Impact of High Risk of Obstructive Sleep-Disordered Breathing on School Performance in Pediatric Age Group: A Cross-Sectional Study
Ibrahim Sumaily, Walaa H Algadhi, Alyaj Hakami, Nirmin H Alhazmi, Khalid A Madkhali, Abdulrahman M Yaseen, Maisa A Baiti

TL;DR
This study shows that children with a high risk of obstructive sleep-disordered breathing tend to perform worse in school, especially boys.
Contribution
The study establishes a strong correlation between obstructive sleep-disordered breathing and poor academic performance in children.
Findings
Children with high risk of OSDB had significantly lower academic grades.
The prevalence of OSDB was higher in males compared to females.
A strong negative correlation was found between PSQ-SRBD scores and academic performance.
Abstract
Background We investigated the effects of high risk of obstructive sleep-disordered breathing (OSDB) on school performance in children aged six to 18 years in the Jazan region of Saudi Arabia. Methodology In this cross-sectional study, data were collected using an online questionnaire, which included questions on sociodemographic details, pediatric sleep questionnaire-sleep-related breathing disorder (PSQ-SRBD) scale, and academic performance metrics. Statistical analyses were performed to determine the associations between high risk of OSDB and academic achievements. Results The study sample comprised 145 (52%) males and 176 (48%) females, with a significant prevalence of OSDB (31.58%). The results indicated a negative correlation between PSQ-SRBD scores and academic grades, with correlation values ranging from -0.28 to -0.369 (p < 0.001). Children with high risk of OSDB were more…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
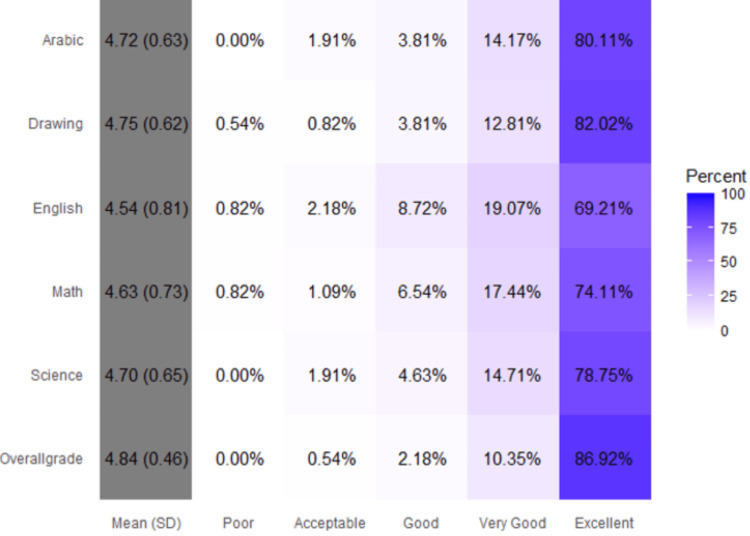 Figure 1
Figure 1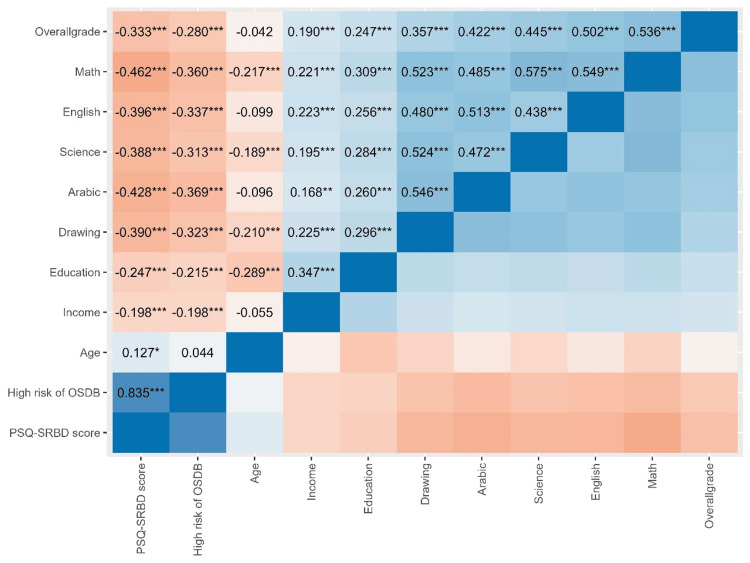 Figure 2
