A case report of Barrett's esophageal adenocarcinoma in a young adult aged 20 years
Takayuki Ohi, Fumisato Sasaki, Nobuhisa Maeda, Shohei Uehara, Hidehito Maeda, Akihito Tanaka, Shuji Kanmura, Akihiro Yamasuji, Akio Ido

TL;DR
A 20-year-old Japanese woman was diagnosed with Barrett's esophageal adenocarcinoma, a rare condition in young adults, and successfully treated with endoscopic submucosal dissection.
Contribution
This case report highlights the rare occurrence of Barrett's esophageal adenocarcinoma in a young adult and emphasizes the importance of surveillance in high-risk individuals.
Findings
Barrett's esophageal adenocarcinoma was diagnosed in a 20-year-old Japanese woman.
The tumor was classified as pT1a-DMM and successfully treated with curative resection.
The case underscores the need for surveillance in young adults with risk factors like obesity and acid exposure.
Abstract
In Japan, the prevalence of Barrett's esophageal adenocarcinoma (BEA) has recently increased owing to a decrease in the number of patients with Helicobacter pylori infection, westernization of the diet, and an increase in obesity prevalence. However, BEA in patients in their 20s is extremely rare. Our patient was a 20‐year‐old Japanese woman with chief complaints of vomiting and nausea. Esophagogastroduodenoscopy was performed to investigate the cause of vomiting, and a raised lesion was found in the gastroesophageal junctional zone. In the magnified observation, the mucosal pattern of the lesion was partially invisible, and the vascular pattern was irregular; the lesion was diagnosed based on the Japan Esophageal Society classification for Barrett's esophagus ‐related superficial neoplasia. Endocytoscopic observations revealed a highly irregular glandular structure. Computed tomography…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
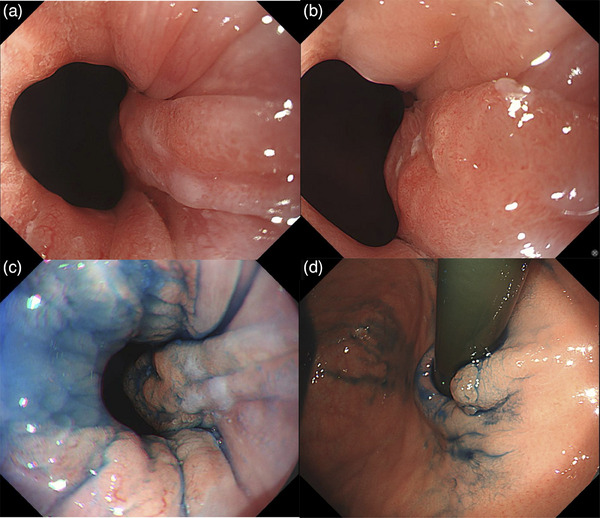 FIGURE 1
FIGURE 1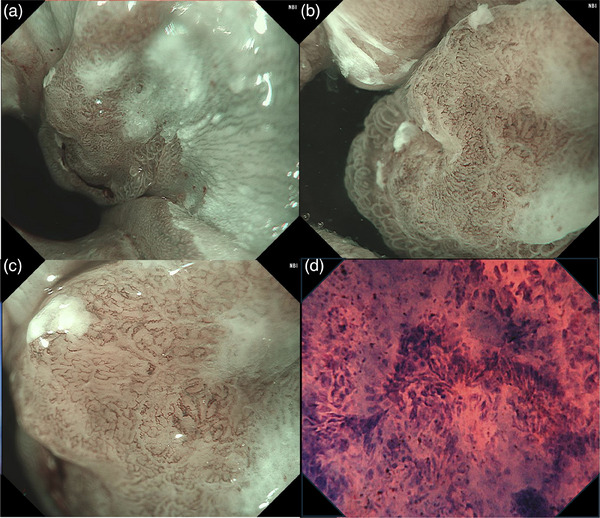 FIGURE 2
FIGURE 2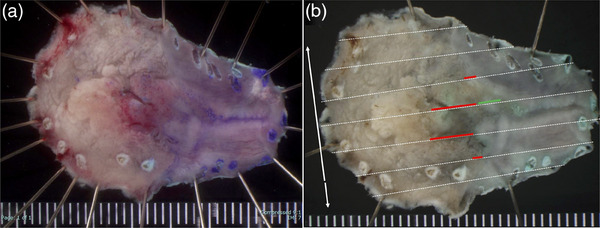 FIGURE 3
FIGURE 3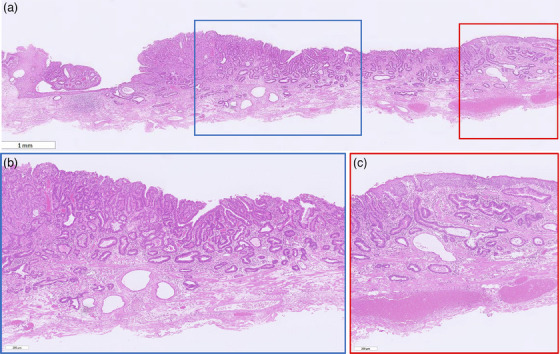 FIGURE 4
FIGURE 4- —None
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsEsophageal Cancer Research and Treatment · Gastric Cancer Management and Outcomes · Helicobacter pylori-related gastroenterology studies
INTRODUCTION
In Western countries, the proportion of adenocarcinomas in esophageal cancers is ≥60% and on the rise1 In Japan, the number of cases of Barrett's esophageal adenocarcinoma (BEA) has also increased recently due to a decrease in the number of patients with Helicobacter pylori infection, westernization of the diet, and an increase in obesity prevalence.2 BEA is more common in older men from an epidemiological perspective,2, 3 and BEA in young adults in their 20s has been rarely reported, in Japan and the West.
