Deep learning signature to predict postoperative anxiety in patients receiving lung cancer surgery
Qingqing Ji, Guohua Zhou, Xiangxiang Sun

TL;DR
This study developed a deep learning model using MRI images to predict postoperative anxiety in lung cancer surgery patients.
Contribution
A novel deep learning signature based on MRI and ResNet-152 to predict postoperative anxiety in lung cancer patients.
Findings
Larger tumor size and lymph node metastasis were independent predictors of postoperative anxiety.
The deep learning model achieved an area under the curve of 0.865 for predicting postoperative anxiety.
Higher deep learning scores correlated with increased risk of postoperative anxiety.
Abstract
This study aims on establishing and validate a deep learning signature based on magnetic resonance imaging (MRI) to predict postoperative anxiety in patients receiving lung cancer surgery. In the current study, 202 patients receiving lung cancer surgery were included. Preoperative MRI-T1WI images were collected to train the deep learning signature utilized the ResNet-152 algorithm. The relationships between clinical variables and postoperative anxiety were explored via Logistic regression and the predictive performances of the developed deep learning signature were evaluated via receiver operating characteristic analysis. Larger tumor size [odds ratio (OR), 2.044; 95% confidence interval (CI), 1.736–3.276; p = 0.002] and occurrence of lymph node metastasis (OR, 2.078; 95% CI, 1.023–3.221; p = 0.043) were revealed as independent predictors for postoperative anxiety. With the increase of…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
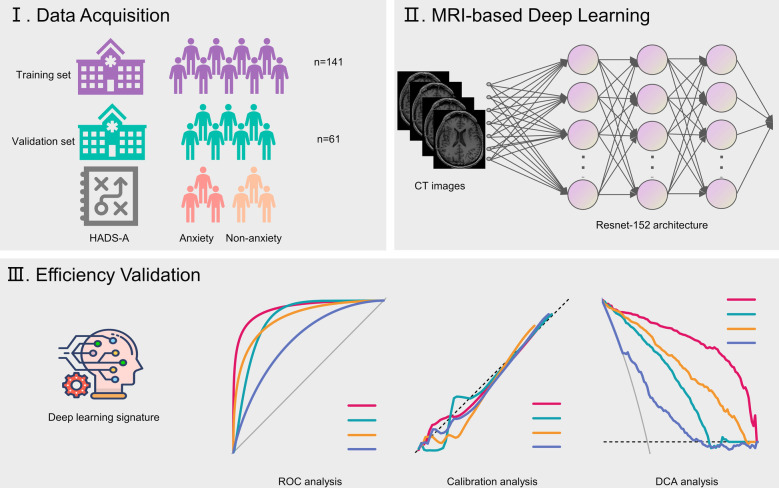 Figure 1
Figure 1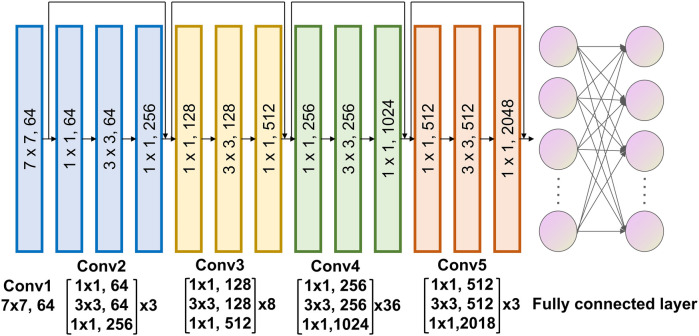 Figure 2
Figure 2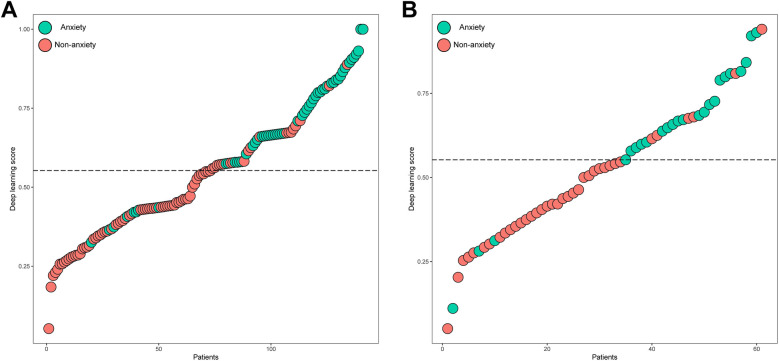 Figure 3
Figure 3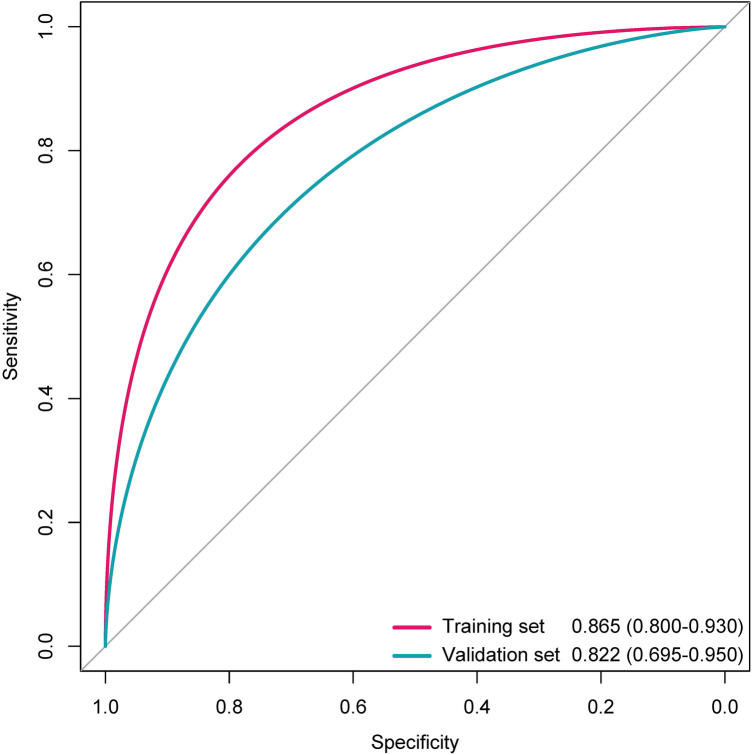 Figure 4
Figure 4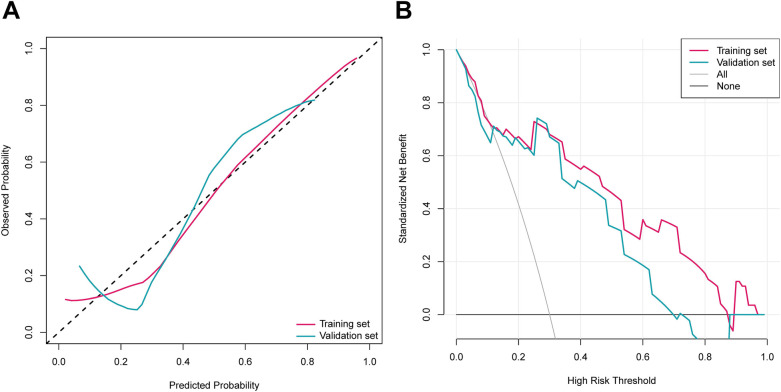 Figure 5
Figure 5| Characteristics | Entire cohort ( | Training ( | Validation ( | |
|---|---|---|---|---|
| Age (years), mean ± SD | 59.1 ± 11.0 | 58.9 ± 11.8 | 59.6 ± 9.2 | 0.696 |
| Sex, | 0.298 | |||
| Male | 94 (46.5) | 69 (48.9) | 25 (41.0) | |
| Female | 108 (53.5) | 72 (51.1) | 36 (59.0) | |
| Smoking, | 1.000 | |||
| Ever | 30 (14.8) | 21 (14.9) | 9 (14.7) | |
| Never | 172 (85.2) | 120 (85.1) | 52 (85.3) | |
| Histology, | 0.395 | |||
| Squamous cell carcinoma | 24 (11.6) | 19 (13.5) | 5 (8.2) | |
| Adenocarcinoma | 164 (81.2) | 111 (78.7) | 53 (86.9) | |
