Assessment of Ventricular-Arterial Coupling in Early Stage Middle-Aged Hypertensives
Andrea Vitali, Giuseppe Biondi Zoccai, George Booz, Raffaele Altara

TL;DR
This study shows that lifestyle changes and drug treatment can improve heart-artery coordination in early-stage middle-aged hypertension patients.
Contribution
The study demonstrates that VAC can be improved through lifestyle and drug interventions in early-stage hypertensives.
Findings
Lifestyle changes reduced blood pressure and improved ventricular-arterial coupling in early-stage hypertensives.
Anti-hypertensive drugs further improved VAC and related parameters after 6 months.
VAC was linearly related to arterial stiffness and heart strain measures.
Abstract
Ventricular-arterial coupling (VAC) is altered by aging and cardiovascular comorbidities, indicating myocardial dysfunction and/or arterial stiffness. Our aim was to demonstrate whether lifestyle changes and anti-hypertensive drug treatment would improve VAC in recently diagnosed, early stage middle-aged hypertensives (HTN) without organ damage. Arterial elastance (Ea), carotid-femoral pulse wave velocity (cfPWV), global longitudinal strain (GLS), and myocardial work (MW) [global work index (GWI), global constructive work (GCW), global wasted work (GWW), and global work efficiency (GWE)] were investigated. This retrospective observational study involved 126 individuals (mean age 40 years; 55% female), divided