11-tube testing than those from the 5%–10% CO_2_ incubator, both at D7 (χ² =4.54, P = 0.033) and D14 (χ² =20.57, P < 0.001). The findings indicate that utilizing the standard incubator and conducting readings on day 7 improved the reliability of TLA-BDQ-MIC results, making this combination the preferred approach for optimal accuracy (Z = 2.38, P = 0.017) (Table 1). Of the 248 TLA plates, only 1 (0.40%) plate at D7 and 3 (1.21%) plates at D14 exhibited partial contamination, preventing the interpretation of the MIC results.
Under optimal conditions with standard incubation and reading at D7, TLA correctly identified all wild-type clinical strains as BDQ-susceptible (Fig. 2). In addition, 9 of 10 BDQ-resistant strains were accurately detected, as they exhibited elevated MICs using the TLA method. One strain, carrying an Rv0678 mutation of unknown significance, had a median MIC distribution that aligned with the proposed critical concentration for BDQ (median [95% CI]: 0.25 [0.125–0.5]).
BDQ MIC median distribution of replicates with 95% CI of (A) 21 clinical M. tuberculosis isolates and (B) 10 in vitro-resistant strain, tested by indirect thin-layer agar with standard incubation and reading at 7 days, stratified by genetic profile coded by color. H37Rv is included as a control. The WHO proposed critical concentration for BDQ on 7H11 agar is marked with a dashed line at 0.25 µg/mL. WT: wild type. Rv0678 mut unk: mutation in the Rv0678 gene that is either not associated with BDQ resistance or not listed in the second edition of the WHO mutation catalog. Rv0678 mut: mutation in the Rv0678 gene that is associated with BDQ resistance. atpE mut: mutation in the atpE gene that is associated with BDQ resistance.
Direct TLA-DST
From December 2021 to December 2023, a total of 143 sputum samples were received at the NRL in Rwanda from patients nationwide with a positive RR-TB result from the GeneXpert test conducted at local health facilities (Fig. 3). The overall culture positivity rates prior to treatment start were 53.8% (77/143) for TLA, 55.9% (80/143) for LJ, and 69.4% (75/108) for MGIT. Among the 58 smear-microscopy-positive (sm+) samples, TLA’s performance in isolating MTB was comparable to LJ (82.8% vs. 87.9%; P = 0.43) and MGIT (82.8% vs. 93.6%; P = 0.093). For 85 smear-negative (sm-) samples, TLA performed equally to LJ (34.1% vs 34.1; P = 1.000) and MGIT (34.1% vs 50.7%; P = 0.055). TLA had a lower incidence of uninterpretable results (4.9%) compared to LJ (7.0%) and MGIT (5.1%), although this difference was not statistically significant. Uninterpretable TLA results were primarily due to contamination (4 cases) or medium drying (3 cases), the latter attributed to the candle proximity during incubation. By contrast, LJ and MGIT encountered contamination as the primary issue.
Sensitivity of direct-TLA-DST for primary MTB isolation by smear grade compared with other media. RR-TB: rifampicin-resistant tuberculosis. Sm+: smear-microscopy-positive samples. Sm-: smear-microscopy-negative samples. LJ: Löwenstein-Jensen medium. TLA: thin-layer agar. MGIT: Mycobacteria Growth Indicator Tube. Pos: culture positive. Neg: culture negative. Cont: culture contaminated.
For sm+ samples, TLA’s median time to MTB primary growth was 15 days (IQR 12–21), comparable to MGIT’s 14 days (IQR 10–23.5) and significantly faster than LJ’s 26 days (IQR 21–32). For sm− samples, TLA achieved MTB growth in a median time of 22 days (IQR 20–27), compared to 25.5 days for MGIT (IQR 19.5–32.75) and 44 days for LJ (IQR 30–55.5). Since TLA provided pDST results simultaneously with MTB isolation, it outperformed the other two culture-based pDST methods.
Among the conditions assessed in the TLA methodology, the incubation method did not exhibit a statistically significant effect on plates containing STC, regardless of smear status (P = 1 for sm +samples and P = 0.28 for sm− samples) (Fig. 4). By contrast, when comparing STC-containing plates to those without STC, the latter exhibited significantly better MTB isolation rates in sm− samples, achieving 71.4% versus 27% for STC plates (P = 0.0037). However, this distinction was less pronounced in smear-positive samples, where non-STC plates achieved 90.9% isolation rates compared to 80.9% for STC plates (P = 0.67). Further comparisons between the three experimental conditions, using LJ culture as a baseline, indicated that observed differences across conditions were unlikely to be due to random variation (P = 0.027 for sm+ samples and P < 0.001 for sm− samples).
