A Case Report of a Boy With Clinically Mild Encephalopathy and a Reversible Splenial Lesion Associated With Severe Acute Respiratory Syndrome-Coronavirus 2 Infection
Yuko Moriuchi, Tatsuo Fuchigami, Ichiro Morioka

TL;DR
A 9-year-old boy with mild encephalopathy and a reversible brain lesion due to SARS-CoV-2 infection is reported, highlighting the importance of MRI in early diagnosis.
Contribution
This case report adds to the understanding of SARS-CoV-2-related neurological manifestations in children.
Findings
The patient showed transient high signal intensity in the splenium of the corpus callosum on MRI.
The patient was diagnosed with mild encephalopathy and recovered without neurological sequelae.
MRI is recommended for children with SARS-CoV-2 and neurological symptoms to detect early encephalopathy.
Abstract
Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection is associated with a high frequency of central nervous system abnormalities, particularly acute encephalopathy, in children. We report the case of a nine-year-old boy with SARS-CoV-2-associated clinically mild encephalopathy with a reversible splenial lesion. The patient was admitted to our hospital with fever, vomiting, and poor speech. The patient tested positive for SARS-CoV-2 by polymerase chain reaction of a nasal swab sample. The cerebrospinal fluid cell count was normal. The patient had a low serum sodium level upon admission. Computed tomography of the brain revealed mild cerebral edema. Diffusion-weighted magnetic resonance imaging (MRI) revealed transient abnormally high signal intensity in the splenium of the corpus callosum. Electroencephalography revealed generalized high-voltage slow waves. The patient…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
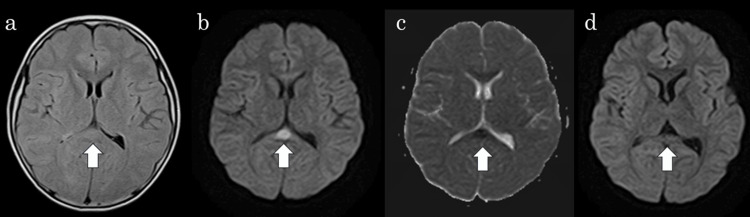 Figure 1
Figure 1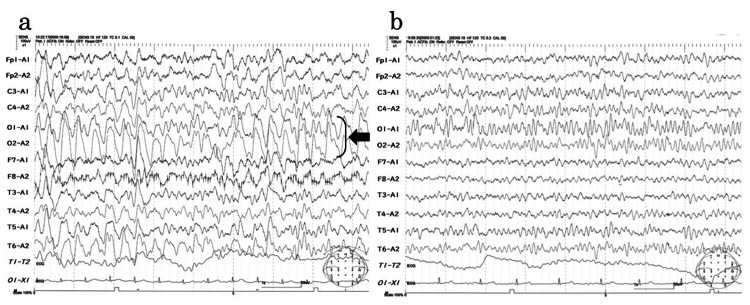 Figure 2
Figure 2| Laboratory blood findings | Our patient’s results | Reference range |
| Leukocyte cell (/µL) | 6,300 | 3,300–8,600 |
| Platelet (/µL) | 199,000 | 158,000–348,000 |
| C-reactive protein (mg/dL) | 2.08 | 0.01–0.14 |
| Sodium (mEq/L) | 133 | 136–147 |
| Potassium (mEq/L) | 4.3 | 3.5–5.0 |
| Chloride (mEq/L) | 96 | 98–108 |
| Urea nitrogen (mg/dL) | 20.8 | 8.0–23.0 |
| Creatinine (mg/dL) | 0.71 | 0.61–1.08 |
| Aspartate aminotransferase (IU/L) | 51 | 8–40 |
| Alanine aminotransferase (IU/L) | 31 | 5–45 |
| Lactate dehydrogenase (IU/L) | 260 | 124–222 |
| Creatinine kinase (IU/L) | 91 | 55–250 |
| Glucose (mg/dL) | 71 | 70–109 |
| Ammonia (µg/dL) | 25 | 55–250 |
| Cerebral spinal fluid results | ||
| Leukocyte cell (/µL) | 5 | 0–5 |
| Protein (mg/dL) | 32.1 | 10–40 |
| Glucose (mg/dL) | 53 | 50–75 |
| Patient number | Reference | Age (years) | Sex | Neurological symptoms | Serum sodium (mEq/l) | Day of the first MRI (since the first neurological symptoms) | Day of follow-up MRI (since the first neurological symptoms) | Diagnosis | Outcome |
| 1 | Abdel-Mannan et al. [ | 15 | F | Confused, disoriented, headache, weakness | Normal | 5 days | NR | MIS-C | Recovering |
| 2 | Abdel-Mannan et al. [ | 15 | F | Confused, dysarthria, dysphagia | Normal | 21 days | NR | MIS-C | Day 32: still inpatient; encephalopathy resolved, wheelchair bound |
| 3 | Abdel-Mannan et al. [ | 9 | M | Confused, ataxia, dysarthria, headache | 129 | 1 day | 6 days (with minimal signal changes remaining on T2) | MIS-C | Recovering |
| 4 | Varol et al. [ | 15 | M | Headache, dizziness, blurred vision, agitation, vomiting | 128 | 5 days | 15days (disappeared) | MIS-C | Recovering |
| 5 | Varol et al. [ | 14 | M | Ataxia, hallucinations | 135 | 3 days | 10days (disappeared) | MIS-C | Recovering |
