Quality of Postoperative Recovery in Patients Undergoing Video Laparoscopy Cholecystectomy in a University Hospital
Raphael K Confessor de Sousa, Hugo W Araújo, Juliana M Freire, Matheus H De Almeida Ribeiro, Ricardo F Arrais

TL;DR
This study evaluates postoperative recovery in patients who had laparoscopic cholecystectomy and finds that recovery is excellent, with gender and anesthetic technique affecting outcomes.
Contribution
The study identifies gender and anesthetic technique as factors influencing postoperative recovery quality after laparoscopic cholecystectomy.
Findings
Patients undergoing ELC achieved excellent postoperative recovery scores.
Gender and anesthetic technique significantly influenced recovery quality.
No significant difference was found between preoperative and postoperative QoR-15 scores overall.
Abstract
Postoperative recovery (PR) is a complex, multifactorial process, resulting largely from the confluence of physical, physiological, and psychological factors. The Quality of Recovery-15 (QoR-15) questionnaire is a tool used to assess patient's satisfaction with their recovery after surgery. The primary objective of the study is to use the QoR-15 questionnaire to describe and compare the preoperative and 24-hour postoperative scores in patients undergoing elective laparoscopic cholecystectomy (ELC) surgery. This is a cross-sectional, single-center study carried out on patients undergoing ELC, aged 18-70 years, and classified as ASA Physical Status I-III. Patients were invited to answer the QoR-15 during hospitalization, preoperatively, and the next day after the procedure. Data collected included age, sex, weight, height, preoperative fasting time, anesthesia technique, analgesic use…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
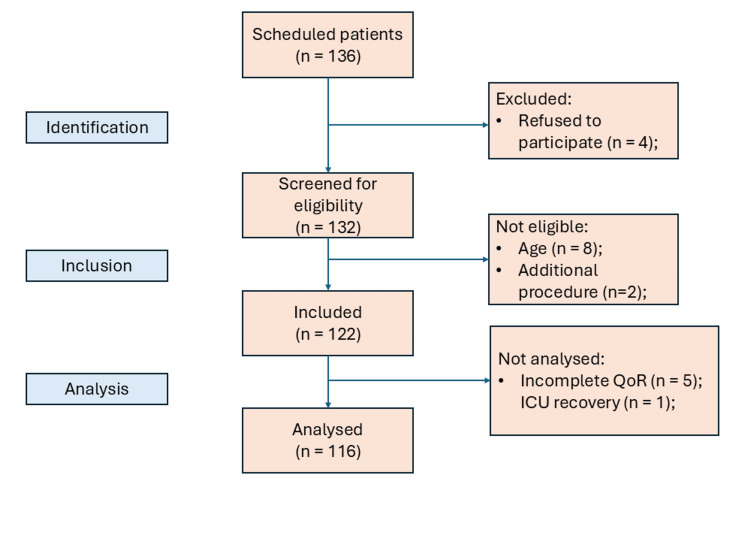 Figure 1
Figure 1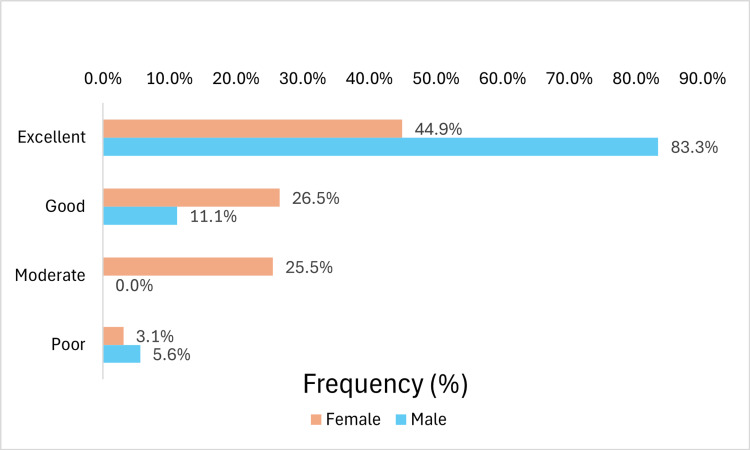 Figure 2
Figure 2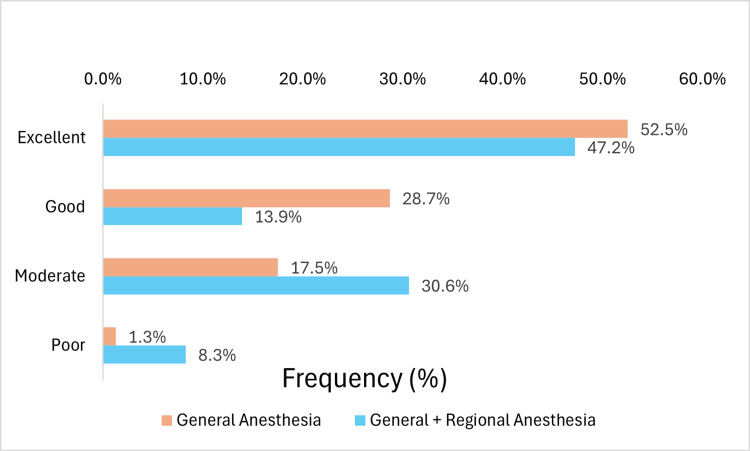 Figure 3
Figure 3| Variable | n (%) |
| Gender | |
| Female | 98 (84.5%) |
| Male | 18 (15.5%) |
| BMI classification | |
| Normal range | 26 (22.4%) |
| Overweight | 27 (23.3%) |
| Obese class I | 25 (21.6%) |
| Obese class II | 22 (19.0%) |
| Obese class III | 16 (13.8%) |
| Hypertension | |
| Yes | 47 (40.5%) |
| No | 69 (59.5%) |
| Diabetes | |
| Yes | 23 (19.8%) |
| No | 93 (80.2%) |
| Thyroid disease | |
| Yes | 7 (6.0%) |
| No | 109 (94.0%) |
| ASA physical status | |
| ASA I | 20 (17.2%) |
| ASA II | 81 (69.8%) |
| ASA III | 15 (12.9%) |
| Variable | Mean | Standard deviation |