into HTN and normotensives, NT. Clinical, echocardiographic and echo vascular parameters were assessed. Lifestyle changes were recommended for HTN. If blood pressure (BP) values…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
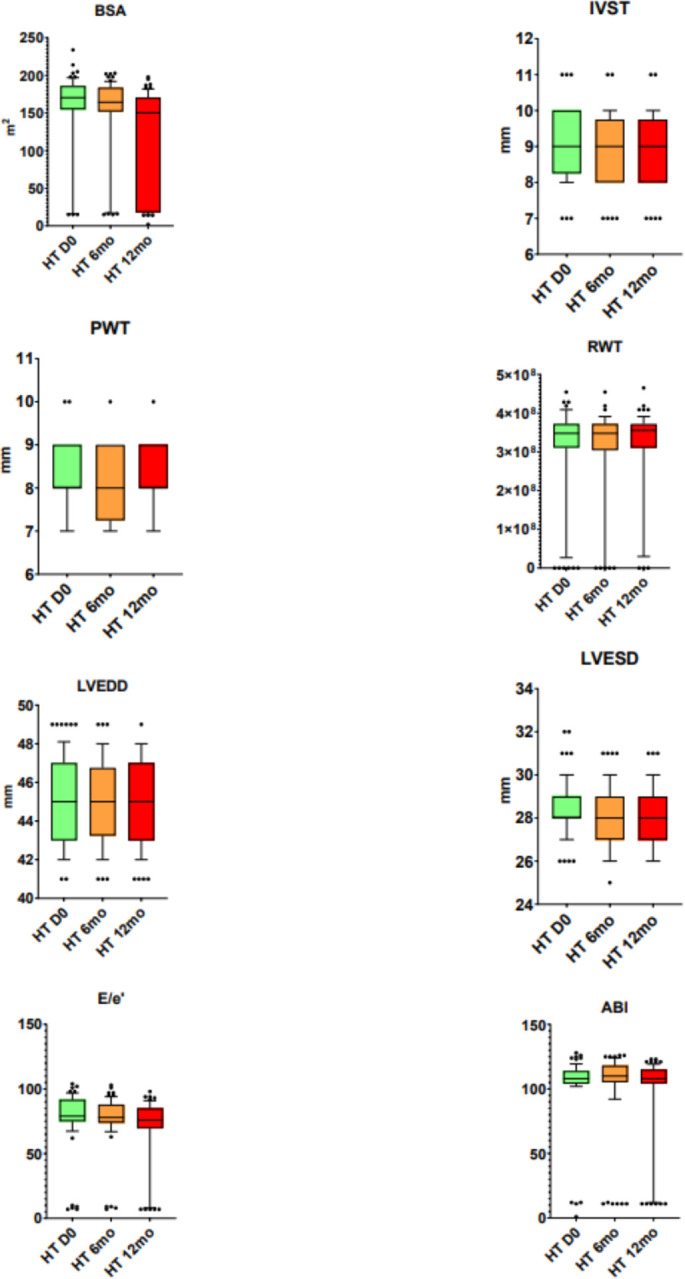 Figure 1
Figure 1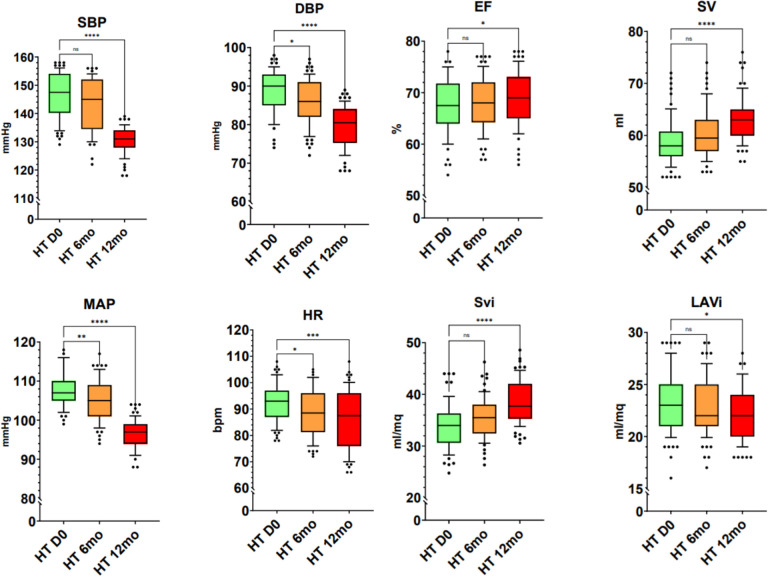 Figure 2
Figure 2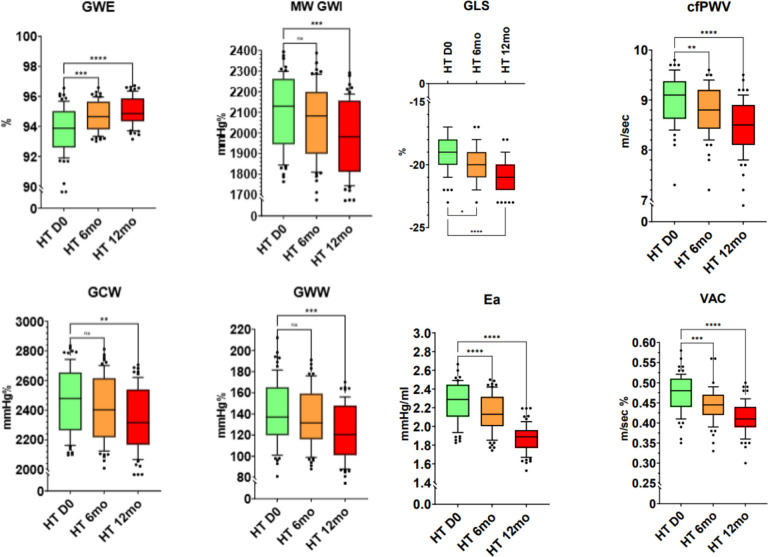 Figure 3
Figure 3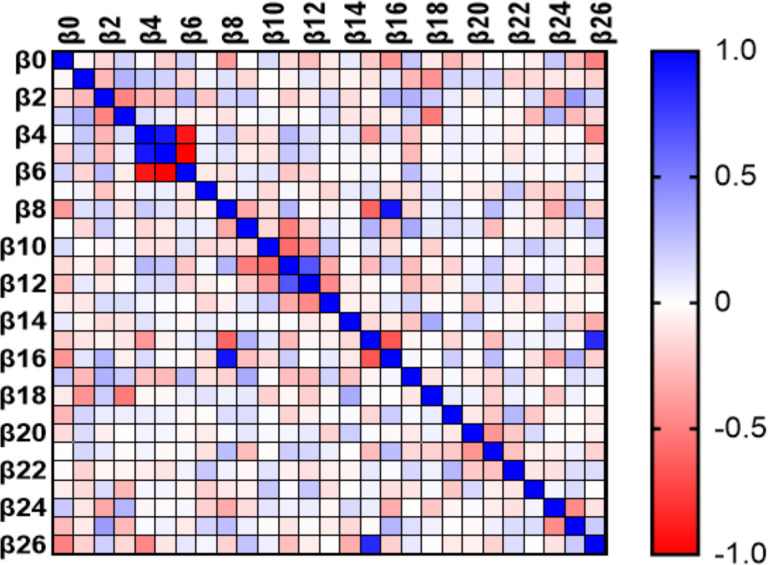 Figure 4
Figure 4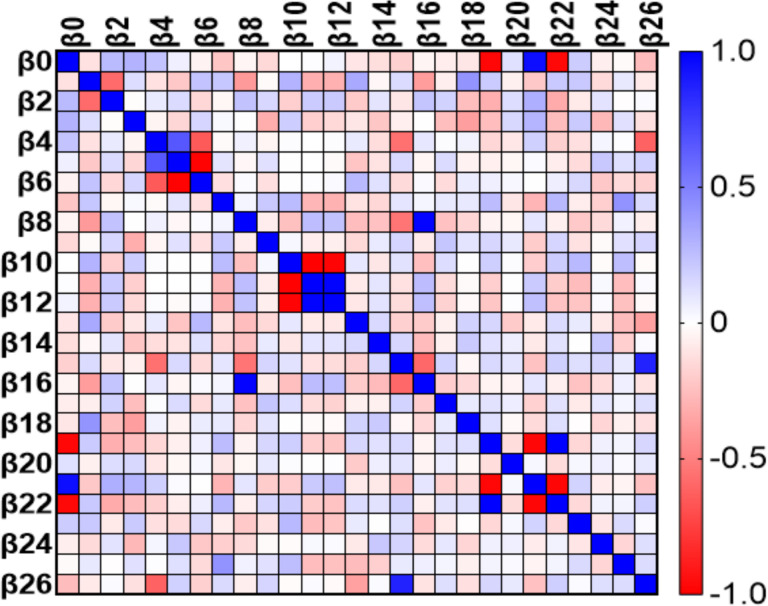 Figure 5
Figure 5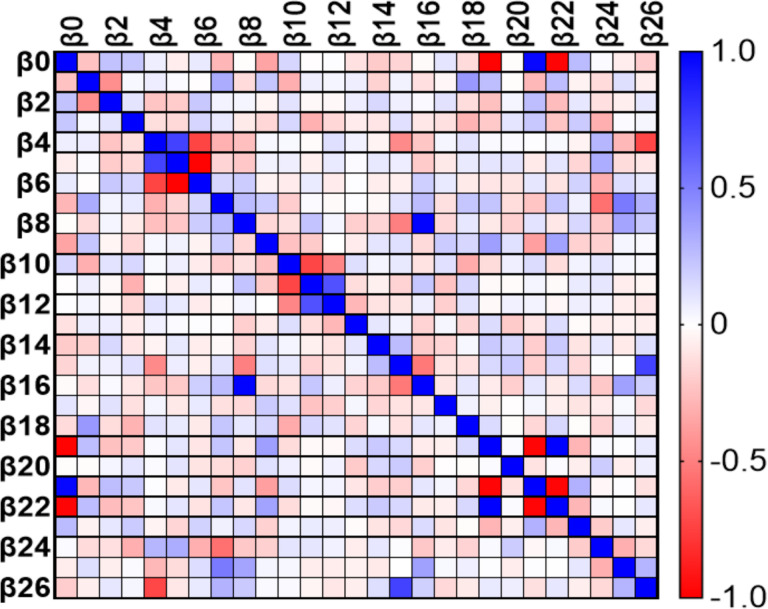 Figure 6
Figure 6Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCardiovascular Health and Disease Prevention · Heart Rate Variability and Autonomic Control · Blood Pressure and Hypertension Studies
Introduction
Ventricular-arterial coupling (VAC), defined as the ratio of two elastances, represents the relationship between the heart and the arterial system. This parameter (measured invasively or non-invasively) is altered by aging and following cardiovascular pathologies, indicating a deterioration of ventricular contractile function (myocardial dysfunction) and/or a stiffening of the arterial system (arterial stiffness). VAC can be calculated by various mathematical formulas, one of which is given by the ratio between the velocity of the arterial pressure wave (pulse wave velocity, PWV), estimated by various methods – including by vascular ultrasound through carotid-femoral pulse wave velocity (cfPWV) – and myocardial contractility, assessed through echocardiographic calculation of global ventricular deformation (global longitudinal strain, GLS).^1^
As myocardial work (MW) represents the force that the heart exerts, by means of the contraction of cardiomyocytes, its assessment offers an additional means to evaluate cardiac performance in relation to energy expenditure, influenced by arterial afterload (aortic pressure) and stroke volume (SV), across various clinical scenarios.^2^
This retrospective observational pilot-study was focused on middle-aged individuals recently diagnosed with early-stage hypertension [Stage I according to the 2024 European Society of Cardiology (ESC) guidelines] without organ damage (Suppl. Figures 1 & 2). Given that the parameters VAC, cfPWV, GLS, arterial elastance (Ea) and MW [in all its components: global work index (GWI), global constructive work (GCW), global wasted work (GWW), and global work efficiency (GWE)] have been primarily studied in cardiovascular diseases of aged populations, we sought to demonstrate whether these parameters were also altered in the early stages of arterial hypertension in middle-aged individuals. Additionally, we assessed whether normalization of blood pressure (BP) through lifestyle changes and/or anti-hypertensive drug treatment would lead to normalization of these parameters.^3–5^
Material and Methods
Study design.