Figure 2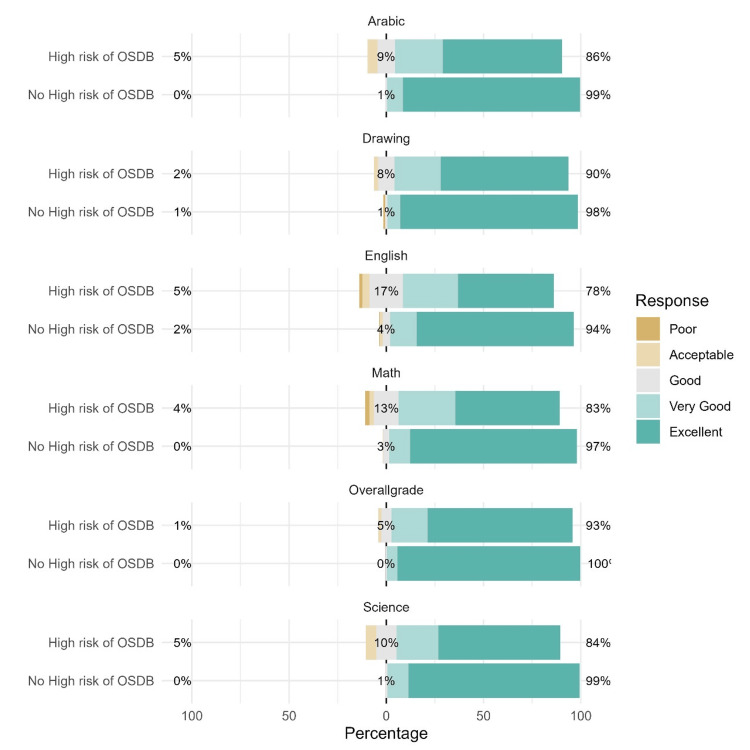 Figure 3
Figure 3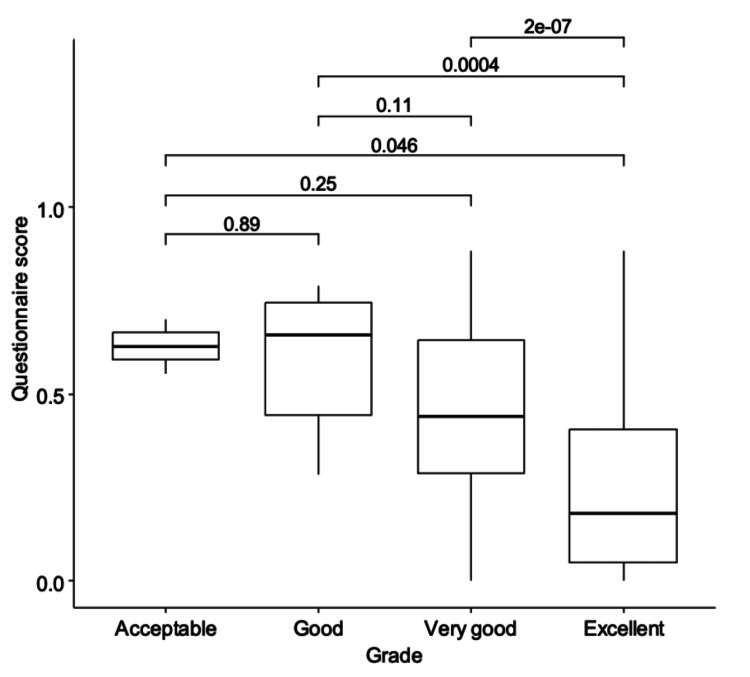 Figure 4
Figure 4| N = 367 | |
| Age (years (±SD)) | 10.8 (3.47) |
| Sex | |
| Male (N (%)) | 191 (52.0%) |
| Female (N (%)) | 176 (48.0%) |
| School level | |
| Primary elementary | 145 (39.5%) |
| Upper elementary | 97 (26.4%) |
| Intermediate | 81 (22.1%) |
| Secondary | 44 (12.0%) |
| Father education level | |
| Illiterate | 8 (2.18%) |
| General education | 80 (21.8%) |
| Bachelor’s degree | 251 (68.4%) |
| Master/PhD | 28 (7.63%) |
| Mother education level | |
| Illiterate | 28 (7.63%) |
| General education | 103 (28.1%) |
| Bachelor’s degree | 224 (61.0%) |
| Master/PhD | 12 (3.27%) |
| Monthly income | |
| <10,000 SAR | 88 (24.0%) |
| 10,000-20,000 SAR | 174 (47.4%) |
| 20,000-40,000 SAR | 74 (20.2%) |
| >40,000 SAR | 31 (8.45%) |
| Variable | N (%) |
| Bronchial asthma | |
| No | 304 (82.8%) |
| Yes | 63 (17.2%) |
| Cardiac | |
| No | 361 (98.4%) |
| Yes | 6 (1.63%) |
| Other chronic diseases | |
| No | 355 (96.7%) |
| Yes | 12 (3.27%) |
| No chronic disease | |
| No | 75 (20.4%) |
| Yes | 292 (79.6%) |
| Total day + night sleeping hours | |
| <9 hours | 162 (44.1%) |
| >9 hours | 205 (55.9%) |
| Total night sleeping hours | |
| <9 hours | 262 (71.4%) |
| >9 hours | 105 (28.6%) |
| Child sleeping time | |
| Before 10 PM | 118 (32.2%) |
| After 10 PM | 249 (67.8%) |
| No ODSB | ODSB | Test statistics | Overall p-value | |
| N = 233 | N = 134 | |||
| Age | 10.0 (8.00; 13.0) | 11.0 (8.00; 14.0) | 8.48 (mean square) | 0.395 |
| Sex | 10.97 (chi-square) | 0.001 | ||
| Male | 106 (45.5%) | 85 (63.4%) | - | - |
| Female | 127 (54.5%) | 49 (36.6%) | - | - |
| School level | 1.498 (chi-square) | 0.683 | ||
| Primary elementary | 93 (39.9%) | 52 (38.8%) | - | - |