| 6 | Bektaş et al. [ | 11 | F | Personality changes | 132 | 6 days | 7 days (disappeared) | MIS-C | Recovering |
| 7 | Bektaş et al. [ | 10 | M | Agitation, disorient, hallucinations | 131 | 2 days | 7 days (disappeared) | MIS-C | Recovering |
| 8 | Gaur et al. [ | 12 | M | Lethargy, headache, vomiting | NR | 5 days | Not performed | MIS-C | Recovering |
| 9 | Gaur et al. [ | 9 | M | Altered mental state, lethargy, dysarthric, ataxic | NR | NR | NR (disappeared) | COVID-19 | Recovering |
| 10 | PR | 9 | M | Vomiting, poor speech | 133 | 2 days | 9 days (disappeared) | COVID-19 | Recovering |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsInfectious Encephalopathies and Encephalitis · Long-Term Effects of COVID-19 · Multiple Sclerosis Research Studies
Introduction
Coronavirus disease 2019 (COVID-19), caused by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), primarily produces respiratory symptoms. However, since the sixth wave, when the Omicron strain became the mainstream of the epidemic, higher frequencies of central nervous system abnormalities, especially acute encephalopathy due to pediatric COVID-19, have been reported [1,2]. Tada et al. [3] identified clinically mild encephalitis/encephalopathy with a reversible splenial lesion (MERS). It was characterized by transient splenial lesions with high signal intensity on diffusion-weighted magnetic resonance imaging (MRI), a mild clinical course, and a good outcome as a new type of acute encephalopathy [3]. A reversible splenial lesion in the corpus callosum with homogenous reduced diffusion may be detected in various conditions such as infection, withdrawal of antiepileptic drugs, altitude sickness, Kawasaki disease, electrolyte abnormalities (especially hyponatremia), hypoglycemia, and X-linked Charcot-Marie-Tooth disease. In particular, encephalitis and encephalopathy with mild neurological symptoms and good prognosis have been reported as MERS [4].
The most common MERS pathogen is the influenza virus (22%), followed by rotavirus (9%) and human herpesviruses 6 and 7 (5%) [5]. However, few reported cases of MERS have been associated with SARS-CoV-2 infection in children [6-9].
Here, we report the case of a nine-year-old boy with MERS associated with SARS-CoV-2 infection.
Case presentation
A previously healthy nine-year-old boy presented to another clinic with a fever, followed by vomiting and appetite loss, and the patient was then admitted to our hospital on the same day. He had no history of seizures and his development was normal.
On the day of admission, the patient had a fever of 39.1 ℃. His blood pressure was 103/57 mmHg, his pulse rate was 123 beats/min, and his oxygen saturation was 99% from room air. His general health status was somewhat poor. The patient’s speech was affected, and his consciousness was 13 points on the Glasgow Coma Scale (GCS) of E4 V3 M6. Neurological examination revealed no abnormalities, except for his poor speech. No neck stiffness was observed. The chest and abdomen exhibited no abnormalities. The patient had no cough, respiratory problems, or abnormal findings on the chest radiograph. The capillary refilling time was elevated (3 s).
Initial laboratory blood findings revealed normal leukocyte and platelet counts and elevated C-reactive protein at 2.08 mg/dL. The serum electrolytes were low sodium at 133 mEq/L and low chloride at 96 mEq/L. Blood urea nitrogen was elevated at 20.8 mg/dL, aspartate aminotransferase at 51 IU/L, and lactate dehydrogenase at 260 IU/L (Table 1).
The patient had no history of SARS-CoV-2 infection and had not been vaccinated against SARS-CoV-2. Approximately two weeks prior, his mother had tested positive for SARS-CoV-2 by polymerase chain reaction (PCR) of a nasal swab sample.