This was a retrospective observational study. The medical records for three years (from 1 March 2021 to 1 March 2024) were screened in the Terni Health District and in other public health districts of the Umbria region (Italy). The study was approved by the Umbria Regional Ethics Committee (protocol nr. 4744/24) and by the Asl Umbria 2 (by executive decision nr. 0003982). The primary outcome was to evidence that lifestyle changes and antihypertensive therapy normalize the ultrasound parameter VAC in recently diagnosed, early stage hypertensives (HTN) without organ damage. The secondary outcomes were (a) demonstration that the non-invasively assessed ultrasound parameters - VAC, Ea, cfPWV, GLS, MW - show worse values in recently diagnosed early-stage HTN without organ damage compared to healthy individuals (normotensives, NT), and (b) demonstration that lifestyle changes and antihypertensive therapy normalize the parameters Ea, cf PWV, GLS, MW.
Study protocol.
The study is divided in two parts. In the first part, recently diagnosed middle-aged early stage HTN, diagnosed within 3 months of the first cardiological visit without organ damage, were compared to NT. Selected patients were divided into two groups: group A (HTN) and group B (NT) at day 0 (zero). Both groups had the same range of age (30–49 years old), sexes and were enrolled by inclusion and exclusion criteria. In the second part, only HTN were investigated by the 2^nd^ and 3^rd^ cardiological visits (two 6 months follow-ups). Cardiological visits (case history and physical examination), general, clinical, electrocardiographic, echocardiographic and echo vascular parameters were assessed at day 0 and at the two follow-ups; laboratory data were assessed in this study only once, at day 0, as part of exclusion criteria (Suppl. Fig. 3).
Participants:
A total of 672 medical records (493 pts excluded at 1st cardiological visit, 53 pts excluded between 1^st^ and 2^nd^ cardiological visit) were analyzed, and 126 patients selected according to the selection criteria of the study. HTN were defined as clinic systolic blood pressure (SBP) range 140–159 mmHg; diastolic blood pressure (DBP) range 90–99 mmHg. NT [normal or elevated blood pressure (BP) individuals, but not hypertensive individuals] were defined as normal clinic BP (< 140 mmHg SBP and < 90 mmHg DBP).
inclusion criteria:
30–49 years old pts of both sexes (HTN and NT); HTN selected had high BP at 1^st^ cardiological visit or within three months from the 1^st^ cardiological visit (assessed at the patient’s home or by family or occupational physician); HTN selected had to be included in the I stage (early stage) hypertension: SBP range 140–159 mmHg; DBP range 90–99 mmHg.