| Age (years) | 44.2 | 12.5 |
| Weight (kg) | 81.3 | 20.2 |
| Height (meters) | 1.6 | 0.1 |
| BMI (Kg/m2) | 31.8 | 7.3 |
| Fasting time - solids (hh:mm:ss) | 14:49:42 | 0.1514 |
| Fasting time - liquids (hh:mm:ss) | 13:07:54 | 0.1711 |
| Anesthesia duration (hh:mm:ss) | 03:05:03 | 0.0404 |
| Surgery duration (hh:mm:ss) | 02:15:19 | 0.0390 |
| Domain | Pre-operative period1 | Postoperative period1 | P-value2 |
| Physical comfort | 46.0 (49.0-41.0) | 47.0 (50.0-41.0) | 0.1764 |
| Physical independence | 20.0 (20.0-18.0) | 17.0 (20.0-14.0) | < 0.0001 |
| Emotional state | 33.0 (37.3-26.8) | 38.0 (40.0-33.0) | < 0.0001 |
| Psychological support | 20.0 (20.0-20.0) | 20.0 (20.0-20.0) | 0.3849 |
| Pain | 20.0 (20.0-15.0) | 16.0 (19.3-13.0) | < 0.0001 |
| Variables | QoR-15 | P-value2 | |||
| Poor | Moderate | Good | Excellent | ||
| Sex | 0.0052 | ||||
| Female | 3 (75.0%) | 25 (100.0%) | 26 (92.9%) | 44 (74.6%) | |
| Male | 1 (25.0%) | 0 (0.0%) | 2 (7.1%) | 15 (25.4%) | |
| Anesthesia duration - minutes1 | 175.5 (199-153) | 185 (215-165) | 170 (200-134) | 165 (205-150) | 0.2942 |
| Surgery duration - minutes1 | 136.5 (154-119) | 145 (160-125) | 112.5 (144-90) | 120 (160-95) | 0.1506 |
| Anesthesia techniques | 0.0462 | ||||
| General | 1 (25.0%) | 14 (56.0%) | 23 (82.1%) | 42 (71.2%) | |
| General + regional anesthesia | 3 (75.0%) | 11 (44.0%) | 5 (17.9%) | 17 (28.8%) | |
| NSAIDs | 0.5502 | ||||
| Parecoxib | 0 (0.0%) | 4 (16.0%) | 9 (32.1%) | 13 (22.0%) | |
| Tenoxicam | 3 (75.0%) | 18 (72.0%) | 13 (46.4%) | 34 (57.6%) | |
| No NSAIDs | 1 (25.0%) | 3 (12.0%) | 6 (21.4%) | 12 (20.3%) | |
| Lidocaine | 0.2049 | ||||
| No | 1 (25.0%) | 9 (36.0%) | 4 (14.3%) | 20 (33.9%) | |
| Yes | 3 (75.0%) | 16 (64.0%) | 24 (85.7%) | 39 (66.1%) | |
| Ketamine | 0.8106 | ||||
| No | 1 (25.0%) | 11 (44.0%) | 10 (35.7%) | 26 (44.1%) | |
| Yes | 3 (75.0%) | 14 (56.0%) | 18 (64.3%) | 33 (55.9%) | |
| Magnesium sulfate | 0.7384 | ||||
| No | 4 (100.0%) | 23 (92.0%) | 26 (92.9%) | 50 (84.7%) | |
| Yes | 0 (0.0%) | 2 (8.0%) | 2 (7.1%) | 9 (15.3%) | |
| Clonidine | 0.5852 | ||||
| Yes | 0 (0.0%) | 7 (28.0%) | 8 (28.6%) | 21 (35.6%) | |
| No | 4 (100.0%) | 18 (72.0%) | 20 (71.4%) | 38 (64.4%) | |
| Dexmedetomidine | 1 | ||||
| Yes | 0 (0.0%) | 1 (4.0%) | 1 (3.6%) | 4 (6.8%) | |
| No | 4 (100.0%) | 24 (96.0%) | 27 (96.4%) | 55 (93.2%) | |
| Methadone | 0.5543 | ||||
| Yes | 1 (25.0%) | 2 (8.0%) | 3 (10.7%) | 5 (8.5%) | |
| No | 3 (75.0%) | 23 (92.0%) | 25 (89.3%) | 54 (91.5%) | |
| Remifentanil | 0.4235 | ||||
