Addressing barriers to sustainable academic-community partnerships through Community Health Grants
Stacey M. Gomes, Monica J. Mitchell, Teresa Smith, Eric Rademacher, Sharon Watkins, Lori E. Crosby, Farrah M. Jacquez

TL;DR
This paper describes how microgrant programs help academic-community partnerships overcome barriers to sustainable health research by fostering collaboration and trust.
Contribution
The paper introduces two innovative microgrant programs that enhance academic-community partnerships through pilot projects and trust-building.
Findings
The programs engaged 94 community organizations and impacted over 55,000 individuals.
A survey of awardees showed high satisfaction and identified trust-building and sustainability as key outcomes.
Abstract
To facilitate and sustain community-engaged research (CEnR) conducted by academic-community partnerships (ACPs), a Clinical Translational Science Award (CTSA)-funded Community Engagement Core (CEC) and Community Partner Council (CPC) co-created two innovative microgrant programs. The Community Health Grant (CHG) and the Partnership Development Grant (PDG) programs are designed to specifically fund ACPs conducting pilot programs aimed at improving health outcomes. Collectively, these programs have engaged 94 community partner organizations while impacting over 55,000 individuals and leveraging 10 million through other grants and awards. A cross-sectional survey of 57 CHG awardees demonstrated high overall satisfaction with the programs and indicated that participation addressed barriers to CEnR, such as building trust in research and improving partnership and…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
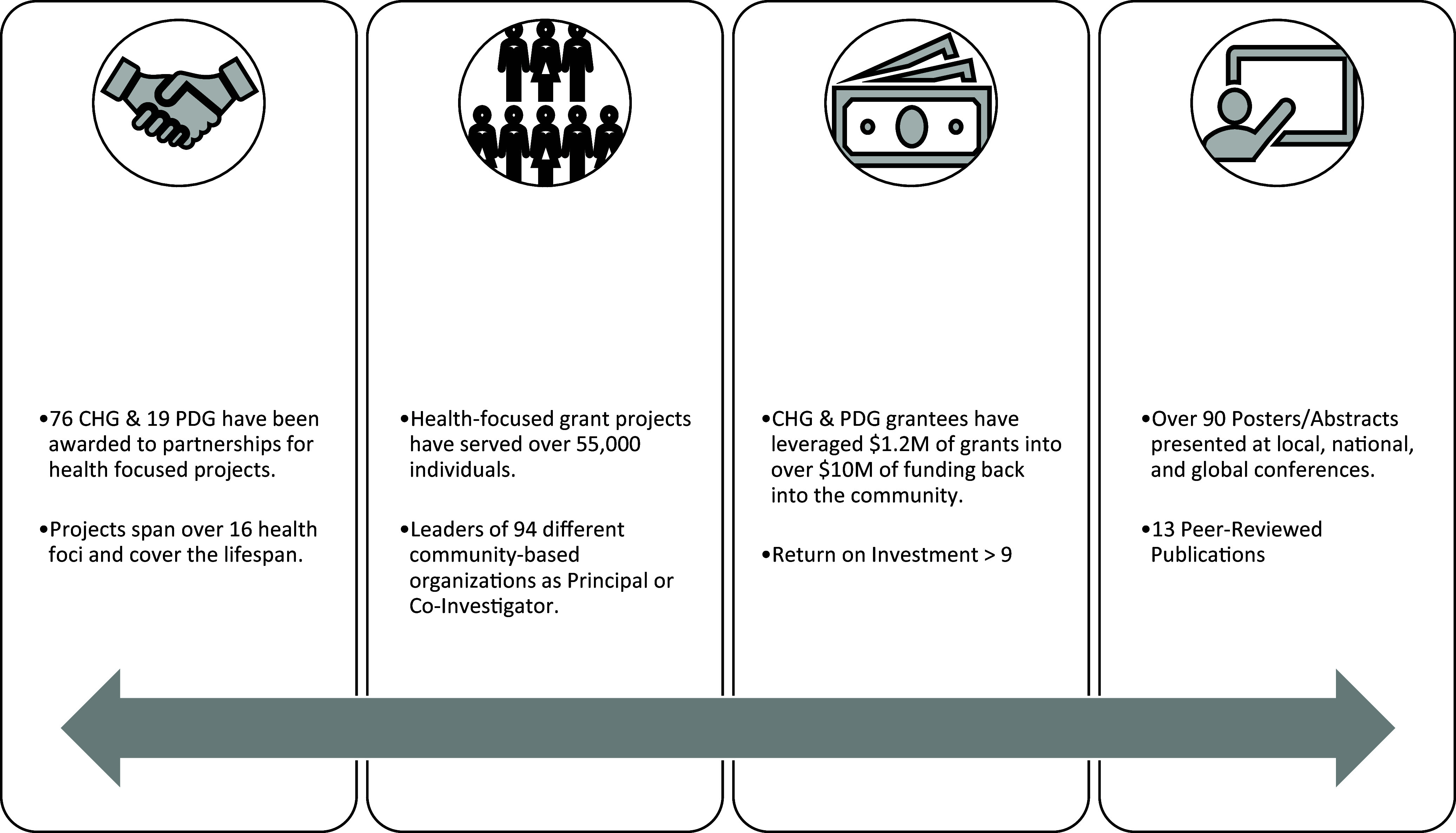 Figure 1
Figure 1 Figure 2
Figure 2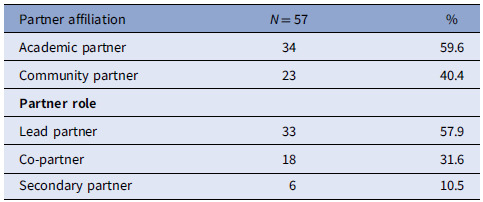 Figure 3
Figure 3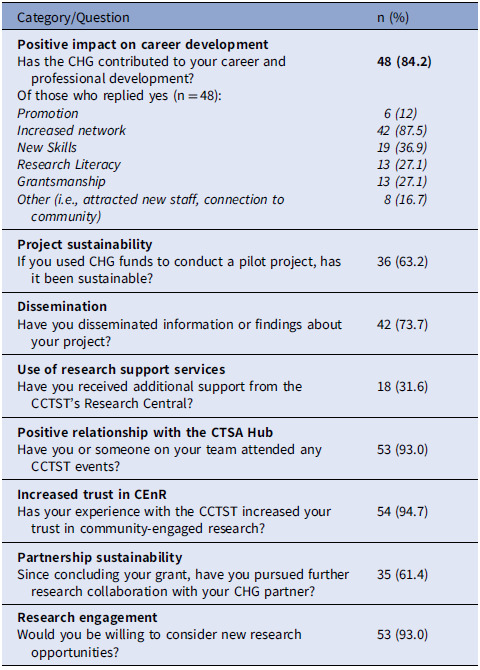 Figure 4
Figure 4Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsService-Learning and Community Engagement · Health Policy Implementation Science · Mental Health and Patient Involvement
Introduction
Community-engaged research (CEnR) addresses health disparities and improves community health outcomes, as partnering with the community promotes alignment with community priorities and needs [1–5]. CEnR has been identified as a best practice in public health; it also contributes significantly to the relevance and sustainability of health interventions [6]. Academic-community partnerships (ACPs) increase the feasibility and impact of CEnR as community members contribute to study design, implementation, and dissemination [5,6]. Translation of research findings is also improved when community voice is reflected in the interpretation of data and dissemination is tailored to meet the needs of varying facets of the community [5,7].