| Upper elementary | 65 (27.9%) | 32 (23.9%) | - | - |
| Intermediate | 50 (21.5%) | 31 (23.1%) | - | - |
| Secondary | 25 (10.7%) | 19 (14.2%) | - | - |
| Nasal condition | ||||
| Nasal obstruction | 0.00 (0.00; 0.00) | 0.50 (0.00; 3.00) | 171.417 (mean square) | <0.001 |
| Nasal discharge | 0.00 (0.00; 1.00) | 1.00 (0.00; 2.00) | 88.319 (mean square) | <0.001 |
| Recurrent sore throat | 0.00 (0.00; 1.00) | 2.00 (1.00; 3.00) | 145.176 (mean square) | <0.001 |
| Decreased hearing | 0.00 (0.00; 0.00) | 0.00 (0.00; 2.00) | 73.492 (mean square) | <0.001 |
| Hyponasality | 0.00 (0.00; 0.00) | 1.00 (0.00; 3.00) | 208.378 (mean square) | <0.001 |
| Chronic conditions | ||||
| Bronchial asthma | 24 (10.3%) | 39 (29.1%) | 21.155 (chi-square) | <0.001 |
| Cardiac | 3 (1.29%) | 3 (2.24%) | 0.479 (chi-square) | 0.673 |
| Other chronic diseases | 3 (1.29%) | 9 (6.72%) | 7.927 (chi-square) | 0.011 |
| No chronic disease | 207 (88.8%) | 85 (63.4%) | 33.778 (chi-square) | <0.001 |
| Total day + night sleeping hours | 0.473 (chi-square) | 0.563 | ||
| <9 hours | 106 (45.5%) | 56 (41.8%) | - | - |
| >9 hours | 127 (54.5%) | 78 (58.2%) | - | - |
| Total night sleeping hours | 0.025 (chi-square) | 0.969 | ||
| <9 hours | 167 (71.7%) | 95 (70.9%) | - | - |
| >9 hours | 66 (28.3%) | 39 (29.1%) | - | - |
| Child sleeping time | 5.298 (chi-square) | 0.029 | ||
| Before 10 PM | 65 (27.9%) | 53 (39.6%) | - | - |
| After 10 PM | 168 (72.1%) | 81 (60.4%) | - | - |
| Monthly income | 16.227 (chi-square) | 0.001 | ||
| <10,000 SAR | 44 (18.9%) | 44 (32.8%) | - | - |
| 10,000-20,000 SAR | 108 (46.4%) | 66 (49.3%) | - | - |
| 20,000-40,000 SAR | 59 (25.3%) | 15 (11.2%) | - | - |
| >40,000 SAR | 22 (9.44%) | 9 (6.72%) | - | - |
| Parent’s education | 17.454 (chi-square) | <0.001 | ||
| None has a bachelor’s degree | 23 (9.87%) | 30 (22.4%) | - | - |