The patient tested positive for SARS-CoV-2 by PCR of a nasal swab sample. Cerebral spinal fluid examination showed no abnormality. Brain computed tomography (CT) revealed mild edema. A brain MRI was performed on the second day of admission because of persistent poor speech. Abnormal signals were observed, however, in the splenium of the corpus callosum (SCC), which revealed a somewhat high intensity on fluid-attenuated inversion recovery imaging (Figure 1a), hyperintensity on diffusion-weighted imaging (DWI) (Figure 1b), and apparent diffusion coefficient (ADC) mapping showed decreased ADC values at the abnormality (17.2 mm^2^/s) (Figure 1c).
Brain MRIInitial MRI revealed abnormal signals in the splenium of the corpus callosum (arrow), which were of somewhat hyperintensity on fluid-attenuated inversion recovery imaging (a), hyperintensity on diffusion-weighted imaging (DWI) (b), and hypointensity on apparent diffusion coefficient (ADC) mapping (c). Follow-up MRI showing complete improvement of the SCC on DWI (arrow) (d).SCC: Splenium of the corpus callosum
Magnetic resonance angiography did not reveal any cerebral vascular stenosis or aneurysms. Electroencephalography (EEG) on the second day of admission revealed diffuse high-voltage slow waves during awake recordings (Figure 2a).
EEGa. Awake patient (second day of admission) exhibited diffused high-voltage slow waves of approximately 2–3 Hz in the particularly marked occipital area (arrow). Calibration: 100 µV, 1 sb. The patient was awake (ninth day of admission) and provided almost normal findings, with no slow waves. The background rhythm was 9–10 Hz, there was no laterality, and the normal spindle and hump were shown. Calibration: 100 µV, 1 s
These findings strongly suggest that acute encephalopathy is associated with SARS-CoV-2 infection. The patient was administered intravenous osmotic diuretic and edaravone. He could state his name and age on the third day of admission, speak spontaneously on the fourth day, and respond to questions on the fifth; therefore, methylprednisolone pulse therapy was not started. On the eighth day after admission, follow-up MRI revealed complete improvement in the SCC signal changes (Figure 1d). The EEG on the same day was almost normal. No slow waves or seizures were observed (Figure 2b). The final diagnosis was MERS associated with SARS-CoV-2 infection. On the 11th day of admission, the patient was discharged without any neurological sequelae. The patient’s development and intelligence have remained unchanged since discharge.
Discussion
During national surveillance from 2014 to 2017 (during the previous SARS-CoV-2 infection outbreak) in Japan, 1115 acute encephalopathies associated with infectious diseases occurred in Japanese children and were most common in infants aged 0-3 [10]. These have been classified into several clinic-radiological syndromes, such as acute encephalopathy with biphasic seizures and late reduced diffusion, which is the most common subtype (34.0%), followed by clinically mild encephalitis/encephalopathy with a reversible splenial lesion (MERS) (19.3%) and acute necrotizing encephalopathy (2.8%) [10]. However, in a nationwide epidemiological study during the SARS-CoV-2 infection outbreak in Japan, MERS accounted for 8.7% of the encephalopathy syndromes due to SARS-CoV-2, which is lower than the 19.3% of non-SARS-CoV-2-associated encephalopathies [11]. Patients with MERS typically exhibit symptoms associated with the central nervous system, including delirious behavior, consciousness disturbances, and seizures, with complete recovery within a month [5]. It has been speculated that the low number of SARS-CoV-2-associated MERS cases may be due to the difficulty in obtaining MRI scans in COVID-19 patients due to isolation after hospitalization, which may result in transient lesions in the splenium being missed, which are essential for the diagnosis of MERS [3,11]. In addition, the mean age of patients with MERS in conventional viral encephalopathy is 5.6 years [10], whereas the patients in this study were relatively older at nine years of age. Table 2 summarizes the 10 cases of MERS associated with SARS-CoV-2 infection in children that have been reported [6-9].
All of these patients were older than nine years of age. Therefore, even in older children, MERS should be considered when SARS-CoV-2 infection is present. In the present case, encephalopathy was suspected because of poor speech. MRI performed on the second day of admission led to a diagnosis of MERS. In addition, follow-up MRI performed one week after admission confirmed the disappearance of high-signal areas in the corpus callosum, confirming the efficacy of the treatment. Thus, MRI is useful for diagnosing encephalopathy and determining the effectiveness of treatment. DWI is a key imaging modality used to diagnose MERS. It reveals homogeneously reduced diffusion in the corpus callosum without contrast enhancement [5]. Therefore, MRI should be considered when encephalopathy is suspected.