Although ACPs strengthen health-focused research, these partnerships are sometimes challenging due to several structural and logistical barriers that contribute to mistrust; thus, there is an increased need for resources to support partnerships and collaborations [8]. Facilitators of successful CEnR include competence within organizational domains of leadership, regulatory support and knowledge, and ethical conduct of research [9]. Potential barriers can include establishing a community advisory board, addressing conflicting priorities between academics and the community, collaborating with under resourced and marginalized communities, launching a community-based project, and facilitating and sustaining community engagement [8,10]. These barriers are perpetuated by fiscal and administrative policies that impede power sharing and communication among partnerships and require navigation of complex institutional policies and procedures [11]. Furthermore, traditional governmental funding mechanisms typically fail to account for the time and resources needed to establish trust, develop a partnership necessary for authentic community-engaged research, and conduct the research collaborative activities [12].
One method to promote and sustain ACPs to conduct health research is through funding mechanisms. For example, microgrants which stem from microfinancing, originally developed to provide small business loans to stimulate the economy of underserved communities, have been utilized to provide funding to ACPs – based on scientific merit and community relevance [14,15]. These microgrants not only increase community participation in health research but also can be focused on meeting individual communities’ needs [6,13]. While there is a growing portfolio of funding opportunities requiring community involvement, a systematic review of community grant programs indicated that most focus on a single health area (e.g., cancer and diabetes), and the majority do not focus solely on partnerships, such as ACPs, as an eligibility requirement [1,13,16]. Furthermore, literature describing these programs, including their development and outcomes, is sparse, and there is a lack of consistent measurement of community health outcomes [13]. Yet, there is evidence to support that participating in a partnership facilitated better project sustainability among Community Health Grant-supported projects. In addition, outcomes are enhanced when there is power-sharing, and the community partner takes an active role in the design and dissemination of the research [13]. Thus, an effective and sustainable way to facilitate impactful, long-term health research in the community may be to fund ACPs while also providing support to minimize barriers to conducting CEnR.
In 2010, the Community Partner Council (CPC) of the Center for Clinical and Translational Science (CCTST)’s Community Engagement Core (CEC) in partnership with the CEC, co-created a Community Health Grant (CHG) program to promote ACP health research in the Greater Cincinnati Region and the surrounding communities (Southwest Ohio including the City of Cincinnati, Northern Kentucky, and Southeast Indiana). Later, in 2018, the Partnership Development Grant (PDG) was created as a seed microgrant to support partnerships during the development phase. Collectively, these grant programs aim to facilitate and support ACPs in conducting health-focused research in the local community. This paper describes the microgrants programs, their impact and outcomes, and lessons learned through an iterative feedback process that we have used and developed for over a decade. It is hoped that it can serve as a guide for the development and implementation of similar ACP microgrants programs.
Methods
Programs
Community Health Grants (CHG)
The CHG request for proposals was developed in partnership with the CPC and focuses on facilitating research conducted by community and academic partners. Either can apply as the principal investigator, but applicants must be part of an ACP consisting of at least one academic partner (faculty or affiliates from CCTST member institutions) and one community partner (e.g., community programs, agencies, physician practices, and non-profit organizations). The CHG program funds ACP projects that (1) apply existing knowledge about health to real-world settings (i.e., translational research) and (2) demonstrate shared decision-making in research activities intended to improve outcomes for the community. Projects must also be feasible within a one-year funding period, use a community-engaged measurement and evaluation strategy, and include a sustainability plan for both the project and partnership. ACPs can receive up to $20,000 in funding for one year for their proposed project.
The complete CHG proposal application includes information on the (1) academic and community partners; (2) proposed health program or translational research project; (3) proposed partnership, impact, and innovation of the project; (4) research and/or evaluation plan; (5) community benefits and sustainability plan; and (6) project timeline and budget (see Appendix 1 for more details). The sustainability plan must describe how the ACP and proposed project will continue to make an impact beyond the funding period. Review criteria are described below.