| Others | 14 (6.9) | 11 (7.8) | 3 (4.9) | |
| Location, | 0.147 | |||
| Left | 85 (42.1) | 61 (45.4) | 21 (34.4) | |
| Right | 117 (57.9) | 77 (54.6) | 40 (65.6) | |
| Tumor size, mean ± SD | 1.8 ± 0.7 | 1.8 ± 0.7 | 1.9 ± 0.7 | 0.293 |
| Lymph node metastasis, | 0.867 | |||
| No | 180 (89.1) | 125 (88.7) | 55 (90.2) | |
| Yes | 22 (10.9) | 16 (11.3) | 6 (9.8) | |
| Anxiety assessed by HADS-A, | 0.960 | |||
| Yes | 80 (39.6) | 56 (39.7) | 24 (39.3) | |
| No | 122 (60.4) | 85 (60.3) | 37 (60.7) | |
| Surgical approach, | 0.865 | |||
| Thoracoscopic | 196 (97.0) | 137 (97.2) | 59 (96.7) | |
| Thoracotomy | 6 (3.0) | 4 (2.8) | 2 (3.3) | |
| Variables | Anxiety | |||
|---|---|---|---|---|
| Univariable | Multivariable | |||
| OR (95% CI) | OR (95% CI) | |||
| Age | 0.994 (0.969–1.020) | 0.625 | ||
| Sex (Male) | 1.108 (0.629–1.951) | 0.723 | ||
| Smoking history (Ever) | 0.813 (0.367–1.803) | 0.611 | ||
| Histology (Adenocarcinoma) | 0.539 (0.141–2.033) | 0.359 | ||
| Location (Left) | 1.058 (0.597–1.874) | 0.847 | ||
| Tumor size | 2.334 (1.546–3.479) | 0.003 | 2.044 (1.734–3.276) | 0.002 |
| Lymph node metastasis (Yes) | 1.999 (1.133–3.528) | 0.017 | 2.078 (1.023–3.221) | 0.043 |
| Surgical approach (Thoracoscopic) | 0.943 (0.903–1.102) | 0.878 | ||
| Data set | Sensitivity | Specificity | PPV | NPV | Accuracy |
|---|---|---|---|---|---|
| Training set | 82.1% | 85.6% | 79.3% | 88.0% | 84.4% |
| Validation set | 83.3% | 83.8% | 76.9% | 88.6% | 83.6% |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsRadiomics and Machine Learning in Medical Imaging · Lung Cancer Diagnosis and Treatment · Cancer survivorship and care
Introduction
Globally, lung cancer ranks among the most common solid tumors and is a leading cause of cancer mortality. Its development is strongly associated with various risk factors, such as tobacco use, chronic obstructive pulmonary disease, and genetic predisposition (1–3). While advancements in radiotherapy, targeted treatments, and immunotherapy have partially enhanced clinical outcomes for lung cancer patients (4–6), mental health challenges remain a significant concern, adversely impacting their quality of life and survival rates (7, 8). Consequently, investigating the psychological issues faced by these patients is essential for optimizing their care.