| No | 3 (75.0%) | 18 (72.0%) | 18 (64.3%) | 47 (79.7%) | |
| Yes | 1 (25.0%) | 7 (28.0%) | 10 (35.7%) | 12 (20.3%) | |
| Dipyrone | 0.7786 | ||||
| No | 0 (0.0%) | 4 (16.0%) | 6 (21.4%) | 14 (23.7%) | |
| Yes | 4 (100.0%) | 21 (84.0%) | 22 (78.6%) | 45 (76.3%) | |
| Tramadol | 0.4788 | ||||
| No | 4 (100.0%) | 20 (80.0%) | 26 (92.9%) | 53 (89.8%) | |
| Yes | 0 (0.0%) | 5 (20.0%) | 2 (7.1%) | 6 (10.2%) | |
| Intravenous morphine | 0.7573 | ||||
| No | 4 (100.0%) | 23 (92.0%) | 27 (96.4%) | 57 (96.6%) | |
| Yes | 0 (0.0%) | 2 (8.0%) | 1 (3.6%) | 2 (3.4%) | |
| Nalbuphine | 0.0974 | ||||
| No | 3 (75.0%) | 25 (100.0%) | 27 (96.4%) | 57 (96.6%) | |
| Yes | 1 (25.0%) | 0 (0.0%) | 1 (3.6%) | 2 (3.4%) | |
| Prophylaxis of nausea and vomiting performed intraoperatively | 0.3641 | ||||
| One medication class | 1 (25.0%) | 2 (8.0%) | 1 (3.6%) | 6 (10.2%) | |
| Two or more classes | 3 (75.0%) | 23 (92.0%) | 27 (96.4%) | 53 (89.8%) | |
| 24h postoperative analgesic medications | 0.7409 | ||||
| As-needed prescription | 0 (0.0%) | 1 (4.0%) | 3 (10.7%) | 3 (5.1%) | |
| One to two time-scheduled medications. | 4 (100.0%) | 23 (92.0%) | 25 (89.3%) | 52 (88.1%) | |
| Three or more time-scheduled medications. | 0 (0.0%) | 1 (4.0%) | 0 (0.0%) | 4 (6.8%) | |
| Prophylaxis of nausea and vomiting performed 24h postoperatively | 0.1724 | ||||
| No prophylaxis | 1 (25.0%) | 11 (44.0%) | 15 (53.6%) | 21 (35.6%) | |
| One medication class | 2 (50.0%) | 14 (56.0%) | 13 (46.4%) | 37 (62.7%) | |
| Two or more classes | 1 (25.0%) | 0 (0.0%) | 0 (0.0%) | 1 (1.7%) | |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsEnhanced Recovery After Surgery · Cardiac, Anesthesia and Surgical Outcomes · Nausea and vomiting management
Introduction
Postoperative recovery (PR) is a process involving physical, psychological, and physiological factors to reestablish the patient's preoperative status [1]. Traditionally, PR has been evaluated based on specific biological, physiological, or other clinical outcomes, such as mortality, length of hospital stay, and recovery of pulmonary or renal function. Despite their importance, these variables do not always reflect patient satisfaction [2].
In line with this approach, anesthesia practitioners typically emphasize indicators related to outcomes concerning the immediate postoperative period, such as the restoration of physiological functions (e.g., arousal, respiration, thermoregulation, and management of nausea and vomiting) and the utilization of hospital resources, including length of stay and admission to intensive care units [3].
