More schooling is associated with lower Hemoglobin A1c at the high-risk tail of the distribution: An unconditional quantile regression analysis
Jillian Hebert, Amanda Irish, Aayush Khadka, Abigail Arons, Alicia R. Riley, Elbert S. Huang, Anusha M. Vable

TL;DR
Higher education is linked to lower blood sugar levels, especially for people at higher risk of diabetes.
Contribution
This study reveals that the protective effect of education on blood sugar levels is strongest at higher risk levels.
Findings
Among those with 12+ years of schooling, each additional year of education was linked to lower HbA1c levels.
The effect of education on HbA1c was strongest at higher quantiles of the distribution.
16.6% of participants had HbA1c levels above the diabetes diagnostic threshold.
Abstract
Risk of diabetes increases exponentially with higher levels of glycosylated hemoglobin (HbA1c). Education is inversely associated with average HbA1c, however, differential associations between education and HbA1c across the HbA1c distribution have not been evaluated. Health and Retirement Study data (N=21,732) was used to evaluate the association between education (linear terms among those with <12 years and ≥ 12 years of education) and first recorded HbA1c (2003–2016) at the mean using linear regression, and at the 1st-99th quantiles of the marginal outcome distribution using unconditional quantile regressions, controlling for birth year, race and ethnicity, gender, birthplace, parent’s education, and year of HbA1c measurement. Mean HbA1c was 5.9%; 16.6% of participants had HbA1c above the diabetes diagnostic threshold of 6.5%. For those with less than 12 years of schooling, there…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
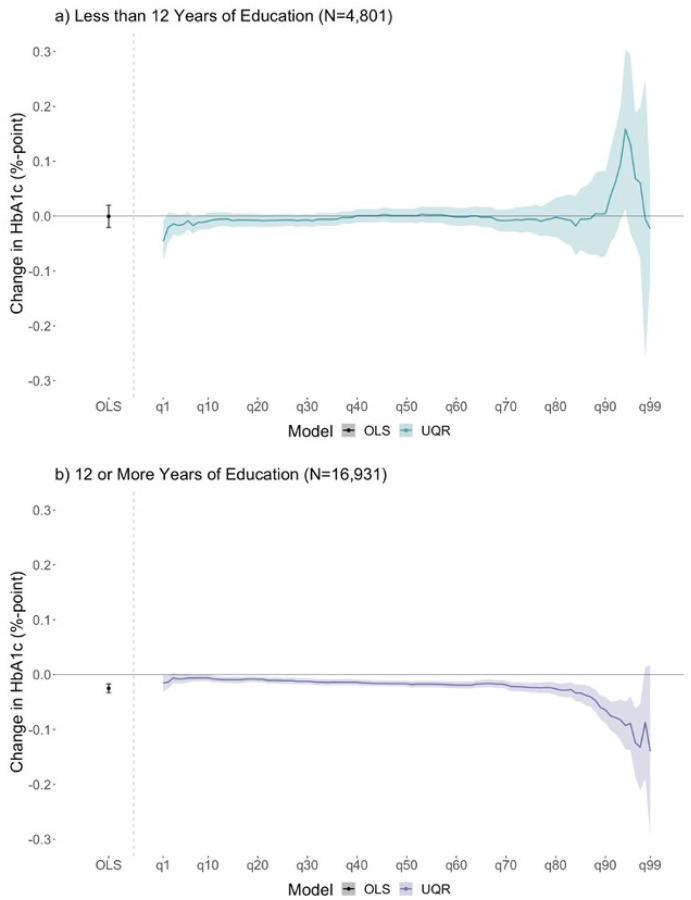 Figure 1
Figure 1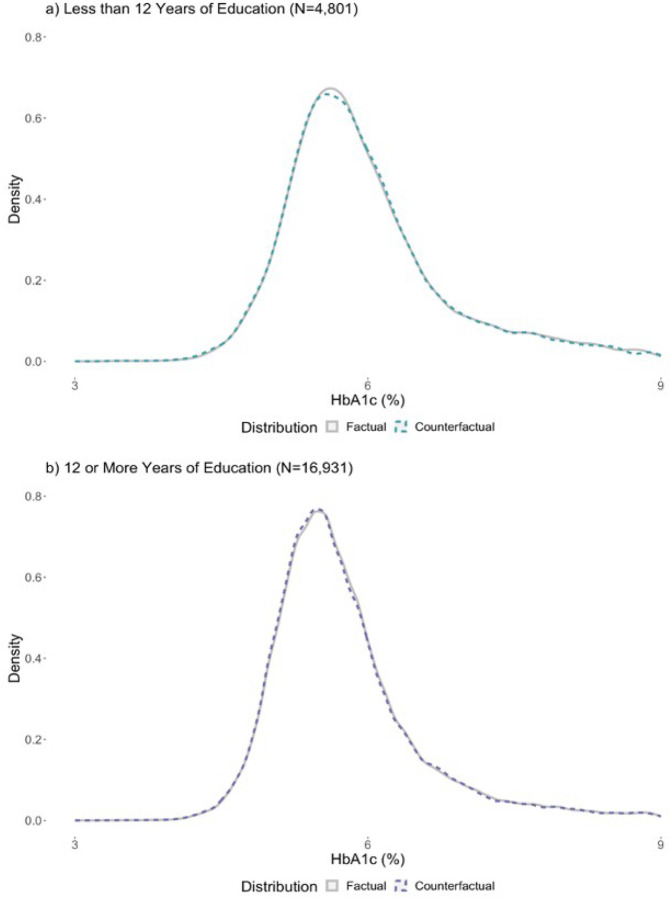 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsLiver Disease Diagnosis and Treatment · Health disparities and outcomes · Global Health Care Issues
Introduction
Prior work, both in the US and globally, reveals a strong inverse relationship between educational attainment and average glycosylated hemoglobin (HbA1c), an index of glucose regulation over the past 2–3 months, such that those with less education are at higher risk of diabetes and diabetes-related complications.