| One has a bachelor’s degree or higher | 65 (27.9%) | 48 (35.8%) | - | - |
| Both have a bachelor’s degree or higher | 145 (62.2%) | 56 (41.8%) | - | - |
| Predictors | Odds ratio | 95% CI | p |
| Parent’s education level (one level increase) | 1.74 | 1.08-2.82 | 0.023 |
| Monthly income | |||
| <10,000 SAR | Ref | - | - |
| 10,000-20,000 SAR | 2.28 | 1.04-5.00 | 0.038 |
| 20,000-40,000 SAR | 2.57 | 0.75-8.82 | 0.134 |
| Monthly income: >40,000 SAR | 1.65 | 0.47-5.74 | 0.432 |
| Risk of OSDB (high vs. low) | 0.23 | 0.11-0.47 | <0.001 |
| Gender: female | 0.98 | 0.50-1.92 | 0.945 |
| School level | |||
| Primary elementary | - | - | - |
| Upper elementary | 0.76 | 0.33-1.75 | 0.520 |
| Intermediate | 1.00 | 0.42-2.39 | 0.992 |
| Secondary | 1.60 | 0.50-5.13 | 0.431 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsSleep and related disorders · Obstructive Sleep Apnea Research · Youth Substance Use and School Attendance
Introduction
Obstructive sleep apnea (OSA) is a sleep disorder defined by the American Thoracic Society (ATS) as “a breathing disorder during sleep characterized by prolonged partial upper airway obstruction and/or intermittent complete obstruction (obstructive apnea) that disrupts normal ventilation during sleep and normal sleep patterns” [1]. The prevalence of obstructive sleep apnea syndrome (OSAS) in the pediatric population is approximately 2-4% in Western countries [2]. Although the pathogenesis of adult OSAS has been the subject of numerous studies, several aspects in children still remain unclear. However, several risk factors may contribute to the etiopathogenesis of OSAS, one of the most important risk factors for obesity [3]. Children who are overweight or obese have a higher chance of developing OSAS than those with normal weight [4].