Case
The patient was a 20‐year‐old Japanese woman with chief complaints of vomiting and nausea. She had a history of schizophrenia and was prescribed multiple antipsychotics. There was no family history of gastric or esophageal cancer. At a previous clinic, she underwent esophagogastroduodenoscopy to evaluate frequent vomiting, which revealed a flat, elevated lesion at the esophagogastric junction. She subsequently visited our department. The patient was obese, with a height of 158.2 cm, a weight of 83.8 kg, and a body mass index of 33.5 kg/m^2^.
Esophagogastroduodenscopy was performed at our hospital. White light imaging revealed a flat, elevated lesion approximately 10 mm in size with an erythematous tone at the 2 o'clock position. The lesion was associated with short segment Barrett's esophagus, with a circumferential extent of metaplasia measuring 1.5 cm and a maximal extent of metaplasia measuring 2.0 cm (C1/M2). Additionally, reflux esophagitis (Los Angeles classification grade A) and a hiatal hernia were observed (Figure 1a,b). Observation using indigo carmine showed a depression in the center of the flattened elevation (Figure 1c,d). In the magnified observation with narrowband imaging, the lesion could be recognized as a brownish area (Figure 2a). We diagnosed the lesion using the Japan Esophageal Society classification for Barrett's esophagus (BE) related to superficial neoplasia.3 The mucosal pattern of the lesion was partially invisible, whereas the vascular pattern was visible and irregular (Figure 2b,c). Endocytoscopic observation showed disturbed polarity in the cellular arrangement within the lesion depression and a highly irregular glandular structure (Figure 2d). The lesion was easily deformed with changes in the amount of air, and endoscopic ultrasonography did not reveal submucosal invasion. No distant metastases were observed on contrast‐enhanced computed tomography. Based on these results, we diagnosed BEA (Jz, 10 mm, cType 0‐IIa+IIc, tub1, cT1a[M], cN0, cM0, and cStage IA) with a short segment BE background and performed endoscopic submucosal dissection. The resected specimen measured 32 × 19 mm, and the tumor measured 12 × 9 mm, with a depression in the center of the flat elevation. A well‐differentiated adenocarcinoma was located in the depressed area. The oral side of the lesion showed a subcutaneous extension in the indicated area (Figure 3).
Endoscopic white light imaging pictures. (a) The flat elevated lesion is observed with a short segment of Barrett's esophagus. (b, c) The lesion is located at the 2 o'clock position, and a slight depression is observed in the center of the lesion. (d) The anal border of the lesion is clearly observed from the retroflex position.
Endoscopic pictures of narrow‐band imaging and endocytoscopic imaging. (a) The lesion is observed as a brownish area. (b, c) The mucosal pattern of the lesion is partially invisible, and the vascular pattern is visible and irregular. (d) Endocytoscopic observation showed disturbed polarity of the cellular arrangement and a highly irregular glandular structure.
Resected specimen and mapping. (a) The tumor measures 12 × 9 mm. (b) The red line shows a well‐differentiated adenocarcinoma in the depressed area. The oral side of the lesion shows subcutaneous extension in the area indicated by the green line.
Histopathologically, the atypical glandular epithelium proliferated, forming irregular tubular glandular structures of various sizes. The background was considered BE, as the mucosal muscularis was multilayered and contained stratified squamous epithelium and esophageal glandular ducts (Figure 4a,b). The carcinoma extended to the multilayered muscularis mucosae and partially showed subepithelial extension (Figure 4c). Victoria Blue staining and CD31 and D2‐40 immunostaining showed no lymphovascular invasion.
Histopathological image. (a) The background mucosa exhibits features of Barrett's esophagus, as the mucosal muscularis is multilayered and contains stratified squamous epithelium and esophageal glandular ducts. (b) The atypical glandular epithelium is proliferating, forming irregular tubular glandular structures of various sizes. (c) The carcinoma extends to the multilayered muscularis mucosae and partially shows subepithelial extension.