^1–6^ Among people with diabetes, glycemic control is essential for reducing complications, such as kidney failure, cardiovascular events, and all-cause mortality;^7–11^ in parallel, staying within normal ranges of HbA1c is important to prevent diabetes onset and related complications. Risk of diabetes complications increase exponentially with HbA1c, such that a percentage-point increase at a higher level of HbA1c (e.g. 6% to 7%) confers a much greater risk for diabetes-related complications compared to a percentage-point increase at lower HbA1c levels (e.g. 4% to 5%). Therefore, exposures and interventions that have larger impacts for those with higher HbA1c may be important for preventing diabetes-related complications.
Education, a main component of socioeconomic status, is consistently associated with better health over the lifecourse.^12–13^ Increased educational attainment may impact HbA1c through several pathways, including longer life expectancy, increased income, better access to healthcare, and more health promoting behaviors (e.g., increased physical activity).^1,4,14–16^ While evidence suggests a strong protective association between educational attainment and mean HbA1c, no study evaluates the association across the entire HbA1c distribution. Evaluating if the relationship is constant across the HbA1c distribution is important, given the exponential relationship between HbA1c and diabetes onset and related complications. Interventions that specifically impact high levels of HbA1c are of interest given their potential to reduce diabetes onset and related complications. We hypothesize education will have larger associations among those with higher HbA1c as participants belonging to more structurally minoritized subgroups (e.g., minoritized due to race, or poverty status) will be over-represented at the high-risk end of the HbA1c distribution (i.e., higher quantiles of the HbA1c distribution),^17–19^ and these same groups also seem to benefit more from education.^45–47^
We add to existing literature by evaluating the relationship between education and HbA1c across the HbA1c distribution through a novel application of quantile regression, a modeling technique that evaluates the exposure-outcome relationship across the outcome distribution. Quantile regressions can identify if educational attainment has a heterogeneous effect across the HbA1c distribution, which allows for discovery of whether, and which parts of, the HbA1c’s distribution are differentially impacted by educational attainment. In this way, our application of quantile regression to the education-HbA1c relationship has the potential to deepen our understanding of educational inequities in diabetes by uncovering details hidden by linear regression.