Other risk factors include adenoid and/or tonsil hypertrophy and allergic rhinitis [5,6]. Moreover, craniofacial abnormalities can also cause upper airway obstruction syndrome and some genetic syndromes [7,8]. In addition, moderate-to-severe high risk of obstructive sleep-disordered breathing (OSDB) and snoring also affect the neurocognitive function in children by affecting developing capabilities, as illustrated by cognitive measures in a severity-graded manner. Sleep-disordered breathing (SDB) can adversely impact the academic achievement of children [9].
In 2016, a study published in the USA between October 2006 and October 2014, included 1,010 children aged five to seven years from public schools and broader communities. They found that children’s abilities to achieve academic and adaptive goals may be adversely affected by SDB, which could ultimately hinder their ability to become independent. Their results highlighted the need for SDB awareness, with a focus on children with severe high risk of OSDB [9].
However, no studies have addressed this issue in Jazan. Therefore, we aimed to investigate the impact of high risk of OSDB on school performance among school-aged children in the Jazan region of Saudi Arabia.
Materials and methods
Study design
This cross-sectional case-control study included pediatric patients with high risk of OSDB in Jazan, Saudi Arabia, a hugely populated region with approximately two million people.
Study tool and data collection
We used an online questionnaire distributed via local social media with a link directing participants to the digital version of the questionnaire, which had three parts (Appendices). The first included questions on socio-demographic data, such as sex, age, educational level, salary, parents’ educational levels, relatives, and chronic illness. The second included questions on the 23 items of the validated Arabic version of the pediatric sleep questionnaire-sleep-related breathing disorder (PSQ-SRBD) scale to assess symptom-complexes associated with snoring, breathing difficulties, mouth breathing, daytime sleepiness, behavioral/inattention, and other symptoms. Each question had three possible responses: yes = 1, no = 0, and do not know = missing. The number of symptom items that receive a positive response (“yes”) is divided by the total number of items that receive a positive or negative response. Thus, the denominator eliminates items with missing responses. The result is a number with a proportion ranging from 0.0 to 1.0. Scores > 0.33 are considered positive and suggestive of a high risk of pediatric sleep-related breathing disorder [10]. The third part of the questionnaire covered academic performance, with five possible responses: excellent, very good, good, pass, and fail.
Sample size calculation
We sought to ascertain the sample size required to accurately estimate the prevalence of high risk of OSDB among the target population. Based on two previous studies, we aimed to detect a prevalence rate of 10-18.5% within the population of interest [11,12]. To ensure statistical rigor, a confidence level of 95% was established a priori along with a 4% margin of error. By employing the normal approximation method to construct confidence intervals (CIs) around a sample proportion, we deduced that a sample size of approximately 362 participants was necessary.
Inclusion criteria
We included Saudi pediatric males and females aged six to 18 years. Data were collected between March and April 2023.
Ethical approval
Ethical approval was obtained from the Standing Committee for Scientific Research at Jazan University (reference number REC-44/02/297, dated September 15, 2022).
Statistical analysis
Statistical analyses were performed using R, version 4.3 (R Foundation for Statistical Computing, Vienna, Austria). Categorical variables are summarized as counts and percentages. The mean ± standard deviation (SD) and median/interquartile range (IQR) were used to summarize continuous normal and non-normal variables, respectively. The chi-square test of independence was used to assess the associations between categorical variables. Spearman’s correlation coefficient was used to assess whether the grades were significantly associated with sociodemographic characteristics and comorbidities. Ordinal logistic regression was used to assess the factors associated with the odds of higher grades. Hypothesis testing was performed at the 5% significance level.
Results
The study included data from 367 children (191 (52%) males and 176 (48%) females). One-quarter of the respondents were in upper elementary school (97, 26.4%) and more than one-third were in primary elementary school (145, 39.5%). More than two-thirds of the parents had at least a bachelor’s degree. The average monthly income was 10,000-20,000 SAR (Table 1).