To assess PR prior to discharge from the post-anesthesia care unit (PACU), the modified Aldrete-Kroulik score can be used [4]. For the intermediate phase, which corresponds to the period from admission to the ward until hospital discharge, one of the tools used is the Quality of Recovery (QoR) Scale. In the late phase, after hospital discharge, assessments include quality of life scores and measurement of daily life activities, such as the six-minute walk test, the Community Health Activities Model Program for Seniors, the Short Form Six Dimensions (SF-6D) or the EuroQol Five Dimensions (EQ-5D) [2,5,6].
Evaluating the effectiveness of interventions designed to enhance patient satisfaction after procedures requires a patient-centered approach. The health team is responsible for optimizing recovery and can utilize tools that assess aspects of physical and mental comfort [7]. The QoR-15 is a PR assessment instrument that produces results ranging from 0-150 (0 being a poor recovery and 150 being an excellent recovery), with a response time of approximately three minutes. It presents five dimensions to be assessed in PR: pain, physical comfort, physical independence, psychological support, and emotional state [8]. The original version created in English has been translated into several languages, including Portuguese, and validated as a reliable and responsive patient-centred outcome metric [9,10].
The primary objective of this study is to use the QoR-15 tool to measure and compare preoperative and 24-hour postoperative scores in patients undergoing elective laparoscopic cholecystectomy (ELC) at a university hospital. As a secondary evaluation, we seek to describe and analyze the relationship between the QoR-15 score and anesthetic, surgical, and patient factors.
Materials and methods
A cross-sectional study was conducted with 132 patients undergoing ELC at the Onofre Lopes University Hospital (HUOL), located in Natal, Brazil, from September 2022 to July 2024. The project was approved by the institution's ethics committee, under validation number 5.621.709 and ethical clearance certificate 61280522.0.0000.5292 (September 2nd, 2022).
The sample size was estimated to detect differences between preoperative and postoperative QoR-15 scores of 14 points, considering a standard deviation of 40 points, a statistical power of 95%, and an alpha error of 5% [11]. A total of 110 patients was required. To mitigate a potential 20% loss, data collection was planned for 132 patients.