This paper empirically evaluates the relationship between educational attainment and late-life HbA1c using linear regression and unconditional quantile regressions (UQR) for US Health and Retirement Study participants ages 50 and older, examining whether the relationship between education and HbA1c varies across the HbA1c distribution. We stratify education at 12 years, where 12 years of schooling typically confers a high school diploma, since prior literature finds evidence for divergent health trajectories of adults with less than a high school education from those with high school or more.^20^
Methods
Data and Analytic Sample
Data came from the U.S. Health and Retirement Study (HRS), a national longitudinal sample of non-institutionalized adults 50 years and older, and their spouses of any age, that began in 1992.^21^ New cohorts of participants have been added every six years after 1998 to maintain a steady state population, and participants are surveyed biennially. A diabetes sub study collected HbA1c for a subset of HRS participants in 2003; in addition, HbA1c and other biomarker data was collected in 2006 for a randomly selected half of the sample, and in 2008 for the other half; biomarker data were subsequently collected every four years.
The eligible sample included all HRS participants with at least one HbA1c measurement between 2003 and 2006 when they were 50 years or older (N = 21,840). Individuals were excluded for missing exposure (N = 89) and covariate data (N = 18); one participant was removed due to their HbA1c measurement being recorded prior to their first HRS interview, resulting in an analytic sample of 21,732 participants (99% of eligible).
Exposure
Our exposure, educational attainment, was created using self-reported total years of schooling. Education in HRS ranges from 0 to 17 years of schooling, where 17 years includes those with 17 or more years of education (17 or more years: N = 2,327). Due to data sparseness of participants with fewer than 5 years of education, we coded those with less than 5 years of education to 5 years to reduce the impact these outliers may have on estimates (N = 776). To assess possible heterogeneities between participants with different types of credentials, and since educational policies tend to target specific levels of education (e.g. compulsory schooling laws and child labor laws targeted K-12 education, while other policies only addressed college education), education was stratified into two levels: fewer than 12 years of education (N = 4,801; 22%) and 12 or more years of education (N = 16,931; 78%), where completing 12 years of education typically corresponds to earning a high school diploma. Education was modeled linearly within these two educational strata.
Outcome
Our outcome was the participant’s first recorded HbA1c value (2003–2016) measured at or after age 50. HbA1c is glycosylated hemoglobin and reflects blood glucose over the prior 2–3 months; HbA1c values between 5.71% and 6.49% are consistent with pre-diabetes and values greater than 6.5% are consistent with diabetes.^22–24^ HbA1c was measured using an automated ion-exchange high-performance liquid chromatography that recorded the percentage of glycosylated hemoglobin in dried blood spot samples.^21^
Covariates
All models were adjusted for sex (female; male), race (Non-Hispanic White; Non-Hispanic Black; Latinx/Hispanic; other), birthplace (non-Southern US; Southern US; Foreign), indicator for birth year (1905–1966), indicator for year of HbA1c measurement (2003–2016), mother’s education (5–17(+) years, linear), father’s education (5–17(+) years, linear), as well as missing indicators for mother’s education and father’s education. Sex was included as an indicator of the socially stratifying effects of gender,^25^ race as an indicator of the socially stratifying effects of systemic racism,^26–27^ and parent’s education as a proxy for childhood socioeconomic status. Chi-square tests were used to evaluate if there were significant differences in categorical covariates by education level (e.g., less than 12 years of education versus 12 or more years of education). See supplemental Table S1 for additional details on covariates.
Race was categorized to include an “other” category in all models for precision, but results were not reported for this group due to the heterogeneous composition and consequent lack of interpretability of estimates.
Birthplace was classified by location within the US (i.e., non-Southern vs Southern) because studies have found increased risk for adverse later-life health outcomes for those born in the Southern US.^28–31^ A subset of participants (N = 414, 2%) were known to be born in the US, but were missing information on the region of birth; participants where the region of birth was unknown were assumed to be born in the Non-Southern US.
Birth year was modeled as an indicator variable to capture differences by individual year. Due to a small number of participants falling in the tail ends of the birth year range, values were recoded to facilitate model convergence: those born before 1917 (N = 240, 1%) were recoded as 1917; those born in 1966 (N = 52, 0.2%) were recoded as 1965.