Partnership Development Grants (PDG)
New and developing ACPs may apply to the PDG program to support a health-focused pilot study or needs assessment in a shared interest area. Like the CHG, eligible partnerships include at least one academic faculty or staff member and at least one member of a non-profit organization. The CCTST CPC reviews all proposals using a standardized scoring system and discusses them at a review meeting. For the PDG, the same scoring categories are used during the review as the CHG; however, the scope of the project is expected to be smaller, and much more emphasis is placed on the potential impact of the partnership collaborating on the health challenge. Funded grantees receive up to $5,000 to complete their project over one year. Free, unlimited support from the CCTST Staff is available throughout the program. All awardees are also invited to other CCTST CEC activities, including academic-community Speaker Series dinners, Grand Rounds, poster sessions, and community forums.
Review processes
Applicants for both programs are encouraged, but not required, to (1) attend an information session describing the program, application process, and experiences of past awardees and (2) submit a one-page Letter of Intent (LOI). The LOI includes information about the ACP and proposed project and is due two months before the proposal. CEC faculty provide thorough, written feedback to any partnerships submitting LOIs, intending to help applicants submit their most competitive proposal. Any LOIs that describe projects that may be a better fit for other CCTST grants or training opportunities receive information about those opportunities and a recommendation that they apply in a future grant cycle. Tailored technical assistance is also offered through the CEC staff to help strengthen proposal components and is available for grantees throughout the funding period. These services include, but are not limited to, research staff and community advisory board review of research design, community engagement and recruitment plans, data analysis plans, evaluation methods, assistance with interpretation, and dissemination strategies.
Each application undergoes a technical review and is independently scored by 2–3 reviewers (including at least one academic and one community reviewer) selected based on their areas of expertise and to avoid any conflict of interest. Proposals are scored using established criteria: a) the strength and capacity of the ACP, b) the proposed health challenges to be addressed, c) potential impact, d) innovation, e) evaluation plan, f) sustainability, and g) project feasibility. At the full review meeting, a primary reviewer presents an overview, strengths, and concerns regarding the application, followed by a full committee discussion of how the application fits with funding priorities and other considerations (e.g., multiple grant applications from a partner, whether the applicant is a past awardee, etc.). The joint and complementary expertise of academic and community partners is highly valued during the review which is demonstrative of program co-creation and shared decision-making. Integration of expertise is an integral determinant of the grant score and drives funding prioritization. The review meeting ends with the compilation of recommended applications, which are then submitted to CCTST leadership for funding approval.
Metrics
All grant awardees provide progress reports biannually assessing the number of individuals impacted, progress toward achieving goals, other relevant grant funding or training received, dissemination activities, community benefits, new health initiatives resulting from the project, and a summary of the budget and expenses to date. In 2018, progress reports were revised to include overall program satisfaction and other metrics beyond return on investment (ROI) to better align with the Clinical Translational Science Award (CTSA)’s initiative to create common metrics [17]. Additional operational outcomes (e.g., number of applications and attendance at program events) were collected from program records. Progress report data from the 2010–2021 CHG and 2017–2021 PDG grant cycles were included in the current analyses.
CHG survey
In November 2013, grant awardees from the first four cycles (2010–2013) of the CHG program were emailed and/or contacted by phone and asked to complete a follow-up survey in SurveyMonkey® that assessed their overall satisfaction with the CHG, its impact on their partnership and the community, the sustainability of the partnership and project, and the dissemination of results. In September 2018, grant awardees from four additional cycles (2014–2017) were contacted to complete the same survey. A total of 189 lead and secondary partners from 55 funded projects were invited to participate in the evaluation.
Data analysis
Grant outcomes, operational data, and survey responses were all analyzed using IBM SPSS Statistics for Windows, version 25 (IBM Corp., Armonk, N.Y., USA). Descriptive statistics were used to summarize partnership and survey data. ROI was calculated using the overall amount of additional funding grantees reported obtaining for related projects after receiving the CHG or PDG divided by the overall cumulative amount of program funds awarded to grantees (2010–2021).
Results
Program impact & outcomes
Over the first 12 CHG cycles, 76 academic-community partnerships received a total of 81,799 were awarded. Three of the 19 PDG projects went on to successfully apply for CHG funding.