Exclusion criteria:
Individuals with hypertension over three months by the 1st cardiological visit; Individuals with a remote history of hypertension; SBP > 160 mmHg and/or DBP > 100 mmHg; HTN with evidence of increased BP during the study (BP assessed during the follow-up cardiological visit or at home > 160/100 mmHg); Altered laboratory parameters: Hemoglobin (Hb) < 12 g/dl (female) < 14 g/dl (male) or > 16 g/dl (female) > 18 g/dl (male); White Blood Cells (WBC) < 4000/mm^3^ or > 10000/mm^3^; Platelets (PLT) < 150000/mm^3^ or > 400000/mm^3^; creatinine > 1 mg/dl; Glomerular Filtration Rate (GFR) < 60 ml/min/1.73 mq, albuminuria > 30 mg/g; natremia < 130 mEq/l or > 146 mEq/l; kalemia < 3,3 mEq/l or > 5,2 mEq/l; glycemia < 60 mg/dl or > 100 mg/dl; total cholesterol > 200 mg/dl; trygliceridemia > 150 mg/dl; low-density lipoproteins (LDL) > 115 mg/dl; high-density lipoproteins (HDL) < 35 mg/dl; Altered electrocardiographic parameters: no sinus rhythm; electrocardiographic criteria for left ventricular (LV) hypertrophy; Altered echocardiographic parameters: LV mass index > 115 g/m^2^ (male) > 95 g/m^2^ (female), interventricular septum thickness (IVST) > 11 mm, posterior wall thickness (PWT) > 11 mm, relative wall thickness (RWT) > 0,43, LV end diastolic diameter (LVEDD) > 60 mm, LV end systolic diameter (LVESD) > 45 mm, LV ejection fraction (EF) < 50%, Left Atrial Volume index (LAVi) > 34 ml/mq, E wave/e’ wave ratio (E/e’) > 14; valvular pathologies (moderate or severe stenosis and/or insufficiency); altered echo vascular parameters: carotid Intima-Media Thickness (IMT) > 0,9; presence of carotid plaques; Ankle Brachial Index (ABI) < 0,9 or > 1,4; Individuals with hypertension or cardiovascular organ damage.
Interventions/Procedures:
HTN were recommended lifestyle changes and anti-hypertensive medication (medication recommended if BP not normalized). No invasive interventions or procedures on patients was performed.
Measurements:
In the assessment of the medical records, the following parameters were collected. General and clinical parameters: Age, Gender, SBP, DBP, Mean Arterial Pressure (MAP), Body Surface Area (BSA), current smoking, current drinking; Laboratory parameters: Complete Blood Count (CBC), creatinine, GFR, albuminuria, natremia, kalemia, glycemia, complete lipid profile: total cholesterol, triglyceridemia, LDL, HDL; Electrocardiographic parameters: sinusal rhythm, heart rate (HR), electrographic signs of LV hypertrophy; Echocardiographic parameters: LV mass index, IVST, PWT, RWT, LVEDD, LVESD, EF, SV, Stroke volume index (Svi), LAVi, E/e’, MW (GWI, GCW, GWW, GWE), GLS; Echo vascular parameters: carotid IMT, presence of carotid plaques, cfPWV, ABI. BP was determined by brachial BP measurements reported in the medical record. HR was calculated by electrocardiogram. BSA was calculated by the Mosteller equation. VAC and Ea were calculated as VAC = cfPWV / GLS and Ea = (SBP × 0,9) / SV, respectively.
Assessment of BP.
In all cardiological visits the patients were asked to relax for 15 minutes in a quiet room before measuring their BP (office BP), after which their weight and height were measured in order to calculate the BSA. SBP and DBP were measured three times using a sphygmomanometer and the average of the three measurements was used.
Day zero:
On day zero, the first cardiological visit assessed that 179 people were considered valid for inclusion. Between the 1^st^ and the 2^nd^ visits 53 pts were excluded. Of these 126 selected individuals, 68 were included in the group A (HTN), 58 in the group B (NT). In both groups, smokers and alcohol binge individuals (drinkers) were identified: group A 68 HTN participants, 38/68 smokers, 12/68 drinkers; group B 58 NT participants, 1/58 smokers, 0/58 drinkers.
6 and 12 months follow up:
Six months lifestyle changes were recommended to HTN (stop smoking, stop alcohol intake, reduce salt intake, foster weight loss, 30 minutes five times a week of moderate intensity aerobic exercise). After a period of 6 months, in HTN group, if SBP kept on being in the range 140–159 mmHg and DBP in the range 90–99 mmHg, antihypertensive drug therapy was administered (monotherapy or dual). In this study, the antihypertensive drug administered was ACE inhibitor Perindopril (at a dosage of 5 mg/day). The dual drug therapy administered was Perindopril/Amlodipine, at a dosage of 5 mg/5 mg per day. In the first follow-up at the 2^nd^ cardiological visit (6 months after day zero), after lifestyle changes, of the 68 HTN, 12/68 had a normalization of BP; 56/68 HTN were required to start drug antihypertensive treatment: 29 out of 56 HTN in monotherapy; 27 out of 56 HTN in dual therapy. 53 HTN were excluded in the 1^st^ follow-up at the 2nd cardiological visit.