Parental education variables (5–17(+) years) were used as a proxy for family socioeconomic status (SES) and modeled continuously. However, HRS participants in the Asset and Health Dynamics Among the Oldest Old (AHEAD) cohort (born 1900–1923) recorded parent’s education as a dichotomized measure (less than 8 years of education, 8 or more years of education) rather than continuous. Dichotomized measures of parent’s education were replaced with continuous values from a previously validated imputation method using measures of childhood socioeconomic status.^32^ Additional missingness in parent’s education was imputed using the sample mean (mother’s education: N_Missing_ = 2,101 (10%), sample mean = 10 (SD 3.9); father’s education: N_Missing_ = 3,644 (17%), sample mean = 10 (SD 4.2)) and a missing indicator was added for proper model adjustment. This allowed for retention of participants with missing parental education where missingness is informative (e.g., if the parent was not in the household).^33^
Statistical Analysis
We used linear regressions and unconditional quantile regressions (UQR) to model the relationship between education and HbA1c.^34–36^ UQR evaluates changes in quantiles of the outcome’s unconditional distribution for a one-unit change in the mean of the exposure. We estimated parameters of the linear regression model using ordinary least squares (OLS). We t UQR models at each unit quantile between the 1st-99th quantiles of the unconditional HbA1c distribution. We used bootstrapping (500 repetitions) to estimate 95% confidence intervals (CIs) for parameters of the linear regression and UQR models; education was modeled as a linear term within both education strata and all models were adjusted for the covariates specified in the preceding section.
To visualize the change in the sample distribution of HbA1c implied by UQR results, we created plots to show the counterfactual HbA1c distribution for a one-year increase in the sample’s mean education. First, we binned the factual, or observed, data into quantiles (1st-99th). We then added the UQR estimation of the association between education and HbA1c to the observed data by quantile, creating a potential counterfactual distribution. Finally, we plotted the observed and counterfactual distributions. Further details about constructing these datasets and plots are provided elsewhere.^36^
Sensitivity Analysis
We conducted three additional analyses to see if results were robust to different analytic decisions. First, to determine if results were sensitive to how the exposure was operationalized (i.e., coded for analysis), we re-coded education as a three category variable (<12 years, 12–15 years, and 16 or more years of education) rather than two. Second, given that the HRS collects data from numerous birth cohorts (from 1905–1966) and given that educational attainment has tended to increase over time, we conducted analyses stratified by HRS entry cohort (which are defined by the HRS using participant’s birth year), to test the sensitivity of the association to secular trends in education. Finally, while medication could be an important contributing factor in the education-HbA1c relationship, medication usage is downstream from education and is therefore a potential mediator of the education-HbA1c relationship. Adjusting for mediators can bias estimates,^37^ so the main analyses did not include adjustment for medication.
Software and Code
All data cleaning and analysis was performed in R.^38^ We used the dineq package for fitting UQRs. All code was reviewed by the second author as recommended practice^39^ and can be found on GitHub.
Results
Participants included in analysis (Table 1) had an average of 13 years of education, were predominantly women (57%), White (65%), and born in the non-Southern US (53%). Most participants self-reported having 12 or more years of education (78%) and median HbA1c (Interquartile Range - IQR) in the overall sample was 5.7% (5.3%-6.2%). Compared to participants with 12 or more years of education (henceforth 12+ years), those with less than 12 years of education (henceforth < 12 years) were older (mean age: 67 vs. 65), had higher proportions of Black and Latinx participants (23% vs. 17% Black; 31% vs. 8% Latinx), had a higher proportion of Southern US birthplace (42% vs. 31%), and had lower parental education (mean mother’s education: 8 vs. 11; mean father’s education: 8 vs. 10) with higher rates of missingness (20% vs. 7% missing mothers education; 30% vs. 13% missing father education). Median HbA1c (IQR) for < 12 years was 5.8% (5.5%-6.4%) and 5.6% (5.3%-6.1%) for 12+ years. Chi-square tests found significant differences in race and ethnicity, birthplace, proportion missing parent’s education, and proportion of the sample with HbA1c levels that are consistent with being pre-diebetic or having diabetes.
Figure 1 displays linear regression and UQR results for both education strata (<12 years; 12+ years). Linear regression results indicate that each additional year of education was not associated with average HbA1c for participants with <12 years (Figure 1, panel a: −0.00, 95% CI: −0.02, 0.02). UQR results for the 1st-99th quantiles suggest that a one-year increase in mean education was not associated with HbA1c across most quantiles, but may have been associated with higher HbA1c at higher quantiles (91–97th quantiles), although the confidence intervals here were wide (Figure 1, panel a: b_q5_ = −0.02%; 95% CI: −0.03, 0.03, b_q50_ = 0.00; 95% CI: −0.01, 0.01, b_q95_ = 0.13%; 95% CI: −0.03, 0.29).
