Recurrent Pericarditis in a Woman With Acromegaly Responding Favorably to Transsphenoidal Surgery
Samantha Jacobson, Jonathan-Raphaël Stetco, Natasha Garfield

TL;DR
A woman with acromegaly experienced recurring pericarditis, which improved after surgery to remove her pituitary tumor.
Contribution
This case suggests a possible link between acromegaly and pericarditis, mediated by elevated IGF-1 levels.
Findings
Recurrent pericarditis resolved after transsphenoidal surgery normalized IGF-1 levels.
Elevated IGF-1 may mediate inflammatory processes in the pericardium in acromegaly.
Pericarditis did not recur during 12 years of acromegaly remission post-surgery.
Abstract
Acromegaly is associated with increased insulin-like growth factor 1 (IGF-1), promoting systemic inflammation and cardiovascular complications. We present a patient with acromegaly who developed recurrent pericarditis, resolving soon after somatotroph pituitary adenoma resection. The objective of this report is to describe a case of uncontrolled acromegaly with recurrent, unexplained pericarditis. A 46-year-old woman was referred after a neurologist identified a 9 mm pituitary lesion on magnetic resonance imaging. Laboratory tests showed elevated IGF-1 of 52.3 nmol/mL (12.3–32.9 nmol/L), a nonsuppressible growth hormone (GH) level of 3.8 mcg/L (<0.4 mcg/L) after a 75 g oral glucose tolerance test, confirming acromegaly. One-year postdiagnosis, the patient developed pleuritic chest pain from pericarditis with moderate-to-severe pericardial effusion. Symptoms resolved with nonsteroidal…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
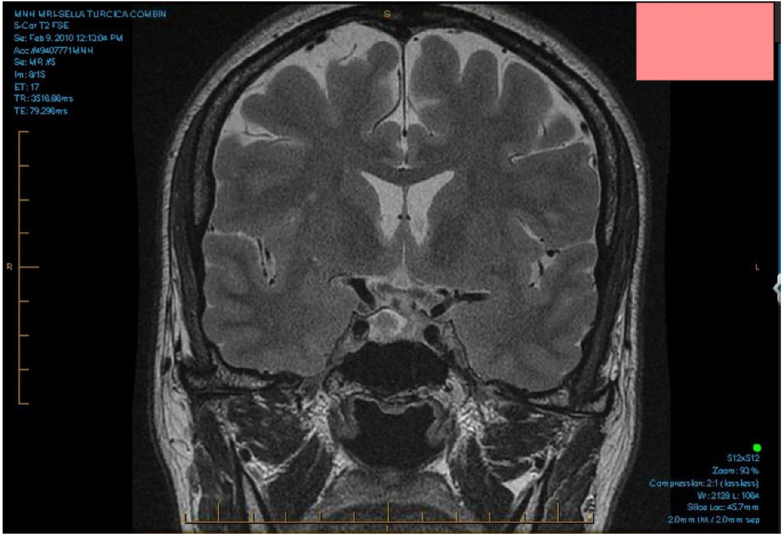 Figure 1
Figure 1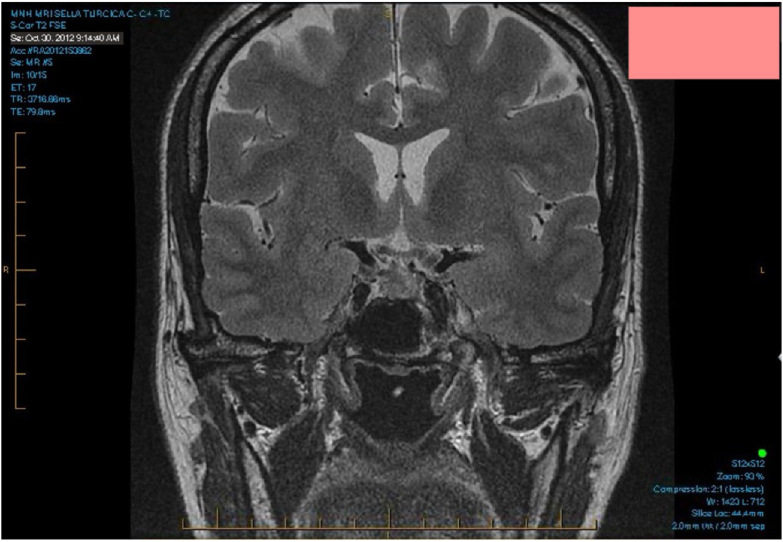 Figure 2
Figure 2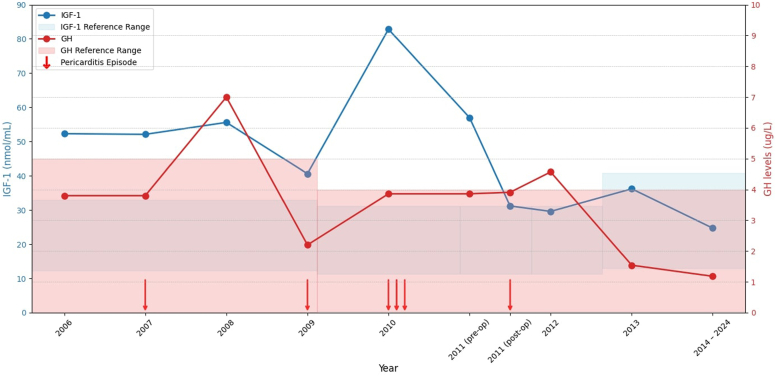 Figure 3
Figure 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsMyasthenia Gravis and Thymoma · Pericarditis and Cardiac Tamponade · Takotsubo Cardiomyopathy and Associated Phenomena
Highlights
- •Recognize pericarditis as a potential complication in acromegaly patients
- •Elevated IGF 1 levels may trigger inflammatory mechanisms leading to pericarditis
- •This case highlights the importance of looking and monitoring for cardiovascular health in acromegaly patients
Clinical RelevanceThis case highlights the importance of monitoring and managing cardiovascular complications in acromegaly, emphasizing the need for early intervention and hormone control to prevent serious conditions like recurrent pericarditis.