After the first cardiological visit one patient stopped smoking and one patient stopped habitual use of alcohol. In the second follow-up at the 3^rd^ cardiological visit (12 months after day zero) it has been assessed that the 12 HTN with normalization of BP at the first follow-up maintained normal BP, the 56 HTN treated with medication continued to take antihypertensive therapy and no HTN were excluded at the 2^nd^ cardiological follow-up. After the 2^nd^ cardiological visit an additional two patients stopped smoking and two patients stopped habitual use of alcohol.
Statistical analysis:
Statistical analysis was performed using Graphpad Prism Ver. 10.3.0 (GraphPad Software, San Diego, California, USA). In the first part of the study continuous variables with a normal distribution were expressed as mean ± SEM and HTN compared to NT using 2-way ANOVA. In the second part, 1-way ANOVA was used and multiple linear regression was performed to assess the impact of each variable on VAC. A value of p < 0.05 was considered statistically significant.
Results
Out of 672 medical records, 126 individuals (aged 30–49 years old) were selected and included in this retrospective observational pilot-study (Table 1). They were divided in two groups: group A (HTN) and group B (NT). In HTN compared to NT, an increase in SBP, MAP, HR, MW GWI, MW GCW, and MW GWW was observed. There was a trend of increased values for DBP (Table 2). In HTN, at day 0 (zero) and after the two follow-ups, the results of clinical and echographic parameters were as follows (Fig. 1, 2, 3). A decrease was observed in the values of SBP at 12 months, DBP at 6 and 12 months, MAP at 6 and 12 months, and HR at 6 and 12 months. Despite the positive trend towards improvement at 6 months for SBP, this did not reach a significant reduction. In HTN, the echocardiographic parameters identified an increase in EF and SV/Svi at 12 months and a reduction in LAVi at 12 months (Fig. 2).
In HTN, a reduction in GWI, GCW, and GWW in the investigated MW components at 12 months and an improvement in GWE at 6 and 12 months were observed. Despite the trend at 6 months of a reduction in GWI, GCW, and GWW, none reached statistical significance. In HTN, a reduction in GLS, cfPWV, Ea, and VAC was observed at 6 and 12 months (Fig. 3).
At day 0, the variables MW GWI, MW GWW, current drinkers, and E/e’ were linearly related to VAC (Fig. 4). At 6 months the variables BSA, PWT, RWT, LVEDD, SVi, GLS, and cfPWV were found to be linearly related to VAC (Fig. 5). At 12 months the variables GLS, and cfPWV were linearly related to VAC (Fig. 6). Analysis indicated a strong trend to linear correlation to VAC for BSA, SBP, DBP, MAP, and Ea, although none were statistically significant.
Discussion
In our study, we found no difference in VAC between HTN and NT groups. Along with HR and BP specifically SBP and MAP (with a positive trend towards significance for DBP), MW (in its components GWI, GCW, and GWW) was found to be higher in HT than NT. By assessment of the HTN group at the two follow-ups at 6 and 12 months, BP, EF, MW (in its components GWI, GCW, and GWW), VAC, Ea, cfPWV and GLS were significantly improved. Analysis of the impact of VAC on the parameters investigated in this study highlighted that VAC was linearly related to cfPWV and GLS after lifestyle changes and hypertensive drug treatment. In addition to cfPWV and GLS, MW (in its components GWI and GWW), current drinking and E/e’ were found to be linearly related to VAC at day 0, whereas the variables BSA, PWT, RWT, LVEDD, and SVi, were found to be linearly related to VAC at 6 months.