For participants with 12+ years, linear regression results indicate that each additional year of education was associated with lower average HbA1c (Figure 1, panel b: −0.02, 95% CI: −0.03, −0.02). UQR results suggest that a one-year increase in mean education was associated with lower HbA1c across almost all quantiles with a larger magnitude at higher quantiles (90–99th quantile) (Figure 1, panel b; b_q5_ = −0.01%; 95% CI: −0.02, −0.00, b_q50_ = −0.02%; 95% CI: −0.02, −0.01, b_q95_ = −0.09%; 95% CI: −0.14, −0.04).
Figure 2 illustrates the factual, or observed, distribution of HbA1c in the sample and the predicted reshaping (i.e., counterfactual) of the HbA1c distribution based on the UQR estimates. Figure 2 helps to visualize the potential impact of increased education on the HbA1c distribution (i.e., the counterfactual distribution). Consistent with the magnitude of the UQR estimates in Figure 1, changes in the counterfactual HbA1c distribution are small and therefore dificult to discern; to aid in visualization, Figure 2 zooms in on the peak of the HbA1c factual and counterfactual distributions. A figure including the full HbA1c distribution is included in the appendix (eFigure 1). For those with <12 years, the density at the peak of the counterfactual distribution is slightly lower than the density at the peak of the factual distribution, suggesting a small rightward shift away from the densest point of the distribution, towards higher HbA1c values. For 12+ years, the density at the peak of the counterfactual distribution is slightly higher than the density at the peak of the factual distribution, suggesting a small leftward shift in the direction of the densest part of the distribution, towards lower HbA1c values.
Sensitivity analyses
Results were attenuated but substantively similar and conclusions were unchanged when stratifying into 3 education strata (<12 years of education, 12–15 years of education, 16+ years of education) (eFigure 2). Results for 12–15 years of education were most similar to results for the 12+ years of education in the main analysis; results for 16+ years of education were null across most quantiles but were associated with lower HbA1c at higher quantiles (90–98th quantiles).
When evaluating differences by entry cohorts, most results included the null, but estimates were largely in the same direction (eFigures 3–9). The War Babies (birth years: 1942–1947) and Mid Baby Boomer (birth years: 1954–1959) cohort’s results were most dissimilar to the main results.
Results and conclusions were unchanged after additional adjustments for medication (eFigure 10).
Discussion
In the HRS sample of older US adults, we found that the relationship between educational attainment and HbA1c varies by education level and is heterogeneous across the HbA1c distribution. Overall, associations between education and HbA1c seem to be strongest at the high-risk tail of the HbA1c distribution (i.e., participants with the highest HbA1c levels; 90–99th quantiles). That is, participants with the highest HbA1c levels who are most at risk of developing diabetes or experiencing diabetes-related complications such as cardiovascular events and all-cause mortality had the strongest association with educational attainment. We also found that these associations varied by total years of schooling: among those with less than 12 years of education, a one-year increase in mean education was not associated with HbA1c for participants with low to average HbA1c levels, however, it was weakly associated with higher HbA1c for participants with high HbA1c levels. Conversely, among those with 12 or more years of education, a one-year increase in mean education was associated with lower HbA1c across the distribution, with larger magnitudes in the association at the high-risk tail of the distribution; more education was associated with a leftward shift in the HbA1c distribution, suggesting lower risk of diabetes and diabetes-related complications in the sample population. While the associations appear minimal, our work adds to existing literature by demonstrating a method of evaluating heterogeneous relationships and identifying that the relationship between education and HbA1c differs by education level.
There were two analytic decisions that allowed us to identify these novel findings. First, we stratified our exposure at 12 years of education. This stratification was informed by prior research highlighting the divergent health trajectories of adults with less than a high school education from those with high school or more.^20^ Second, we used UQRs to evaluate the relationship across the entire HbA1c distribution, as opposed to evaluating the relationship at the mean, where one assumes the change at the mean is constant across the entire HbA1c distribution. Among older adults with more than 12 years of education, estimates at the mean were associated with lower HbA1c, as were estimates for most of the quantiles in the HbA1c distribution; at the highest quantiles of the HbA1c distribution, magnitudes of the estimates were larger, suggesting that there may be a larger association for those with higher levels of HbA1c. This discovery additionally exemplifies that the mean association was not constant across the entire HbA1c distribution.