Outcomes from the CHG and PDG are depicted in Fig. 1. During the one-year funding period, CHG awardees from grant cycles 2010–2021 reported leveraging 8.4 million in state and federal funding by applying to other grant mechanisms to sustain CHG projects (ROI>9.3), including the Ohio Department of Health, National Institutes of Health, U.S. Department of Health & Human Services, and NAACP. Subsequently, recipients of the PDG leveraged a grant investment of 729,500.00 (ROI>8.9). Combined, CHG and PDG have been awarded to partnerships representing 94 different community-based organizations and have impacted over 55,000 individuals. Grant results have been disseminated broadly, including presentations, abstracts, and peer-reviewed publications.
Figure 1. Outcomes of community health grants (CHGs) and partnership development grants (PDGs) describe the overall outcomes of the microgrant programs with respect to the number of partnerships, numbers served, funding obtained post-award, and dissemination.
Survey Results
The CHG survey was completed by 57 grantees, including 23 community partners (40.4% of respondents) who participated in 55 CHG-funded projects (see Table 1). Overall satisfaction with the CHG program was high: almost all (n = 54, 94.7%) agreed or strongly agreed with the statement “I was satisfied with the Community Health Grant program” (see Fig. 2). Additionally, partners reported a variety of dissemination activities, including presentations (n = 34), academic papers (n = 13), and community-focused newsletters (n = 11) related to ACP projects. Nearly half (n = 26; 45.6%) reported conducting staff education sessions or training related to their grant project.
Figure 2. Overall satisfaction with the Community Health Grant (CHG) program illustrates the overall satisfaction of participants responding to the Community Health Grant evaluation survey (n = 57) in 2013 and 2018 across different domains.
Table 1.Community Health Grant survey participants indicate the affiliation and role of each participant (n = 57) in the Community Health Grant evaluation in 2013 and 2018Partner affiliation N = 57%Academic partner3459.6Community partner2340.4 Partner role Lead partner3357.9Co-partner1831.6Secondary partner610.5
Participants also indicated they were satisfied with their CHG partner (91.2%), that the CHG had a positive long-term impact on their ACP (89.5%) and their organization (84.2%), and that they intend to pursue additional research opportunities in the future (89.5%). Most also agreed or strongly agreed that the CHG positively impacted the community (93.0%). Over half of respondents reported that their pilot projects funded by the CHG program were sustained beyond the funding period (n = 36; 63.2%) and have continued to engage in research collaboration with their CHG partner (n = 35; 61.4%). For those who did not sustain the project beyond the funding period, this was most often attributed to a lack of funding and/or personnel. Some grantees (n = 18, 31.6%) also utilized the research services offered by the CCTST either during or after the award period, such as assistance with REDCap databases, community engagement, grant writing, study design, or data management and statistical analysis. CHG awardees have remained engaged with the CCTST and CEC, joining CPC subcommittees (n = 12), participating in the Community Leaders Institute (an eight-week research training program; n = 24) [18], and attending CEC Speaker Series events, including Grand Rounds (n = 26) [19], Awards Ceremonies (n = 38), and Community Forums (n = 26).
Participants indicated that the CHG positively impacted their career development, research literacy, and perceptions of CEnR (see Table 2). Most respondents reported that the CHG program contributed to their career and professional development (n = 48; 84.2%), including broadening their network, learning new skills, improving research literacy, increasing grantsmanship, and event promotion. Other positive career outcomes included attracting new staff members to organizations and fostering a greater connection with the community. Finally, grantees indicated that participating in the CHG program increased their trust in CEnR.