Several comorbidities were reported in the children, including asthma (63, 17.2%) and cardiac problems (6, 1.63%). However, no chronic diseases, including hypertension or diabetes mellitus, were reported in 292 (79.6%) of the children. The total daily and night sleeping time was >9 hours in 205 (55.9%) and 105 (28.6%) of the included children, respectively. Two-thirds of the parents reported that their children slept after 10 PM. The prevalence of high risk of OSDB in the study sample was 31.58% (95% CI: 36.51-41.67). The median PSQ-SRBD questionnaire was 0.23 (IQR 0.09; 0.45) (Table 2).
More than three-quarters of the respondents achieved excellent grades in all the included subjects and in the overall grade (Figure 1).
Grades of the included respondentsThe proportion of children who achieved each grade as well as the average score, assuming excellent = 5 and poor = 1.
High risk of OSDB was negatively associated with the grades of all subjects and with the overall grade (p < 0.001) (Figure 2).
Correlation between the grades of the children and socio-demographic characteristics p < 0.05, ** p < 0.01, *** p < 0.001OSDB score: OSDB score as a continuous variable; OSDB: OSDB as yes/no, based on a cutoff of 0.33.OSDB, obstructive sleep-disordered breathing*
A comparison between children with and without high risk of OSDB is illustrated in Figure 3.
Association between high risk of obstructive sleep-disordered breathing (OSDB) and socio-demographic characteristicsThe numbers on the right represent the percentage of respondents who obtained excellent or very good grades. The numbers on the left represent the percentage of those who obtained acceptable or poor grades.
The high risk of OSDB score was negatively correlated with the grades of all participants and the overall grade (p < 0.001).
Results suggest that the distribution of grades was between respondents without OSDB.
The results showed that the average age was not significantly different between children with and without OSDB. Males were more prevalent among children with high risk of OSDB (85 (63.4%) vs. 106 (45.5%); p < 0.001). The distribution of school levels did not differ significantly between groups. Nasal symptoms were more severe in patients with high risk of OSDB. The prevalence of different comorbidities was significantly higher in children with high risk of OSDB (p < 0.001 for bronchial asthma) (Table 3).
Although sleeping hours were not significantly different between the groups, higher income levels were reported in parents of children without ODSB (p < 0.001).
Ordinal logistic regression was used to assess the association between high risk of ODSB and overall grade after adjusting for possible confounders. The dependent variable was the overall grade (1 to 5) and independent variables included school level, education level, risk of ODSB (high vs. low), monthly income, and gender. Education was included as an ordinal variable.
The ordinal logistic regression model identified several factors associated with grade outcomes. Parent’s education level showed a significant positive association with grade, with each one-level increase in education level being associated with 1.74 times higher odds of achieving a higher grade (95% CI: 1.08-2.82, p = 0.023). Compared to families earning less than 10,000 SAR, families with an income of 10,000-20,000 SAR had significantly higher odds of achieving a higher grade (OR = 2.28, 95% CI: 1.04-5.00, p = 0.038). However, income levels of 20,000-40,000 SAR (OR = 2.57, 95% CI: 0.75-8.82, p = 0.134) and above 40,000 SAR (OR = 1.65, 95% CI: 0.47-5.74, p = 0.432) were not significantly associated with grades.
The risk of OSDB had a significant inverse relationship with grade outcomes. High OSDB risk was associated with 77% lower odds of achieving a higher grade compared to low OSDB risk (OR = 0.23, 95% CI: 0.11-0.47, p < 0.001). Gender did not show a significant association with grade outcomes (OR = 0.98, 95% CI: 0.50-1.92, p = 0.945). Similarly, school level (upper elementary, intermediate, and secondary) showed no significant association with grade outcomes when compared to the primary elementary reference group.
The overall grades were used for the analysis. The results of all the pairwise comparisons are presented in Figure 4.