Anxiety is a widespread mental health condition that negatively influence lung cancer patient outcomes. These disorders affect between 20.9% and 57.1% of individuals with lung cancer (9–11) and have been identified as indicators of poorer survival (12). Research indicates that post-surgical lung cancer patients experience anxiety influenced by factors like gender, marital status, complications, and aggressive tumor characteristics, all of which correlate with worse prognoses. Hence, precise recognition of patients who have the risk to experience anxiety after surgery is crucial for personalized management of lung cancer.
Deep learning-based radiomics, which extracts detailed features from medical images, offers a promising tool for tumor diagnosis, prognosis, and treatment planning (13–16). We hypothesized that the deep learning technique could capture features associated with postoperative anxiety from medical imaging, and further quantify the risks of postoperative anxiety to optimize the management of lung cancer. Therefore, this study purposes to develop and validate an imaging signature to predict anxiety based on the deep learning algorithm in patients after lung cancer surgery.
Materials and methods
Study population and data collection
The study obtained approval from the institutional review boards and ethics committees at Ningbox First Hospital. Patients undergoing lung cancer surgery between January 2024 and December 2024 were consecutively recruited. Clinicopathological information was extracted from electronic medical records. Anxiety was evaluated 3 days post-surgery using the Hospital Anxiety and Depression Scale-Anxiety (HADS-A), where scores range from 0 to 21, and a score ≥ 8 signifies anxiety (17). Preoperative brain magnetic resonance imaging (MRI) scans, conducted within 1 week before surgery, were obtained from the picture archiving and communication system. The study's design is depicted in Figure 1.
Flow chart illustrating study design. HADS-A, Hospital Anxiety and Depression Scale-Anxiety.
Deep learning procedures
All MRI-T1WI scans were download as DCM format. The personal information of patients in MRI images including name, medical number and hospital name were eliminated and images were transformed into NIfTI format by using an in-house software. In order to analyze images in an isotropic voxel size, all images were resampled to the voxel size of 1 mm × 1 mm × 1 mm. Brain MRI NII format images were segmented using the MedSAM2 algorithm (18) and the segmented data were reviewed by a senior radiologist to ensure the accuracy of segmentation. Each segmented MRI was annotated by a specific anxiety label.