Flowchart showing enrolled patients and samples for direct-TLA-DST evaluation, stratified by smear-microscopy, STC addition, and TLA plate incubation conditions. RR-TB: rifampicin-resistant tuberculosis. Sm+: smear-microscopy-positive samples. Sm−: smear-microscopy-negative samples. TLA: thin-layer agar. STC: 2,3-diphenyl-5-(2-thienyl) tetrazolium chloride. Pos: culture positive. Neg: culture negative. Cont: culture contaminated. NI: non-interpretable
Of the 77 samples that showed growth in direct-TLA-DST, 67 had reference pDST results for comparison: 29 by LJ and 38 by MGIT. The specificity of TLA compared to indirect DST was 93.6% for RIF, 85.7% for INH, and 100% for both LFX and BDQ. The sensitivity was 95% for RIF and 84.6% for INH, while the sensitivity for LFX and BDQ could not be assessed due to the absence (BDQ) or an insufficient number (LFX) of resistant strains in the cohort. When discrepancies between direct-TLA and either indirect-MGIT or -LJ DST were examined against the reference standard, 13 out of 16 discordant results (81%) were resolved, with 9 (69%) favoring TLA (Table 2). The adjusted sensitivity for direct-TLA-DST was 100% for RIF and 87.8% for INH, while the specificity was 100% for all drugs, except INH (96.2%) (Table 3).
DISCUSSION
Based on our findings, TLA performs well for indirect BDQ-MIC determination, as well as direct tests for MTB isolation and DST for BDQ and other anti-TB drugs against established pDST methods on LJ and in MGIT.
The BDQ-MIC values observed for the H37Rv strain by indirect-TLA confirmed its technical accuracy, with MICs consistently falling below the tentative CC of 0.25 μg/mL, and 99% inside the reference MIC quality control (QC) range for BDQ (0.015 to 0.12 μg/mL) (16, 18). For indirect testing, TLA-based MIC determination saves time and consumables over tube-based MIC determination (solid 7H11 or, by inference, liquid MGIT tubes), with the reading at D7 showing optimal results. Moreover, the standard incubator outperformed the 5%–10% CO_2_ incubator, further enhancing the feasibility of adopting TLA in routine diagnostic settings. While prior studies suggested that CO_2_ incubation might reduce the time to detection, our study found no significant difference in timing between the two methods, with results reliably available by day 7 in both conditions (26).
TLA’s performance for MTB isolation and direct DST was further validated in this study. Consistent with previous research, TLA showed a high positivity rate for MTB detection in smear-positive samples, closely matching the 83% positivity rate reported by other studies (27, 28). In smear-negative samples, TLA could isolate MTB comparably to LJ yet lower than MGIT, although the rate of uninterpretable results due to contamination was low. The low contamination rates and short detection times associated with TLA highlight its suitability for use in settings where rapid diagnosis—and potentially treatment follow-up—is essential for optimal patient management. Furthermore, by transitioning from a CO_2_-enriched candle jar to standard incubation, we addressed the drying issues of plates that contributed to uninterpretable results. Even with the drying plates, the rate of uninterpretable results in TLA was lower than in the compared methods, although this difference was not statistically significant. Had these technical challenges been avoided, a more pronounced difference between the methods could have been observed. This adjustment not only enhances TLA’s reliability but also its potential scalability to peripheral laboratories.
Direct-TLA-DST proved highly effective in detecting RIF resistance, showing robust sensitivity and specificity (20, 21). However, the performance in detecting isoniazid (INH) resistance was somewhat lower than anticipated, with some unresolved discrepancies. Nonetheless, TLA’s ability to rapidly exclude INH resistance remains a key strength of the method.
This study is also the first to evaluate TLA as a direct method for detecting LFX and BDQ resistance. Although sensitivity could not be assessed due to an insufficient number of resistant samples, the high specificity observed for these drugs demonstrates TLA’s potential as a rapid diagnostic tool for ruling out extensively drug-resistant TB (XDR-TB) cases, representing a significant advancement for guiding MDR-TB treatment.