Comparison of paediatric sleep questionnaire-sleep-related breathing disorder (PSQ-SRBD) score between different grades
The line in each box represents the median value. The upper and lower margins represent the 75 and 25% percentile, respectively. Pairwise comparisons using the Mann-Whitney U test showed a statistically significant difference in the distribution of high risk of OSDB scores between good and excellent grades, as well as between very good and excellent grades, with lower high risk of OSDB scores in children with higher grades. The Kruskal-Wallis test showed a statistically significant difference in the distribution of high risk of OSDB scores between the groups. The distribution of the high risk of OSDB scores also differed significantly between children with acceptable and excellent grades.
Discussion
High risk of OSDB has garnered increasing attention due to its potential to adversely affect academic performance among school-aged children and adolescents. Therefore, we comprehensively explored the association between OSDB and academic performance, examining its various facets, from the prevalence of high risk of OSDB in this demographic to its consequences on educational attainment and risk factors contributing to its development. Our results underscore the critical role of educational institutions in recognizing and addressing the high risk of OSDB-related challenges to optimize the academic outcomes of affected students.
The findings of this study on the negative association between high risk of OSDB and academic performance are in line with extensive research on this topic. Beebe et al. found that children with untreated SDB demonstrated decline in cognitive and academic performance over time, confirming its detrimental impact on academics [13]. Furthermore, a comprehensive review by Trosman et al. reinforced this finding by revealing that children with high risk of OSDB had lower cognitive and academic test scores than those without [14]. O'Brien et al. investigated the academic performance of children with high risk of OSDB and reported that they scored lower levels in reading and math assessments [15]. Additionally, Archbold et al. conducted a longitudinal study that showed that children with severe OSDB experienced poorer academic performance over time, emphasizing the dose-response relationship between OSDB severity and academic outcomes [16].
This study also highlights the presence of comorbidities, such as bronchial asthma, in some children with OSDB, which aligns with the existing research. Kheirandish-Gozal et al. found a bidirectional association between OSDB and asthma in children [17]. Children with OSDB were more likely to have asthma and vice versa. In contrast, one study found no significant group differences in test scores when evaluating six separate executive function areas in a chosen sample of patients without comorbidities [18]. Therefore, they concluded that OSDB without comorbidities did not result in impaired executive function. However, Hilsendager et al. found that OSDB paired with obesity impairs executive function, and that obesity status is a strong predictor of performance on executive functioning tests [19].
This study emphasized the influence of parental education and income on academic outcomes, which is in line with the broader literature on socioeconomic factors and academic success. Duncan and Magnuson noted that children from higher socioeconomic backgrounds tended to perform better academically [20]. Sirin reviewed the impact of socioeconomic status on academic achievement and highlighted income and education as key factors shaping children's educational outcomes [21].
The current study found a higher prevalence of OSDB in males, consistent with the results of other studies. Li et al. reported a higher prevalence of OSDB in male children than in female children [22].
This study noted variations in sleep duration and bedtime patterns among children, which are a relevant aspect of this discussion. Owens et al. investigated the impact of irregular sleep schedules on academic achievement in adolescents and found that irregular sleep patterns were associated with poor academic performance, thus highlighting the importance of consistent sleep routines [23]. Moreover, Short et al. emphasized the significance of adequate sleep duration for academic success, noting that insufficient sleep can impair cognitive function and negatively affect educational outcomes [24].
Our results demonstrated significant differences in OSDB scores between different grade groups, with lower OSDB scores in children in higher grades. Mitchell et al. reported that greater OSDB severity was associated with lower academic performance, which is consistent with the results of the current study [25]. Biggs et al. assessed the impact of OSDB on neurocognitive function in children and found that children with more severe OSDB had poorer neurocognitive outcomes, including academic difficulties [26].