Introduction
Acromegaly is a rare endocrine disorder caused by excessive growth hormone (GH) secretion, with a prevalence ranging from 2.8 to 13.7 per 100 000 people.1 It typically results from a GH-secreting pituitary adenoma, leading to elevated insulin-like growth factor 1 (IGF-1) levels.2 Clinical manifestations include enlarged facial features, hands and feet, alongside systemic complications, including cardiovascular diseases like left ventricular hypertrophy and cardiomyopathy.2^,^3 Arterial hypertension and valvular heart disease are common, with electrocardiographic abnormalities frequently observed.3
Although cardiovascular complications are recognized in acromegaly, pericardial abnormalities are exceedingly rare. To date, only a single case of chronic pericardial effusion in a patient with active acromegaly has been reported, with elevated IGF-1 levels.4 The occurrence of recurrent pericarditis in patients with acromegaly has not been previously described in the literature.
Here, we describe a 46-year-old patient who experienced multiple episodes of pericarditis during hormonally active acromegaly. This case highlights the temporal association between active acromegaly, recurrent pericarditis, and resolution of episodes following definitive treatment and normalization of IGF-1 levels, suggesting a potential causal relationship.
Case Report
A 46-year-old woman was referred to our clinic after a neurologist, in the evaluation of headaches, identified a 9 mm lesion in the right hemianterior pituitary gland on brain magnetic resonance imaging (MRI). The patient complained of worsening headaches over several months, described as 'pressure-like pain'. Her medical history was positive for an oophorectomy for an ovarian cyst decades earlier, a history of cholelithiasis requiring cholecystectomy, and recurrent urinary tract infections. Her only chronic condition was thalassemia minor. She was not taking any medications other than over-the-counter analgesics for headaches and reported no prior cardiovascular disease. On physical examination, her visual fields were intact to confrontation. She was noted to have an enlarged nose and increase nasolabial folds. Her blood pressure was 110/65 mmHg and no signs of cardiac murmurs, joint swelling, prognathism, enlarged tongue, hoarse voice, or enlarged hands and feet. Laboratory testing revealed IGF-1 of 52.3 nmol/mL (12.3–32.9 nmol/mL) and a nonsuppressible GH of 3.8 mcg/L, following a 75 g oral glucose tolerance test (<0.4 mcg/L). Prolactin (16.8 ug/L; reference range of 3.3-26.7 ug/L), AM cortisol (301 nmol/L; reference range of 120-535 nmol/L), adrenocorticotropic hormone (7 pmol/L; reference range of ≤ 10 pmol/L), thyroid-stimulating hormone (1.35 mIU/L; reference range of 0.4-4.40 mIU/L), free T3 (3.9 pmol/L; reference range of 3.5-5.7 pmol/L), luteinizing hormone (2.6 IUslLiter), follicle-stimulating hormone (7.7 IUslLiter), and estradiol (174 pmol/L) were within normal limits.
The patient was diagnosed with acromegaly, and somatostatin analog therapy was initiated with octreotide, which initially decreased her IGF-1 to 35.1 nmol/L (12.3–32.9 nmol/mL). On follow-up 8 months later, her IGF-1 subsequently rose to 52.1 nmol/L (12.3–32.9 nmol/mL), prompting a switch to lanreotide.