Our study presented some limitations. The relatively small sample size used to evaluate the TLA-BDQ-MIC should be expanded to include a broader range of MTB complex lineages, as lineages L5 to L10 were not represented. In the clinical setting, the stockout of reagents and the use of three different experimental conditions for direct TLA-DST led to data stratification, which may have affected the interpretation of the results. Moreover, while TLA performed well in detecting resistance in susceptible cases, the limited number of resistant isolates for BDQ and LFX prevented a comprehensive assessment of TLA’s sensitivity to detect resistance to these drugs. Finally, some discrepancies between DST methods remain unresolved, highlighting the need for further investigations into the underlying causes of discordant results.
Overall, the results of this study contribute to the growing evidence supporting TLA as a valuable tool to rapidly diagnose resistance to BDQ in BSL2-level decentralized conditions. TLA’s ability to deliver accurate results within a short timeframe, combined with its simplicity, makes it an attractive option for rapid pDST of BDQ in laboratories with moderate biosafety requirements (level 2). Incorporating growth-enhancing components into the medium and/or increasing the inoculum volume could further improve TLA’s diagnostic efficacy, particularly for smear-negative samples (29, 30). Additional research is required to validate TLA’s performance for BDQ sensitivity and extend its application to other new and repurposed anti-TB drugs.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Global tuberculosis report. 2022 Available from: https://www.who.int/publications/i/item/9789240061729
- 2WHO consolidated guidelines on tuberculosis: module 4: treatment: drug-resistant tuberculosis treatment. 2020. Available from: https://www.who.int/publications-detail-redirect/978924000704810.3760/cma.j.cn 112147-20200709-0078633832022 · doi ↗ · pubmed ↗
- 3Andries K, Verhasselt P, Guillemont J, Göhlmann HWH, Neefs J-M, Winkler H, Van Gestel J, Timmerman P, Zhu M, Lee E, Williams P, de Chaffoy D, Huitric E, Hoffner S, Cambau E, Truffot-Pernot C, Lounis N, Jarlier V. 2005. A diarylquinoline drug active on the ATP synthase of Mycobacterium tuberculosis. Science 307:223–227. doi:10.1126/science.110675315591164 · doi ↗ · pubmed ↗
- 4Veziris N, Bernard C, Guglielmetti L, Le Du D, Marigot-Outtandy D, Jaspard M, Caumes E, Lerat I, Rioux C, Yazdanpanah Y, Tiotiu A, Lemaitre N, Brossier F, Jarlier V, Robert J, Sougakoff W, Aubry A, CNR My RMA and the Tuberculosis Consilium of the CNR My RMA, CNR My RMA and Tuberculosis Consilium of the CNR My RMA. 2017. Rapid emergence of Mycobacterium tuberculosis bedaquiline resistance: lessons to avoid repeating past errors. Eur Respir J 49:1601719. doi:10.1183/13993003.01719-201628182568 · doi ↗ · pubmed ↗
- 5Ghajavand H, Kargarpour Kamakoli M, Khanipour S, Pourazar Dizaji S, Masoumi M, Rahimi Jamnani F, Fateh A, Siadat SD, Vaziri F. 2019. High prevalence of bedaquiline resistance in treatment-naive tuberculosis patients and verapamil effectiveness. Antimicrob Agents Chemother 63:e 02530-18. doi:10.1128/AAC.02530-1830602521 PMC 6395892 · doi ↗ · pubmed ↗
- 6Catalogue of mutations in Mycobacterium tuberculosis complex and their association with drug resistance, 2nd ed. 2023 Available from: https://www.who.int/publications-detail-redirect/9789240082410
- 7Kadura S, King N, Nakhoul M, Zhu H, Theron G, Köser CU, Farhat M. 2020. Systematic review of mutations associated with resistance to the new and repurposed Mycobacterium tuberculosis drugs bedaquiline, clofazimine, linezolid, delamanid and pretomanid. J Antimicrob Chemother 75:2031–2043. doi:10.1093/jac/dkaa 13632361756 PMC 7825472 · doi ↗ · pubmed ↗
- 8Zimenkov DV, Nosova EY, Kulagina EV, Antonova OV, Arslanbaeva LR, Isakova AI, Krylova LY, Peretokina IV, Makarova MV, Safonova SG, Borisov SE, Gryadunov DA. 2017. Examination of bedaquiline- and linezolid-resistant Mycobacterium tuberculosis isolates from the Moscow region. J Antimicrob Chemother 72:1901–1906. doi:10.1093/jac/dkx 09428387862 · doi ↗ · pubmed ↗