A longitudinal study by Rosen et al. examined the impact of OSDB on academic performance and found that children with untreated OSDB had lower academic achievements, and that academic improvement was associated with the resolution of OSDB [27]. Golan et al. examined SDB in school-aged children and found that children with OSDB had lower school achievement scores than those without [28]. Another study by Carotenuto et al. investigated the neuropsychological profiles of children with OSA and observed deficits in attention, memory, and executive function that could have contributed to academic difficulties [29]. Furthermore, Brockmann et al. examined the impact of OSA on school performance of children and found that children with severe OSA had lower grades and poorer school attendance than the controls [30].
A longitudinal study by Marcus et al. followed up children with OSDB after adenotonsillectomy and found improvements in academic performance and behavior [31]. Another study investigated academic achievement in children with OSDB and found that they had lower scores on standardized tests than children without OSA [32]. In addition, Friedman et al. assessed the academic performance of children with OSA and found that they had lower reading and math scores than controls [33]. Smith et al. examined the relationship between OSA and academic achievement and found that children with OSA had lower standardized test scores and poorer school attendance [34]. Molfese et al. investigated the effects of OSA on academic achievement and found that children with OSA had lower scores on tests of reading and math [35]. Jackman et al. examined the academic achievements of children with OSDB and found that they had lower scores on measures of reading, math, and overall academic achievement, although no cognitive-behavioural impairments were observed [36]. Giordani et al. assessed the neuropsychological functioning of children with OSA and found deficits in attention, memory, and executive functions that could contribute to academic problems [37].
Our study is limited by being an online questionnaire, so we did not use polysomnography or examine the patients clinically. Furthermore, the evaluation of academic performance is done based on grades rather than scores.
Conclusions
In summary, the findings of this study showed that high risk of OSDB has been consistently associated with lower academic performance, underscoring the importance of early diagnosis and intervention to mitigate these effects. Further prospective studies are encouraged to clarify the long-term impact of high risk of OSDB and its treatment modalities on the academic and occupational performance of these patients.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Standards and indications for cardiopulmonary sleep studies in children Am J Respir Crit Care Med Loughlin GM Brouillette RT Brooke LJ 8668781531996856414710.1164/ajrccm.153.2.8564147 · doi ↗ · pubmed ↗
- 2Diagnosis and management of childhood obstructive sleep apnea syndrome Pediatrics Marcus CL Brooks LJ Draper KA 055130201210.1542/peds.2012-167122926173 · doi ↗ · pubmed ↗
- 3Upper airway structure and body fat composition in obese children with obstructive sleep apnea syndrome Am J Respir Crit Care Med Arens R Sin S Nandalike K 78278718320112093510510.1164/rccm.201008-1249 OCPMC 3081285 · doi ↗ · pubmed ↗
- 4Obesity in children with different risk factors for obstructive sleep apnea: a community-based study Eur J Pediatr Su MS Zhang HL Cai XH 21122017520162631631810.1007/s 00431-015-2613-6 · doi ↗ · pubmed ↗
- 5Pathophysiology of childhood obstructive sleep apnea: current concepts Respir Physiol Marcus CL 14315411920001072285710.1016/s 0034-5687(99)00109-7 · doi ↗ · pubmed ↗
- 6Allergy and sleep-disordered breathing Curr Opin Otolaryngol Head Neck Surg Kimple AJ Ishman SL 2772812120132361942410.1097/MOO.0b 013e 32835 ff 132 · doi ↗ · pubmed ↗
- 7Pierre Robin Sequence: evaluation, management, indications for surgery, and pitfalls Otolaryngol Clin North Am Scott AR Tibesar RJ Sidman JD 6957104520122258804410.1016/j.otc.2012.03.007 · doi ↗ · pubmed ↗
- 8Sleep-disordered breathing in paediatric setting: existing and upcoming of the genetic disorders Ann Transl Med Zaffanello M Antoniazzi F Tenero L Nosetti L Piazza M Piacentini G 343620183030608210.21037/atm.2018.07.13PMC 6174189 · doi ↗ · pubmed ↗