Our deep learning model was developed using ResNet-152 (Figure 2). The input consisted of segmented MRI scan data, and the algorithm generated probability outputs for various categories. The entire cohort was divided in to a training and validation set at the ratio of 7:3. The Softmax cross-entropy loss between predictions and ground truth labels was minimized using a momentum optimizer, with a batch size of 64 and an initial learning rate of 0.01. The learning rate was reduced every 300 iterations using an exponential decay rate of 0.99. Data augmentation techniques included random rotations (0°, 90°, 180°, 270°) along the Z-axis and random flips across the X, Y, and Z axes. L2 regularization was applied to mitigate overfitting. Training concluded after 3,000 iterations, with the model exhibiting the lowest loss being selected. This AI model was specifically designed to classify anxiety vs. non-anxiety cases. Training was conducted on a system equipped with an NVIDIA GTX 4070 GPU (NVIDIA, Santa Clara, CA) and leveraged the TensorFlow framework (Google, Mountain View, CA). Python 3.6.4 was used for all programming tasks.
Architecture of the deep learning algorithm.
Statistical analysis
Baseline data were summarized as frequencies (percentages) for categorical variables and means ± standard deviations for numerical variables. Comparisons were made using the Chi-square test for categorical data and the t-test for numerical data. Model performance was evaluated using receiver operating characteristic (ROC) curves, with areas under the curve (AUCs) calculated for further analysis. Univariate and multivariate logistic regression analyses were performed to identify clinical predictors for anxiety, with a clinical model constructed using backward elimination. The performance metrics including sensitivity, specificity, positive predictive value (PPV), negative predictive value (NPV), and accuracy were determined by the maximum Youden index in the training set. All statistical analyses were conducted using R (version 4.3.1) and Python (version 3.6.4), with a p-value <0.05 considered statistically significant.
Results
Clinicopathologic characteristics
Table 1 summarizes the clinicopathological characteristics of the study population. The cohort comprised 94 males (46.5%) and 108 females (53.5%), with an average age of 59.4 years. A history of smoking was reported in 30 patients (14.8%). Adenocarcinoma was the most common histological type, representing 81.2% (n = 164) of cases. Tumors were predominantly located on the right side (57.9%, n = 117), with an average size of 1.8 cm. Lymph node metastasis was detected in 22 patients (10.9%). Based on the HADS-A scale, 80 individuals (39.6%) were categorized as having anxiety. Subgroup analysis comparing the training (n = 141) and the validation groups (n = 61) revealed no statistically significant differences between the two groups.
Variables associated with postoperative anxiety
In the univariable analyses (Table 2), larger tumor size [odds ratio (OR), 2.334; 95% confidence interval (CI), 1.546–3.479; p = 0.003] and occurrence of lymph node metastasis (OR, 1.999; 95% CI, 1.133–3.528; p = 0.017) were significantly associated with postoperative anxiety. Similarly, in the multivariable analyses, larger tumor size (OR, 2.044; 95% CI, 1.736–3.276; p = 0.002) and occurrence of lymph node metastasis (OR, 2.078; 95% CI, 1.023–3.221; p = 0.043) independently predicted postoperative anxiety.
Predictive performance of deep learning signature
The distributions of the deep learning score were illustrated in Figure 3, with the increase of deep learning scores, more patients experiencing postoperative anxiety were observed in the training and validation sets. As displayed in Figure 4, in the training set, the ability of the deep learning signature for predicting postoperative anxiety yielded an AUC of 0.865 (95% CI, 0.800–0.930). In addition, in the validation set, the deep learning signature achieved an AUC of 0.822 (95% CI, 0.695–0.950). The performance metrics were detailed in Table 3, the sensitivity, specificity, PPV, NPV, and accuracy of the deep learning signature was 82.1%, 85.6%, 79.3%, 88.0%, and 84.4% in the training set, and 83.3%, 83.8%, 76.9%, 88.6%, and 83.6% in the validation set. Moreover, as shown in Figure 5, the calibration curve and decision curve analyses indicated that the developed deep learning signature yielded satisfactory clinical usefulness in both training and validation set.
The distribution of the deep learning score and anxiety in the (A) training and (B) validation sets.
The ROC curves of the deep learning signature for predicting anxiety in the training and validation sets.
The (A) calibration curves and (B) decision curves of the deep learning signature.
