Antimicrobial resistance of Streptococcus pneumoniae from invasive pneumococcal disease in Brazil
Pedro Kurtz, Pedro Fernandez Del Peloso, Fernando Augusto Bozza

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
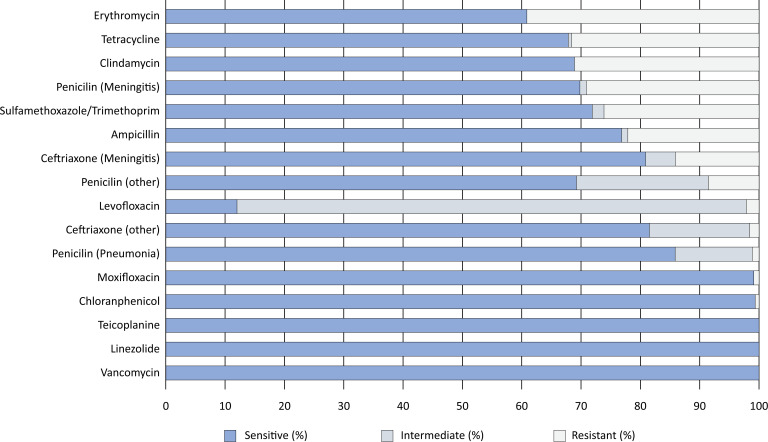 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPneumonia and Respiratory Infections · Bacterial Infections and Vaccines · Pneumocystis jirovecii pneumonia detection and treatment
Invasive pneumococcal infections, which are predominantly caused by Streptococcus pneumoniae (S. pneumoniae), remain a significant health concern throughout the world. S. pneumoniae is the principal pathogen in community-acquired pneumonia and bacterial meningitis, which often lead to severe complications; moreover, these diseases require intensive care and are associated with increased mortality rates. A particularly concerning trend involves the emergence of penicillin- and cephalosporin-nonsusceptible pneumococcal strains, which pose a growing challenge to public health worldwide.^(1–4)^
Our study aimed to assess the prevalence of antimicrobial-resistant pneumococci in the hospital setting in Rio de Janeiro, Brazil. Between January 1^st^, 2021, and December 31^st^, 2023, we analyzed all 411 consecutive isolates of S. pneumoniae from blood cultures of individual patients from 16 tertiary hospitals. These bacterial isolates were identified utilizing MALDI-TOF mass spectrometry, and antibiotic susceptibility testing was conducted with the VITEK 2 XL system using the AST-ST03 card. We conducted parallel resistance screening for beta-lactams using oxacillin discs and determined the minimum inhibitory concentrations (MICs) for penicillin and ceftriaxone, whereby we employed concentration gradient strips for subsequent comparative analysis. The interpretation of the results adhered to the standards of EUCAST version 14.0.^(5)^
The median age of the patients was 46 years (interquartile range 4 - 71), and 48% were female, with 141 (34%) children and 136 (33%) elderly patients being analyzed (Table 1). When MIC breakpoints for meningitis treatment were considered, we detected in vitro antimicrobial nonsusceptibility (resistance) in 14% of the isolates for ceftriaxone and 29% for penicillin. When the MIC breakpoints for other infections were considered, resistance was present in 2% of the isolates for ceftriaxone, 8% for penicillin, 22% for ampicillin, 26% for sulfatrimethoprim, 1% for moxifloxacin, and 2% for levofloxacin. Remarkably, no resistance was observed for linezolid, teicoplanin, or vancomycin (Figure 1).
Our findings revealed that approximately one in every seven S. pneumoniae isolates were nonsusceptible to ceftriaxone as a treatment for meningitis, which remains the first-line therapy recommended by the Brazilian Ministry of Health.^(6)^ Data on ceftriaxone resistance in meningitis vary widely in the literature, with resistances ranging from as low as 1% to as high as 20%.^(1–4)^ Additionally, 17% of isolates had intermediate MICs for ceftriaxone for other infections, such as pneumonia, which would require higher antimicrobial doses or alternate treatments compared to current therapeutic recommendations.^(7,8)^ These results urge a reconsideration of empirical antibiotic strategies for meningitis and possibly for pneumonia. Empirical treatments for community-acquired meningitis should always involve the combination of ceftriaxone and vancomycin, as recommended by international guidelines.^(9–11)^ Our study has evident limitations. First, our data had no information on the serotype distribution among the samples, which has been shown to affect the severity of disease, resistance patterns, and vaccine effectiveness. Nonetheless, serotypes are not usually clinically evaluated or utilized for individual decisions on empirical antibiotic treatment. Second, our database did not include clinical data on the etiology of invasive pneumococcal disease, the utilized antibiotics, or patient outcomes. This clearly limits our conclusions to the microbiological patterns of resistance. Future studies are needed to better understand the impact of these resistance patterns on the antibiotic response and clinical outcomes.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Brandileone MC Almeida SC Bokermann S Minamisava R Berezin EN Harrison LH Dynamics of antimicrobial resistance of Streptococcus pneumoniae following PCV 10 introduction in Brazil: Nationwide surveillance from 2007 to 2019 Vaccine 20213923320732153370706210.1016/j.vaccine.2021.02.063 · doi ↗ · pubmed ↗
- 2Rossoni AM Dalla Costa LM Berto DB Farah SS Gelain M Brandileone MC Acute bacterial meningitis caused by Streptococcus pneumoniae resistant to the antimicrobian agents and their serotypes Arq Neuropsiquiatr 2008663 A 5095151881371010.1590/s 0004-282x 2008000400014 · doi ↗ · pubmed ↗
- 3Sandoval MM Ruvinsky S Palermo MC Alconada T Brizuela ME Wierzbicki ER Antimicrobial resistance of Streptococcus pneumoniae from invasive pneumococcal diseases in Latin American countries: a systematic review and meta-analysis Front Public Health 202412133727613372763831780010.3389/fpubh.2024.1337276 PMC 10839967 · doi ↗ · pubmed ↗
- 4Parellada CI Abreu AJ Birck MG Dias CZ Moreira TD Julian GS Trends in pneumococcal and bacterial meningitis in Brazil from 2007 to 2019 Vaccines (Basel)2023118127912793763184710.3390/vaccines 11081279 PMC 10459388 · doi ↗ · pubmed ↗
- 5"The European Committee on Antimicrobial Susceptibility Testing Breakpoint tables for interpretation of MI Cs and zone diameters. Version 14.02024 Available from: http://www.eucast.org
- 6Ministério da Saúde, Secretaria de Vigilância em Saúde e Ambiente, Departamento de Ações Estratégicas de Epidemiologia e Vigilância em Saúde e Ambiente Guia de Vigilância em Saúde. 6a edição revisada Brasília Ministério da Saúde 2024 Disponível em: https://www.gov.br/saude/pt-br/assuntos/saude-de-a-a-z/t/tetano-acidental/publicacoes/guia-de-vigilancia-em-saude-6a-edicao.pdf/view
- 7Corrêa RA Costa AN Lundgren F Michelin L Figueiredo MR Holanda M 2018 recommendations for the management of community acquired pneumonia J Bras Pneumol 20184454054233051734110.1590/S 1806-37562018000000130 PMC 6467584 · doi ↗ · pubmed ↗
- 8Salluh JI Kawano-Dourado L Implementing the severe community-acquired pneumonia guidelines in low- and middle-income countries Intensive Care Med 20234911139213963772873910.1007/s 00134-023-07220-7 · doi ↗ · pubmed ↗