Our findings that increased educational attainment was associated with lower HbA1c among those with 12 or more years of education is consistent with prior literature showing that lower educational attainment is associated with increased risk of diabetes and more broadly that detrimental social factors strongly affect risk of diabetes.^1–17^ Our use of quantile regressions revealed a larger magnitude of the education-HbA1c association at the high-risk tail of the HbA1c distribution, where individuals are more likely to have diabetes. We hypothesize two potential mechanisms for this: First, the impact of structural factors (race, poverty, historic systems of marginalization and exclusion) on educational attainment and HbA1c. Evidence shows that education has a larger impact among low childhood socioeconomic status or racial and ethnic minoritized groups, when compared to structurally advantaged groups (e.g., White).^41–44, 47^ Second, is that education impacts skill-level, which, in turn, impacts the type of job one attains and their income. Therefore, individuals with diabetes who have higher levels of education likely also have greater access to resources, such as money, health care and medications, or social and behavioral resources that support lifestyle changes to better manage glucose levels.^40, 45–46^
Our findings about the relationship between HbA1c and education are relevant for both clinicians and public health policymakers. At the clinical level, this association underscores the role of social determinants of health screening as a part of diabetes risk assessment, and future research should explore the added benefit of more precise screening for education in terms of number of years rather than more commonly used broad categories of educational attainment. Such screening and subsequent linkage to social services has the potential to support clinicians in better identifying and supporting patients to lower their risk of diabetes (e.g., pursuing earlier or more intensive preventive intervention or more aggressive glycemic control once diagnosed with diabetes). Additional studies could explore the effectiveness of interventions for these patients that seek to mitigate the detrimental effect of less education on HbA1c, such as disease education programs, navigational supports, and pharmacy management tools. Finally, our results raise the question of whether increasing educational attainment, even by 1 year, for populations would be an effective intervention to reduce future glucose levels. Future secondary data analyses and intervention studies can further elucidate whether individual-level or population-level interventions that increase post-secondary educational attainment may be an effective strategy for lowering diabetes risk.
It is important to contextualize why results for those with less than 12 years of education are different from those with 12 or more years of education, especially because the results for those with less than 12 years of education are contrary to our hypothesis and prior literature. It could be that those with less than 12 years of education are a different, more structurally minoritized group than those with more education, resulting in different relationships between education and HbA1c; we found significant differences in race and ethnicity, birthplace, proportion missing parent’s education, and proportion of the sample with HbA1c levels that are consistent with being pre-diebetic or having diabetes. Our sample of those with less than 12 years of education were more likely to be people of color, born outside of the US or in the Southern US, and their parents had less education or more missing data on education – all potential indicators of increased marginalization. Results could also be due to standard variability in the unconditional quantile regression estimates at the tails of the distribution, where the density is low, and the variance of the RIF is larger.^34^
An important strength of this analysis is the additional information provided by the UQR modeling technique. By looking at the exposure-outcome relationship across the entire outcome distribution, estimates can identify heterogeneities in the education and HbA1c relationship. OLS results only suggest lower HbA1c levels given an additional year of education for participants with 12 or more years of education. UQR results further suggest that the magnitude of change in HbA1c is larger for those at the high-risk tail of the distribution. Comparing the OLS and UQR results highlights the limitation of mean models in capturing an exposure’s relationship with the outcome distribution, and the necessity for evaluating the relationship across the entire outcome distribution, especially when the risk could be non-linear.
There are limitations in these analyses that should be acknowledged. As with any observational study, residual confounding is a potential problem. We did not have information on whether participants had type 1 or type 2 diabetes; inability to differentiate if participants had type 1 or 2 diabetes was a concern given that they are two distinct diseases with unique risk factors and treatments. Additionally, we evaluated educational quantity, and assumed quality was comparable across respondents, potentially resulting in residual confounding in the relationship between educational attainment and HbA1c. We hypothesize that the education-HbA1c relationship could differ by race and ethnicity and sex, due to socially stratifying effects of gender and systemic racism; understanding if there are differential returns to education by sociodemographic subgroup is an important area for future study. Results from HRS underscores that these analyses should be replicated in other data sources to determine if these results are robust to variations in time, place, and population; evaluating if these relationships are causal is also warranted.