Approximately 1 year after diagnosis, the patient developed pleuritic chest pain. Electrocardiogram revealed diffuse ST elevations with T wave inversions and transthoracic echocardiogram showed moderate-to-severe pericardial effusion secondary to pericarditis with no structural heart anomaly. No etiological workup was done. Pericardiocentesis was performed and she was treated with nonsteroidal antiinflammatory drugs (NSAIDs), colchicine, leading to symptom resolution. Two years later, she had a second episode of pericarditis. She was treated again with NSAIDs and colchicine, which resulted in symptom resolution. Her IGF-1 level was 40.6 nmol/mL on lanreotide (12.3–32.9 nmol/mL). Over the next year, the patient experienced three additional episodes of pericarditis. Each episode was managed with a combination of naproxen, colchicine, and prednisone. During one episode, she developed a pericardial effusion, which required pericardiocentesis. Echocardiography revealed a left ventricular ejection fraction of 57%. Tests including ANA, anti-SSA, anti-dsDNA, c-ANCA, p-ANCA, C3, C4, and ACE levels, were noncontributory. Tests for syphilis, tuberculosis, and HIV, were negative. Laboratory results showed elevated C reactive protein at 150 mg/L (reference range of 0–5 mg/L) and microcytic anemia (hemoglobin: 102 g/L; reference range of 120–160 g/L, mean cell volume: 65.2 fL; reference range of 82.0–100.0 fL). Her liver function tests (bilirubin total: 18.0 μmol/L; reference range of 1.7–18.9 μmol/L, alanine aminotransferase: 16 U/L; reference range of 6–45 U/L, alkaline phosphatase: 71 U/L; reference range of 42–98 U/L), renal function (creatinine 50 umol/L; reference range of 40-85 umol/L), thyroid-stimulating hormone (0.92 mIU/L; reference range of 0.4-4.40 mIU/L), troponin-I (0.05 ug/L; reference range of 0.00-0.06 ug/L), and creatine kinase (61 U/L (reference range of 5-140 U/L) were all within normal limits. She exhibited no symptoms of arthritis, uveitis, or cutaneous manifestations of vasculitis. Her IGF-1 level at that time was elevated at 82.8 nmol/mL (11.4–31.1 nmol/mL). The patient was thus referred to neurosurgery for pituitary lesion removal.
Preoperative brain MRI revealed a 1.8 cm lesion in the right hemianterior pituitary gland, compatible with a pituitary adenoma (Fig. 1). Nine months following her previous pericardial episode, she underwent a transsphenoidal resection of the pituitary adenoma. Histopathology of the resected adenoma confirmed a somatotroph pituitary adenoma. Postoperatively, her IGF-1 dropped to 31.2 nmol/mL (11.4–31.1 nmol/mL), and she stopped all her medications, including lanreotide, colchicine, and naproxen.Fig. 1. Preoperative brain magnetic resonance imaging (MRI); Showing a 1.8 cm pituitary adenoma in right hemianterior pituitary gland.
Two months after surgery, despite an improvement in IGF-1 at 29.6 nmol/mL (11.4–31.1 nmol/mL) and GH to 0.32 mcg/L (0.03–4.00 mcg/L), the patient experienced a final episode of pericarditis. This episode was treated with NSAIDs and colchicine, leading to full resolution. One-year postoperative brain MRI findings were compatible with resection of right-sided pituitary adenoma, with no evidence of recurrence of the lesion previously operated (Fig. 2).Fig. 2. Brain magnetic resonance imaging (MRI) post-transsphenoidal pituitary adenoma resection; Showing no evidence of recurrence of the pituitary adenoma.
Since her pituitary surgery, the patient has been followed-up for a period of 12 years. During this time, the patient has not experienced any recurrent episodes of pericarditis. Her acromegaly remains in remission with an IGF-1 of 10.7 nmol/L (7.3–22.1 nmol/L). No adjuvant therapy was required. There were no other complications of acromegaly including hypertension, colonic polyps, diabetes, change in ring and shoe size, or arthralgias. As of her most recent visit in 2024, she has continued to report no symptoms of recurrence, including chest pain or headaches. Fig. 3 summarizes the trends in IGF-1 and GH levels over time and their association with her acute pericarditis episodes.Fig. 3. Trends of IGF-1 and GH levels with pericarditis episodes (2006-2024), with reference ranges highlighted. Red arrows indicate the timing of pericarditis episodes. GH = growth hormone; IGF-1 = insulin-like growth factor 1.