Notwithstanding no significant difference in VAC, significant difference in BP, HR and MW was observed between the two groups, highlighting the pre-clinical role of an increase in sympathetic activity in the onset of hypertension even in middle-aged HTN. Furthermore, along with EF and GLS, MW components were valid indicators of LV systolic function, even at the early onset of hypertension, providing a more comprehensive appraisal of LV systolic function.^6,7,8^
Despite the positive trend of lifestyle changes at 6 months, the improvement of the parameters VAC, Ea, MW, cfPWV, EF, and GLS was more evident after the onset of antihypertensive therapy, demonstrating the benefit of a further reduction in BP. These data align with the current guidelines on further restricting BP in terms of normal ranges, highlighting the paramount impact of BP in the management of sub-clinical hypertension.^9^
As a consequence of the improvement of VAC, Ea, MW, cfPWV, EF, and GLS by lowering of BP and HR and changes in lifestyle (such as body weight loss, physical exercise, smoking cessation and reduction in salt and alcohol consumption), the improvement in systolic function by reduction of sympathetic overdrive and its significant effect on BP and HR was evidenced. In addition to aging as an independent contributor to the deterioration of diastolic function, the significant correlation between the echocardiographic parameter E/e’ ratio and VAC in HT was observed by echocardiographic signs of an early effect of high BP values on diastolic function.^10,11^
Despite no statistically significance, the increase in VAC in the young hypertensive population compared to the healthy individuals was based on an increase in cfPWV and a reduction in GLS. The two determinants cfPWV and GLS for the calculation of VAC were found significantly related to VAC at 6 and 12 months, easily predictable as VAC = PWV / GLS, deducing that simultaneously arterial stiffness and LV systolic function are progressively altered.^12,13^ This is dependant upon the progressive hardening of the arteries by aging (mostly in the population with exposure to risk factors such as tachycardia, high BP and smoking) that determined a progressive increase in the pulse wave transmission with consequent effect given by the return to the heart of the anterograde pulse wave at an earlier time point during the late systolic phase of the cardiac cycle. As a consequence of this, constantly increased afterload affected a progressive impairment of cardiac function with progressive reduction of GLS.^14^ Concerning the effect of medical treatment on BP, BP control occurred with antihypertensive drugs in monotherapy and dual therapy. As predictable, dual drug antihypertensive treatment was more effective in reducing both BP and VAC compared to single drug antihypertensive treatment.^3,9^
As demonstrated by other research, VAC was associated with the prevalence of both hypertension and other cardiovascular risk factors, such as active smoking, alcohol consumption, and increased HR, highlighting reports that it is the most significant predictor of risk.^1,15,16^ In agreement with the studies of Holm H et al. and Stoichescu-Hogea G et al., VAC and cfPWV were found higher and GLS lower than in the control population. The former was found to be especially associated with age and active smoking; the latter found to be worse in coronary artery disease and HTN vs HTN vs group control. Compared to the aformentioned studies, the investigated population in our study did not have additional cardiovascular risk factors or organ damage, highligthing that in early stage of hypertension these parameters were not statistically significant.^2,12,13,15,17,18^ The finding of no significant difference in VAC was mainly due to the small sample size and lack of longitudinal analysis in NT. Furthermore, as the investigated population was not elderly and without cardiovascular diseases, it was demonstrated that this parameter was not altered in middle-aged HTN at early stage of hypertension. As left VAC represents both a parameter that characterizes the energetic cost, particularly when the LV function is changed, and a hemodynamic measure linked to patient outcomes,^19,20^ this highlights the importance of observing small changes in the pre-clinical context, such as arterial hypertension without organ damage.^1^ On the other hand, in the population studied, MW was demonstrated to be sensitive to impairment even in young HTN, highlighting it to be more affected at early stages from augmentations in sympathetic increases in BP and HR. In addition, as MW was observed to be statistically higher in HT without other cardiovascular risk factors or organ damage, this parameter can account for BP and myocardial energy consumption at the onset of hypertension and not only in overt cardiovascular diseases.^2,10,21^
The NORRE substudy, was the first to offer data on age-related changes in GWI and GCW among both males and females. In women, values increased, whereas in men, they remained unchanged, with an increase primarily associated with elevated SBP alone. Additionally, GWW and GWE values were found to increase in men and decrease in women, with no significant age-related differences (Table 6).^22^ GWI represents the area within the LV loop quantifying the work performed by the LV throughout the entire mechanical energy between MVC and MVO; GCW represents the positive work performed by shortening during IVC and systole and the negative work by lengthening during filling, quantifying the energy consumed by the myocardium that effectively contributes to CO; GWW represents negative work by lengthening during IVC and systole and positive work by shortening during IVR, quantifying the wasted energy by the myocardium that does not contribute to CO. As a consequence of this, to complete the mechano-energetic study, the assessment of MW adds, through its components (GWI, GCW, GWW, GWE), a greater definition of myocardial energy expenditure both in the evaluation of the amount of MW performed by the left ventricle during systole and the amount of MW that participates or does not in ejection. We observed that at early stage of arterial hypertension, GWI, GCW, GWW are higher indicating an increase in MW expenditure. Through lifestyle changes and anti-hypertensive drug treatment, these parameters tend to be renormalized, indicating a better mechano-energetic efficiency.^2^ Therefore, myocardial mechano-energetic efficiency represented as a surrogate of MW was found to be more sensitive and with higher impact than VAC and other parameters studied at early stage of hypertension in middle-aged HTN.^18,21,23^
Used with permission from Dr. Federica Ilardi, April 8, 2024.