Discussion
Research indicates that anxiety is more common among lung cancer patients compared to healthy individuals (8, 11, 19). This trend persists even after surgery, with postoperative lung cancer patients showing higher anxiety levels than their healthy counterparts (20). In this investigation, the HADS-A scale was employed to assess anxiety in postoperative lung cancer patients. Additionally, a deep learning model was developed using brain MRI data, demonstrating that patients with higher deep learning scores exhibited elevated anxiety rates based on HADS-A. The model achieved an AUC of 0.822 in the validation set for predicting postoperative anxiety.
Given the significant proportion of anxiety in patients suffered from lung cancer, identifying risk factors is crucial for improving clinical management (9, 11). Prior studies have suggested that younger, non-surgical lung cancer patients are more prone to anxiety (11), while others have linked anxiety to dyspnea, severe pain, and diabetes (21). However, these studies often lacked comprehensive parameters, such as surgical details and tumor stage. To address this gap, our study incorporated a broader range of variables and found that tumor size and lymph node metastasis were independently associated with increased anxiety risk in postoperative patients. This may be attributed to pain and discomfort from advanced disease.
Anxiety adversely affects cancer prognosis, with studies linking it to higher mortality in breast and gastric cancer patients (22). Similarly, lung cancer patients with anxiety experience reduced survival rates (8, 12). Early identification of postoperative anxiety is therefore vital for optimizing treatment outcomes. Radiomics, which extracts detailed features from medical images, offers a promising tool for tumor diagnosis, prognosis, and treatment planning (13–16). However, this study has limitations. First, its single-center design limits the generalizability of the deep learning model, as external validation is lacking. Second, the dataset may introduce selection bias and confounding factors. Although multivariable regression was used to adjust for predictors, some variables' impacts remain unaddressed. Future studies with larger, more diverse cohorts are needed to confirm these findings and enhance the model's robustness.
Conclusion
Our deep learning signature harbor the potential to serve as an effective biomarker to predict postoperative anxiety in patients receiving lung cancer surgery.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Nasim F Sabath BF Eapen GA. Lung cancer. Med Clin North Am. (2019) 103(3):463–73. 10.1016/j.mcna.2018.12.00630955514 · doi ↗ · pubmed ↗
- 2Siegel RL Miller KD Jemal A. Cancer statistics, 2020. CA Cancer J Clin. (2020) 70(1):7–30. 10.3322/caac.2159031912902 · doi ↗ · pubmed ↗
- 3Zhang Z Yang S Ma Y Zhou H Wu X Han J Consistency of recommendations for the diagnosis and treatment of non-small cell lung cancer: a systematic review. Transl Lung Cancer Res. (2021) 10(6):2715–32. 10.21037/tlcr-21-42334295672 PMC 8264323 · doi ↗ · pubmed ↗
- 4Bassanelli M Ramella S Zeuli M Ceribelli A. Radiotherapy and immunotherapy: the power of the teamwork for the treatment of NSCLC. Anticancer Res. (2022) 42(5):2241–7. 10.21873/anticanres.1570435489718 · doi ↗ · pubmed ↗
- 5Yang Q Luo LC Li FM Yi Q Luo W. Survival outcomes of radiofrequency ablation compared with surgery in patients with early-stage primary non-small-cell lung cancer: a meta-analysis. Respir Investig. (2022) 60(3):337–44. 10.1016/j.resinv.2022.01.00235172951 · doi ↗ · pubmed ↗
- 6Choi SH Yoo SS Lee SY Park JY. Anti-angiogenesis revisited: reshaping the treatment landscape of advanced non-small cell lung cancer. Arch Pharm Res. (2022) 45(4):263–79. 10.1007/s 12272-022-01382-635449345 · doi ↗ · pubmed ↗
- 7Siwik CJ Phillips K Zimmaro L Salmon P Sephton SE. Depressive symptoms among patients with lung cancer: elucidating the roles of shame, guilt, and self-compassion. J Health Psychol. (2022) 27(5):1039–47. 10.1177/135910532098833133478252 · doi ↗ · pubmed ↗
- 8Arrieta O Angulo LPNúñez-Valencia C Dorantes-Gallareta Y Macedo EO Martínez-López D Association of depression and anxiety on quality of life, treatment adherence, and prognosis in patients with advanced non-small cell lung cancer. Ann Surg Oncol. (2013) 20(6):1941–8. 10.1245/s 10434-012-2793-523263699 · doi ↗ · pubmed ↗