Patients who were scheduled to undergo elective laparoscopic cholecystectomy were approached and invited to participate in the study. If accepted, they signed the informed consent form (ICF). The inclusion criteria were patients aged between 18 and 70 years with ASA physical status I-III [12]. The study excluded patients who did not consent to participate or withdrew their consent, pregnant women, individuals with cognitive impairments or neurological conditions that prevented them from understanding the questionnaire, and those requiring postoperative monitoring in the intensive care unit (ICU).
Patients completed a printed version of the QoR-15 assessment upon admission to the surgical center in the immediate preoperative period and again the next day, within 24 hours after the procedure. Additional data were collected, including age, sex, weight, height, body mass index (BMI), preoperative fasting time, anesthesia technique (general, regional, or combined), analgesic medications used intra- and postoperatively, duration of anesthesia and surgery, type of procedure and use of antiemetics. Data were collected by the authors of the study or by resident physicians previously trained in the application of the questionnaire.
The variables were represented by descriptive measures, such as frequency and percentage, median, interquartile range (IQR: Q3-Q1), mean, and standard deviation. The QoR-15 information was analyzed using the nonparametric Wilcoxon test. In addition to the numerical value obtained in the total QoR-15 scores, the results were categorized as proposed by Kleif and Gögenur [13]: under 90, 90-121, 122-135, and 136-150, representing, respectively, a poor, moderate, good or excellent recovery.
Some variables were compared according to the postoperative QoR-15 score. For this analysis, Fisher's exact test was applied to categorical variables. For numerical variables, the Kolmogorov-Smirnov test was used to verify the normality of the data. When the hypothesis of normality was rejected, the Kruskal-Wallis test was used. The Mann-Whitney test was used to verify whether the variables age, weight, and BMI presented higher values in female patients compared to male patients.
For all analyses, a significance level of α = 5% was adopted. Data were processed and analyzed using R programming language (R Core Team, 2023, R Foundation for Statistical Computing, Vienna, Austria) and presented following the STROBE (Strengthening the Reporting of Observational Studies in Epidemiology) guidelines [14].
Results
A total of 136 patients had ECL scheduled during the research period and were invited to participate, however, only 116 were analyzed, as shown in Figure 1. Information on patient characteristics, fasting time, and duration of the procedure can be found in Tables 1-2. The patients were between 21 and 70 years old, with a mean weight of 81.3 kg (standard deviation: 20.2 kg) and a mean height of 1.6 m (standard deviation: 0.1 m).
Organization Chart of Research Participants
Among the demographic variables analyzed (age, weight, and BMI), only BMI showed a statistically significant difference between the sexes. The median BMI was 32.5 kg/m² (IQR: 37.9-26.9) in females and 27.6 kg/m² (IQR: 31.1-24.5) in males, with a p-value of 0.0246.
In the data analysis, no significant difference was observed in the total QoR-15 score between the preoperative period (135.0, IQR: 143.0-125.0) and the postoperative period (136.0, IQR 142.0-121.7) (p = 0.4803). The scores for the five dimensions assessed by the questionnaire are presented in Table 3. Significant differences were identified between the preoperative and postoperative periods in the following domains: physical independence, emotional state, and pain.
The association between the collected data and the categorized postoperative QoR-15 score can be seen in Table 4. There was statistical significance between the variables sex (p-value=0.0052) and anesthesia technique (p-value=0.0462).
Among men, 83.3% reported excellent recovery, 11.1% good, and 5.6% poor. On the other hand, among women, 44.9% had excellent recovery, 26.5% good, 25.5% moderate and 3.1% poor (Figure 2).
Overall Postoperative QoR-15 Scores According to SexQoR-15: Quality of Recovery-15
Regarding the anesthesia technique, among patients who underwent general anesthesia, 52.5%, 28.7%, 17.5%, and 1.3% reported excellent, good, moderate, and poor recovery, respectively. In comparison, patients who received a combination of general and regional anesthesia reported recovery rates of 47.2%, 13.9%, 30.6%, and 8.3%, following the same order (Figure 3).