In light of these results, in addition to BP and HR controls, the sub-clinical assessment of LV systolic and diastolic functions can be investigated in clinical practice in young people at early stage of hypertension by calculating MW and the E/e’ ratio, respectively. Longitudinal studies with larger sample of young HT could provide additional robust results in order to define the significant role of VAC and the other parameters investigated in this study in terms of cardiovascular prevention for more accurate management and assessment in clinical practice.
Limitations of the study
This study has several limitations. The number of people investigated was small and the timeframe brief. A longitudinal study on the healthy population was not performed, so that the HTN and NT groups were not compared at 6 and 12 months. Also, VAC was non-invasively calculated. This study did not analyze all stages of hypertension and HT with organ damage.
Conclusions
VAC was found to be advantageous in early stage middle-aged HT for the assessment of the cardiovascular system. In addition to VAC, the parameters Ea, MW, cfPWV, GLS, and EF were highlighted to be altered even in early stage of hypertension and statistically improved after lifestyle changes or antihypertensive drug treatment. Since hypertension is both an important independent risk factor for cardiovascular disease and endothelial dysfunction, this study highlights the clinical impact of cardiovascular prevention in young HT, particularly in active smokers and drinkers with increased HR. Despite VAC being easily determined at the patient’s bedside, it still remains neglected. Further studies are needed to demonstrate the effective introduction of this parameter into clinical practice.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Vitali A, Zouein FA, Booz GW, Altara R. Prognostic Utility of Assessing Ventricular-Arterial Coupling in Arterial Hypertension and Cardiovascular Diseases. Minerva Cardiology and Angiology 2024–5.10.23736/S 2724-5683.24.06655-939846964 · doi ↗ · pubmed ↗
- 2Vitali A, Zouein F A, Booz G W, Altara R. Clinical Utility of Myocardial Work Assessment in Arterial Hypertension and Cardiovascular Diseases. Minerva Cardiology and Angiology 2024–5.10.23736/S 2724-5683.24.06654-739881632 · doi ↗ · pubmed ↗
- 3Kelly MS, Dacey A, Siana A, Ojeda J. Efficacy and Safety of a Polypill to Reduce Cardiovascular Events: A Review of Clinical Trials. J Cardiovasc Pharmacol 2024; 83(1): 8–15.37924288 10.1097/FJC.0000000000001508 · doi ↗ · pubmed ↗
- 4Zhao Y, Wang L, Huang Y, Evans PC, Little PJ, Tian X, Weng J, Xu S. Anthocyanins in Vascular Health and Disease: Mechanisms of Action and Therapeutic Potential. J Cardiovasc Pharmacol 2024; 84(3): 289–302.39240726 10.1097/FJC.0000000000001602 · doi ↗ · pubmed ↗
- 5Chilbert MR, Woodruff AE, Rogers KC. A Practical Guide to Understanding and Treating Peripheral Artery Disease. J Cardiovasc Pharmacol 2024; 83(6): 565–579.38452186 10.1097/FJC.0000000000001556 · doi ↗ · pubmed ↗
- 6Loncaric F, Marciniak M, Nunno L, Mimbrero M, Fernandes JF, Fabijanovic D, Sanchis L, Doltra A, Montserrat S, Cikes M, Lamata P, Bijnens B, Sitges M. Distribution of myocardial work in arterial hypertension: insights from non-invasive left ventricular pressure-strain relations. Int J Cardiovasc Imaging 2021; 37(1): 145–154.32789553 10.1007/s 10554-020-01969-4 · doi ↗ · pubmed ↗
- 7Russell K, Eriksen M, Aaberge L, Wilhelmsen N, Skulstad H, Remme EW, Haugaa KH, Opdahl A, Fjeld JG, Gjesdal O, Edvardsen T, Smiseth OA. A novel clinical method for quantification of regional left ventricular pressure-strain loop area: a non-invasive index of myocardial work. Eur Heart J 2012; 33(6): 724–733.22315346 10.1093/eurheartj/ehs 016PMC 3303715 · doi ↗ · pubmed ↗
- 8Flachskampf FA, Chandrashekar Y. Myocardial Work and Work Index: Related But Different for Clinical Usage. JACC Cardiovasc Imaging 2022; 15(8): 1521–1523.35926913 10.1016/j.jcmg.2022.07.001 · doi ↗ · pubmed ↗