Table 2.Community Health Grant (CHG) survey responses demonstrate the outcomes related to community-engaged research categories from the Community Health Grant evaluation survey (n = 57) in 2013 and 2018Category/Questionn (%) Positive impact on career development Has the CHG contributed to your career and professional development?Of those who replied yes (n = 48): Promotion
Increased network
New Skills
Research Literacy
Grantsmanship
Other (i.e., attracted new staff, connection to community)
48 (84.2)
6 (12)
42 (87.5)
19 (36.9)
13 (27.1)
13 (27.1)
8 (16.7)
Project sustainability If you used CHG funds to conduct a pilot project, has it been sustainable?36 (63.2) Dissemination Have you disseminated information or findings about your project?42 (73.7) Use of research support services Have you received additional support from the CCTST’s Research Central?18 (31.6) Positive relationship with the CTSA Hub Have you or someone on your team attended any CCTST events?53 (93.0) Increased trust in CEnR Has your experience with the CCTST increased your trust in community-engaged research?54 (94.7) Partnership sustainability Since concluding your grant, have you pursued further research collaboration with your CHG partner?35 (61.4) Research engagement Would you be willing to consider new research opportunities?53 (93.0)
Discussion
This paper describes the development and evaluation of the CHG and PDG programs, innovative partnership development initiatives sponsored by Cincinnati’s CTSA hub (CCTST). These microgrant programs support CEnR projects that are feasible, impactful, and address barriers to CEnR. CHG and PDG-funded projects address health priorities identified by community-level data and have served tens of thousands of community members. Grants have successfully leveraged additional funding, bringing over $8 million in additional grants into the Greater Cincinnati community for health programing and research. The ability to secure funding post-CHG/PDG is an indicator that the microgrant programs likely contributed to ACP sustainability.
CHG survey results suggest that the grantees are satisfied with the program and that the grants benefited ACP participants and communities/populations served. Those who utilized CCTST services were also satisfied, and engagement with the CCTST was reported to be high. Moreover, most respondents reported that their project findings have been disseminated in some way (e.g., presentations, newsletters, publications). Evaluation results also revealed unintended benefits related to career and professional development (e.g., promotion, learning new skills, promotion, broadening network to new sectors). Technical assistance and support provided by the CCTST may have supported participants and minimized traditional barriers to ACP engagement and collaboration. Finally, respondents reported that the grant programs increased their trust in collaborative CEnR and intention to pursue additional academic-community research opportunities.
The community and public health, economic, and policy benefits associated with the CHG program are comparable to other funding mechanisms [20,21]. However, while similar microgrants exist, to our knowledge, the CHG is a novel approach to funding community microgrants because it was created, implemented, and evaluated in collaboration with community partners. Furthermore, the CHG and PDG programs, directly addressed barriers to CEnR and ACP-conducted research by increasing trust between partners, providing research and team-building resources, and providing seed funds that lead to the implementation of more sustainable programs.
Our finding that ACP-funded research was sustained as evidenced by subsequent funding and partner self-report is commensurate with a systematic review of 36 grant-funded community health revealed that partnerships were associated with long-term project sustainability, which further supports funding ACP-conducted research. This review also found that only a small percentage of the initiatives were evidence-based and/or reported health outcomes [22–25]. Our program not only requires an in-depth evaluation plan in the proposal but also provides technical support to help applicants utilize validated measures where appropriate and select outcomes based on evidence. Thompson et al. indicated that restrictive project timelines and application requirements were barriers to success in projects funded through their cancer prevention program [26]. While the CCTST offers resources such as technical assistance, sustainability, logistical, and dissemination challenges remained. Thus, these are key areas to be addressed in future iterations of the programs.
Lessons learned
Utilizing a microgrant funding mechanism to promote similar programs in other institutions, across the CTSA network, and among community groups, could potentially increase the number and success of ACPs. The CHG and PDG led to several lessons learned, including (1) the development and utilization of a review process involving both academic and community partners, which is critical to the successful implementation of funded projects; (2) identifying priority neighborhoods, populations, or outcome areas to catalyze community action in underserved locations, helping to strengthen cumulative impact; and (3) prioritizing projects that reflect the outlined goals of the awarding institution, community partners, and the ACP facilitates sustainability. Notably, institutional commitment to allocate funding for these microgrants annually was paramount to our success. Other institutions may consider utilizing the results and impact of these microgrant programs and others to justify the budget for similar programs.