Transient signal changes in the splenium of the corpus callosum on MRI have been reported in various neurological and non-neurological disorders. Based on signal changes, the splenium is involved in two types according to its shape and extent: oval, circumscribed, with well‑defined borders usually located in the middle, or broader, with less regular borders and involving the entire splenium ("boomerang sign") [12].
MERS is caused by intramyelinic axonal edema or local inflammatory cell infiltration [3]. Takanashi et al. [13] have reported that most patients with MERS have mild hyponatremia. Hypotonic hyponatremia causes fluid accumulation in the brain, leading to cerebral edema, headache, nausea, vomiting, confusion, and seizures. It is clinically challenging to distinguish MERS from hyponatremic encephalopathy or to exclude hyponatremia as a causative factor of MERS [13]. Our previous reports revealed that MERS is not specifically associated with hyponatremia [14-16]. Previous SARS-CoV-2-associated MERS reports, summarized in Table 2, have also reported low to normal serum sodium levels. These findings indicate that SARS-CoV-2-associated MERS can develop without hyponatremia.
In adults, SARS-CoV-2 mainly causes respiratory infections but may also be accompanied by neurological symptoms and complications such as cerebral infarction, encephalitis, and encephalopathy have also been reported [17]. In recent years, acute encephalopathy caused by SARS-CoV-2 infection in Japanese children appeared as a primary neurological symptom before respiratory symptoms [18]. No respiratory symptoms were observed in this case, and obvious respiratory symptoms have accompanied no previous MERS cases. Thus, the mechanism of development of central nervous symptoms associated with SARS-CoV-2 infection is speculated to differ between adults and children.
In this case, neurological symptoms and MRI findings improved with the administration of mannitol and edaravone alone. However, except for the present case and patient 9 in Table 2, the other patients developed pediatric multisystem inflammatory syndrome and required methylprednisolone pulse therapy and intravenous immunoglobulin therapy. Furthermore, as for patient 2, the clinical symptoms can persist even in patients with MERS. Thus, although MERS is generally considered to have a good prognosis, careful follow-up is required.
Conclusions
Performing an MRI evaluation is useful in children with SARS-CoV-2 infection in conjunction with impaired consciousness, poor speech, and behavior, given the possibility that they may be in the early stages of encephalopathy. DWI is an important imaging modality for diagnosing MERS, and performing MRI is recommended to detect reversible lesions in the corpus callosum. MRI is not only useful for diagnosing encephalopathy but also for assessing the effectiveness of treatment.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1COVID-19 and acute neurologic complications in children Pediatrics Antoon JW Hall M Howard LM Herndon A Freundlich KL Grijalva CG Williams DJ 150202210.1542/peds.2022-058167 PMC 963338335949041 · doi ↗ · pubmed ↗
- 2Global incidence of neurological manifestations among patients hospitalized with COVID-19-a report for the GCS-Neuro COVID consortium and the ENERGY consortium JAMA Netw Open Chou SH Beghi E Helbok R 04202110.1001/jamanetworkopen.2021.12131 PMC 811414333974053 · doi ↗ · pubmed ↗
- 3Clinically mild encephalitis/encephalopathy with a reversible splenial lesion Neurology Tada H Takanashi J Barkovich AJ 185418586320041555750110.1212/01.wnl.0000144274.12174.cb · doi ↗ · pubmed ↗
- 4Guidelines for the diagnosis and treatment of acute encephalopathy in childhood Brain Dev Mizuguchi M Ichiyama T Imataka G 2314320213282997210.1016/j.braindev.2020.08.001 · doi ↗ · pubmed ↗
- 5Neuroimaging in acute infection-triggered encephalopathy syndromes Front Neurosci Takanashi JI Uetani H 12353641720233763832010.3389/fnins.2023.1235364 PMC 10447893 · doi ↗ · pubmed ↗
- 6Neurologic and radiographic findings associated with COVID-19 infection in children JAMA Neurol Abdel-Mannan O Eyre M Löbel U 144014457720203260933610.1001/jamaneurol.2020.2687 PMC 7330822 · doi ↗ · pubmed ↗
- 7Can plasma exchange therapy be an option for the treatment of SARS-Co V-2 Related Splenial Lesion Syndrome: two cases from the pediatric intensive care unit Transfus Apher Sci Varol F Ergul N Sahin EG Can YY Ergul U Guven S Cam H 1034916120223571076510.1016/j.transci.2022.103491 PMC 9187863 · doi ↗ · pubmed ↗
- 8Reversible splenial lesion syndrome associated with SARS-Co V-2 infection in two children Brain Dev BektaşG Akçay N BoydağK Şevketoğlu E 2302334320213308205910.1016/j.braindev.2020.10.002PMC 7553133 · doi ↗ · pubmed ↗