Our results suggest the relationship between education and HbA1c is heterogeneous, varying both by education level and across the HbA1c distribution, with the largest associations in the high-risk right tail of the HbA1c distribution where risk of diabetes-related complications is highest. We found a one-year increase in average education for those with 12 or more years of education was associated with lower HbA1c, with larger point estimates for those in the high-risk tail of the HbA1c distribution. Our results add to understanding the education-HbA1c relationship and underscore the importance of evaluating the education-HbA1c relationship across the entire outcome distribution. Our results may also suggest an avenue for intervention: policies to increase education could reduce population-level diabetes complications, such as cardiovascular events and all-cause mortality.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Pinchevsky Y, Butkow N, Raal FJ, Chirwa T, Rothberg A. Demographic and Clinical Factors Associated with Development of Type 2 Diabetes: A Review of the Literature. International Journal of General Medicine [Internet]. 2020;13(1):121–9. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC 7127847/32280262 10.2147/IJGM.S 226010 PMC 7127847 · doi ↗ · pubmed ↗
- 2Mirzaei M, Rahmaninan M, Mirzaei M, Nadjarzadeh A, Dehghani tafti AA. Epidemiology of diabetes mellitus, pre-diabetes, undiagnosed and uncontrolled diabetes in Central Iran: results from Yazd health study. BMC Public Health. 2020 Feb 3;20(1).10.1186/s 12889-020-8267-y PMC 699815232013917 · doi ↗ · pubmed ↗
- 3Zeru MA, Tesfa E, Mitiku AA, Seyoum A, Bokoro TA. Prevalence and risk factors of type-2 diabetes mellitus in Ethiopia: systematic review and meta-analysis. Scientific Reports. 2021 Nov 5;11(1).10.1038/s 41598-021-01256-9PMC 857129734741064 · doi ↗ · pubmed ↗
- 4Nilsson PM, Johansson SE., Sundquist J. Low educational status is a risk factor for mortality among diabetic people. Diabetic Medicine. 2004 Jul 19;15(3):213–9.10.1002/(SICI)1096-9136(199803)15:3<213::AID-DIA 569>3.0.CO;2-#9545122 · doi ↗ · pubmed ↗
- 5Aamir AH, Ul-Haq Z, Mahar SA, Qureshi FM, Ahmad I, Jawa A, Diabetes Prevalence Survey of Pakistan (DPS-PAK): prevalence of type 2 diabetes mellitus and prediabetes using Hb A 1c: a population-based survey from Pakistan. BMJ Open [Internet]. 2019 Feb;9(2):1–9. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC 6398762/10.1136/bmjopen-2018-025300 PMC 639876230796126 · doi ↗ · pubmed ↗
- 6Östgren CJ, Sundström J, Svennblad B, Lohm L, Nilsson PM, Johansson G. Associations of Hb A 1c and educational level with risk of cardiovascular events in 32 871 drug-treated patients with Type 2 diabetes: a cohort study in primary care. Diabetic Medicine. 2013 Jan;30(5):170–7.23350893 10.1111/dme.12145 PMC 3654570 · doi ↗ · pubmed ↗
- 7Yahyavi SK, Snorgaard O, Knop FK, Schou M, Lee C, Selmer C, Prediabetes Defined by First Measured Hb A 1c Predicts Higher Cardiovascular Risk Compared With Hb A 1c in the Diabetes Range: A Cohort Study of Nationwide Registries. Diabetes Care [Internet]. 2021 Oct 21;44(12):2767–74. Available from: https://diabetesjournals.org/care/article/44/12/2767/138475/Prediabetes-Defined-by-First-Measured-Hb A 1c?searchresult=134675054 10.2337/dc 21-1062 · doi ↗ · pubmed ↗
- 8Kuo I-Ching, Lin HYH, Niu SW, Hwang DY, Lee JJ, Tsai JC, Glycated Hemoglobin and Outcomes in Patients with Advanced Diabetic Chronic Kidney Disease. Scientific Reports [Internet]. 2016 Jan 28;6(1). Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC 4730215/10.1038/srep 20028 PMC 473021526818011 · doi ↗ · pubmed ↗