Limitations
Several limitations exist within this work, including a relatively low response rate (30.2%) for the survey. Because many funded projects included multiple academic and community partners, many secondary partners did not participate. However, based on the data, we believe we have a representative sample of the primary coordinating partners from both community and academic institutions. Another limitation is that all progress reports are completed by awardees 12–18 months after funding, so there may be recall biases. We also did not collect data 2–5 years post-award so may have missed reporting longer-term outcomes. Additionally, in our region, community members have a larger turnover rate than academic partners and were therefore more difficult to contact. Finally, all fields in the progress reports were not always completed. Future progress reports should consider collecting longer-term data to assess sustainability, health impact, and translational benefits including community and economic impact. Another limitation is that all projects were conducted in the greater Cincinnati region; thus, findings should be confirmed in other communities.
Next Steps and Implications
The CHG Program promotes CEnR conducted by ACP. Our data suggested that we have developed reliable processes and methods for using a community-driven health microgrant as a funding strategy to accomplish the CCTST and CTSA program’s aim of engaging communities in clinical and translational research. In addition to providing funding for essential partnership building, these programs may also help address known barriers to successful CEnR, including building trust and sustaining ACPs. These funding programs can be adapted and adopted by other CTSAs and academic institutions seeking to support CEnR. Overall, by leveraging the benefits of programs like the CHG and PDG while also addressing areas for improvement (e.g., additional resources, more support for sustainability between funding cycles), CTSAs can enhance their infrastructure to support ACPs and CEnR, both institutionally and across the translational research spectrum.
Supporting information
Gomes et al. supplementary material 1Gomes et al. supplementary material
Gomes et al. supplementary material 2Gomes et al. supplementary material
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Ramos MA , Fox A , Simon EP , Horowitz CR. A community-academic partnership to address racial/ethnic health disparities through grant-making. Public Health Rep. 2013;128 Suppl 3(Suppl 3):61–67. doi: 10.1177/00333549131286 S 310.24179281 PMC 3945451 · doi ↗ · pubmed ↗
- 2Israel BA , Schulz AJ , Parker EA , Becker AB. Review of community-based research: assessing partnership approaches to improve public health. Annu Rev Public Health. 1998;19(1):173–202. doi: 10.1146/annurev.publhealth.19.1.173.9611617 · doi ↗ · pubmed ↗
- 3Holzer JK , Ellis L , Merritt MW. Why we need community engagement in medical research. J Investig Med. 2014;62(6):851–855. doi: 10.1097/JIM.0000000000000097.PMC 410854724979468 · doi ↗ · pubmed ↗
- 4Ahmed SM , Palermo AG. Community engagement in research: frameworks for education and peer review. Am J Public Health. 2010;100(8):1380–1387. doi: 10.2105/AJPH.2009.178137.20558798 PMC 2901283 · doi ↗ · pubmed ↗
- 5Institute of Medicine (US) Committee on Educating Public Health Professionals for the 21st Century, Hernandez L. Who Will Keep the Public Healthy?: Workshop Summary, Washington (DC): National Academies Press (US); 2003.
- 6Jenkins C , Fagan HB , Passarella J , Fournakis N , Burshell D. Training academic and community investigator teams for community-engaged research: program development, implementation, evaluation and replication. Prog Community Health Partnersh. 2020;14(2):229–242. doi: 10.1353/cpr.2020.0019.33416644 PMC 8392131 · doi ↗ · pubmed ↗
- 7Mc Mc Closkey DJ , A.-G. S , Michener JL. Principles of community engagement, 2nd ed. ed. 2011. Washington, DC.
- 8Hallmark CC , Bohn K , Hallberg L , Croisant SA. Addressing institutional and community barriers to the development and implementation of community-engaged research through competency-based academic and community training. Front Public Health. 2023;10:1070475. doi: 10.3389/fpubh.2022.1070475.36711424 PMC 9877443 · doi ↗ · pubmed ↗