Discussion
We present a case describing a 46-year-old woman with acromegaly who experienced six episodes of pericarditis over several years. The majority of these episodes occurred while her acromegaly was active. Acromegaly is characterized by excessive secretion of GH and IGF-1, leading to systemic complications, including cardiovascular abnormalities. Common manifestations include left ventricular hypertrophy which can lead to heart failure and cardiomyopathy3 and arterial hypertension which is an independent risk factor for mortality in acromegaly.3 Valvular heart disease often involves the aortic and mitral valves and can persist even after treatment.3 Pericarditis, to our knowledge, has not been described in the literature as a feature of acromegaly, although a case of chronic pericardial effusion in a 73-year-old woman with active acromegaly has been documented.4 The authors of that report suggested that the effusion was likely linked to pericardial disturbances associated with elevated GH and IGF-1 levels.4 In our case, the recurrent nature of the pericarditis and its resolution with IGF-1 normalization further support a possible causal relationship. The pathophysiology of pericarditis in acromegaly may involve inflammatory and immunologic mechanisms influenced by elevated GH and IGF-1 levels.5^,^6
The episodic flares of pericarditis appeared to correlate with increased IGF-1 levels. To note, IGF-1 was only measured during endocrinology follow-ups, which occurred after her initial cardiology hospitalizations for pericarditis. As shown in Fig. 3, her highest IGF-1 level (82.8 nmol/L) coincided with her most severe episodes of pericarditis. This temporal relationship underscores the potential influence of active acromegaly on her condition. IGF-1 has been shown to potentiate the production of pro-inflammatory cytokines (interleukin 6, tumor necrosis factor alpha, and interferon-γ) in response to toll-like receptor ligands.6 These proinflammatory cytokines play critical roles in inflammatory diseases.7 Therefore, elevated IGF-1 could upregulate systemic inflammation, potentially triggering or exacerbating episodes of pericarditis.
Most common causes of pericarditis, including autoimmune disorders or infections,8 were ruled out in this patient. Additionally, she did not take medications known to cause drug-induced pericarditis, such as procainamide, hydralazine, methyldopa, isoniazid, or phenytoin.8 The absence of alternative etiologies strengthens the plausibility of this association. The final episode occurred postoperatively, despite a normal IGF-1 (29.6 nmol/mL), and resolved with reinitiation of colchicine and NSAIDs. This episode followed the abrupt discontinuation of anti-inflammatory therapy, a known risk factor for pericarditis recurrence.9 Recurrent pericarditis develops in 15% to 30% of cases.10 Risk factors for recurrence include early corticosteroid use, lack of response to NSAIDs, and elevated C reactive protein levels.11
At the time of her diagnosis of acromegaly, medical management was the preferred alternative to surgical treatment.12 Therefore, a decision was made to treat her medically to shrink the tumor, with the goal of making surgery a viable curative option in the future. As such, she was initially treated with octreotide LAR, which was discontinued and switched to lanreotide after her IGF-1 levels failed to decrease adequately.
While this case adds to the limited understanding of cardiac complications in acromegaly, it is observational and lacks mechanistic validation. Future research should explore the underlying mechanisms linking acromegaly and recurrent pericarditis, as well as the role of medical therapy in preventing recurrence.
Disclosure
The authors have no conflicts of interest to disclose.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Lavrentaki A.Paluzzi A.Wass J.A.H.Karavitaki N.Epidemiology of acromegaly: review of population studies Pituitary 20120174910.1007/s 11102-016-0754-x 27743174 PMC 5334410 · doi ↗ · pubmed ↗
- 2Ershadinia N.Tritos N.A.Diagnosis and treatment of acromegaly: an update Mayo Clin Proc 972202233334610.1016/j.mayocp.2021.11.00735120696 · doi ↗ · pubmed ↗
- 3Sharma M.D.Nguyen A.V.Brown S.Robbins R.J.Cardiovascular disease in acromegaly Methodist De Bakey Cardiovasc J 1322017646710.14797/mdcj-13-2-6428740584 PMC 5512681 · doi ↗ · pubmed ↗
- 4Alter P.Rominger M.B.Kajdan U.Pericardial effusion and non-constrictive diastolic dysfunction in acromegaly Eur J Radiol Extra 5832006818410.1016/j.ejrex.2006.03.007 · doi ↗
- 5Witkowska-Sędek E.Pyrżak B.Chronic inflammation and the growth hormone/insulin-like growth factor-1 axis Cent Eur J Immunol 454202046947510.5114/ceji.2020.10342233613096 PMC 7882400 · doi ↗ · pubmed ↗
- 6Wolters T.L.C.Netea M.G.Hermus A.R.M.M.Smit J.W.A.Netea-Maier R.T.IGF 1 potentiates the pro-inflammatory response in human peripheral blood mononuclear cells via MAPKJ Mol Endocrinol 592201712913910.1530/JME-17-006228611056 · doi ↗ · pubmed ↗
- 7Kany S.Vollrath J.T.Relja B.Cytokines in inflammatory disease Int J Mol Sci 20232019600810.3390/ijms 2023600831795299 PMC 6929211 · doi ↗ · pubmed ↗
- 8Lilly L.S.Pathophysiology of Heart Disease: An Introduction to Cardiovascular Medicine, 7e 2021 Lippincott Williams & Wilkins, a Wolters Kluwer business