DISCUSSION
The incidence of BEA has increased rapidly in Western countries.1 Although squamous cell carcinoma still accounts for most cases in Japan, the proportion of adenocarcinoma cases has increased from 1.7% in 1995 to 7.4% in 2015.4 The total number of cases of adenocarcinomas of the gastroesophageal junction, including BEA, is also increasing, with an increasing trend in all age groups, including young people.2 However, the percentage of patients with BEA aged <50 years is approximately 9%, and the rate in those aged <30 years is even lower.5 Only one report of BEA in Japanese patients aged <30 years exists in PubMed and the Japanese Medical Abstracts.6 This report describes an extremely rare case involving a 20‐year‐old patient with BEA. BEA originates from BE, which is divided into long segment BE of ≥3 cm and short segment BE of <3 cm and the risk of cancer differs depending on the length of the BE.7 The risk of cancer increases by 1.11 to 1.39 times for every 1 cm increase in the length of the BE, and the longer the BE,8 the higher the risk, with the annual rate of carcinogenesis of long segment BE being 1.2%.9 According to the 2022 edition of the Japan Esophageal Society Guidelines, esophagogastroduodenoscopy surveillance states that no recommendations can be currently made for BE with a maximum length of <3 cm.8 Furthermore, most guidelines recommend endoscopy for screening purposes only in patients aged ≥50 years with multiple risk factors.2 For this reason, BEA develops in young patients at a more advanced stage, and they have a poorer prognosis than older patients.10 Therefore, it is essential to identify risk factors and consider early screening tests, particularly for patients with symptoms such as vomiting and reflux esophagitis.
To date, the reported clinical risk factors for BEA are congenital factors such as race and sex; acquired factors such as smoking, obesity, and diet; and other gastrointestinal‐related factors such as gastric acid, bile acid reflux, failure of the reflux prevention mechanism, nitrate in saliva, length of the BE, H. pylori infection, and hiatal hernia.3 In addition, factors that contribute to the onset of the disease, particularly in young people, are obesity (body mass index ≥30 kg/m^2^) and gastric acid and bile acid reflux.2 This patient was considered to have a high risk of developing BEA owing to multiple risk factors, including obesity, exposure to acid and bile due to persistent vomiting, and hiatal hernia. There was no family history in this case, suggesting a low likelihood of genetic factors. Although previously reported cases were not obese, they exhibited symptoms of gastric acid and bile acid reflux.6
As the number of cases of BEA in Japan increases, there is a possibility of increasing the number of cases among young people. Therefore, as in the present case, it is necessary to conduct appropriate surveillance of patients with multiple risk factors.
CONFLICT OF INTEREST STATEMENT
None.
ETHICS STATEMENT
All procedures were performed in accordance with the ethical standards of the Declaration of Helsinki and its later amendments.
PATIENT CONSENT STATEMENT
Informed consent was obtained from the patient for the publication of this case report.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Arnold M , Laversanne M , Brown LM , Devesa SS , Bray F . Predicting the future burden of esophageal cancer by histological subtype: International trends in incidence up to 2030. Am J Gastroenterol 2017; 112: 1247–1255.28585555 10.1038/ajg.2017.155 · doi ↗ · pubmed ↗
- 2Iwaya Y , Shimamura Y , Goda K et al. Clinical characteristics of young patients with early Barrett's neoplasia. World J Gastroenterol 2019; 25: 3069–3078.31293342 10.3748/wjg.v 25.i 24.3069 PMC 6603815 · doi ↗ · pubmed ↗
- 3Goda K , Takeuchi M , Ishihara R et al. Diagnostic utility of a novel magnifying endoscopic classification system for superficial Barrett's esophagus‐related neoplasms: A nationwide multicenter study. Esophagus 2021; 18: 713–723.34052965 10.1007/s 10388-021-00841-1PMC 8387266 · doi ↗ · pubmed ↗
- 4Watanabe M , Toh Y , Ishihara R et al. Comprehensive registry of esophageal cancer in Japan, 2015. Esophagus 2023; 20: 1–28.36152081 10.1007/s 10388-022-00950-5PMC 9813101 · doi ↗ · pubmed ↗
- 5Drahos J , Xiao Q , Risch HA et al. Age‐specific risk factor profiles of adenocarcinomas of the esophagus: A pooled analysis from the international Beacon consortium. Int J Cancer 2016; 138: 55–64.26175109 10.1002/ijc.29688 PMC 4607633 · doi ↗ · pubmed ↗
- 6Kiyokawa H , Maehata T , Sato N et al. A case of Barrett's esophageal adenocarcinoma in young adult. Prog Dig Endosc 2013; 82: 87–89.
- 7Kitagawa Y , Ishihara R , Ishikawa H et al. Esophageal cancer practice guidelines 2022 edited by the Japan Esophageal Society: Part 1. Esophagus 2023; 20: 343–372.36933136 10.1007/s 10388-023-00993-2PMC 10024303 · doi ↗ · pubmed ↗
- 8Amano Y , Ishimura N , Ishihara S . Is malignant potential of Barrett's esophagus predictable by endoscopy findings? Life 2020; 10: 244.33081277 10.3390/life 10100244 PMC 7602941 · doi ↗ · pubmed ↗