Among the patients who received a regional block technique: 27 (75%) underwent wound infiltration, 4 (11.1%) received spinal anesthesia, 3 (8.3%) had an epidural, and 2 (5.6%) received a transversus abdominis plane block. The primary local anesthetic used was ropivacaine (80.6%), followed by bupivacaine (11.1%). The hospital's postoperative analgesic protocol included dipyrone as the first-line option and tenoxicam as the second-line option, both on a scheduled regimen. In cases of allergy to either substance, paracetamol was used as an alternative. Tramadol was the primary rescue medication for pain relief.
Postoperative QoR-15 Scores Categorized According to Anesthetic TechniquesQoR-15: Quality of Recovery-15
Discussion
Modern PR is a multifaceted concept that extends beyond traditional metrics like mortality and hospital length of stay, emphasizing the importance of the patient’s subjective experience. Recent studies highlight that patients prioritize the restoration of daily activities, symptom management, and emotional well-being over purely clinical outcomes, such as the timing of hospital discharge [15].
Studies have demonstrated the utility of the QoR-15 across diverse surgical contexts, where it has been used in both observational studies and clinical trials to assess the impact of interventions such as peripheral nerve blocks and different anesthetic techniques [16]. The present study, conducted in a university hospital, found that the QoR-15 score in the postoperative period was 136, with no significant difference in relation to the preoperative period. However, analyzing the domains, there was an improvement in the emotional state, but a reduction in physical independence and pain, reflecting the complexity of postoperative recovery. Anxiety levels are often higher in the preoperative period, with a Brazilian study showing that over 50% of patients experience this emotion before elective procedures [17]. This may explain the lower satisfaction with emotional well-being before surgery.
It was observed that gender was a statistically significant variable in relation to postoperative QoR-15, with males presenting higher scores. Approximately 83% of male patients reported an excellent recovery, compared to 45% of females. A similar finding was reported by Kleif et al. [18] in a study of patients undergoing laparoscopic surgery for appendicitis treatment, where female patients had recovery scores approximately 21% lower than male patients on the first postoperative day. Another study concluded that sex is an independent factor in anesthesia and surgery recovery [19]. Female sex hormones, particularly progesterone, may play a role, with premenopausal women experiencing poorer overall outcomes [19]. While it is important to account for potential differences in subjective perception between sexes regarding the various domains assessed by the questionnaire, the lack of sex homogeneity represents a limitation of the present study.
Analysis of the anesthetic technique showed differences in postoperative QoR-15, with a lower score in patients who used some type of locoregional block. In the literature, the association between peripheral blocks and the quality of recovery measured by QoR-15 presents conflicting results. In breast surgeries, some studies have reported benefits in recovery with the use of peripheral blocks [20,21]. On the other hand, in minimally invasive thoracic surgeries, although a meta-analysis showed a positive effect with regional anesthesia [22], a recent randomized clinical trial found no significant advantages in using erector spinae plane block (ESP-block) for pain, opioid consumption, or QoR-15 [16]. In patients undergoing laparoscopic ventral hernia repair, the addition of an ESP block did not demonstrate an improvement in scores in a randomized, placebo-controlled clinical trial [23].
The disparity may reflect differences between surgical sites, predominance of somatic or visceral pain, and variations in the concentrations and volumes of local anesthetics. In the analysis of this study, several blockade techniques were grouped (wound infiltration, spinal anesthesia, epidural, and fascia blocks). Therefore, it was not possible to identify which of them specifically influenced the outcomes. Thus, conclusions about this association are limited.
This study has additional limitations that deserve to be noted. First, due to its observational design, it is not possible to establish causal relationships. In addition, although the questionnaire administrators were instructed to remain neutral, application bias cannot be completely excluded. The use of questionnaires also indicates the potential for recall bias. Finally, this is a single-center study, with assessment of postoperative recovery limited to the first 24 hours after the procedure, in a public university hospital in a developing country, where socioeconomic and cultural factors may influence the results. Therefore, extrapolation of the findings to other populations should be done with caution.
Conclusions
In this analysis, most patients reported an excellent or good postoperative recovery; however, when compared to preoperative scores, there was no overall statistical difference. Among the perioperative factors evaluated, the variables sex and anesthetic technique showed an association with the quality of recovery perceived by the patients. Due to the observational nature of the study and the limitations pointed out, it is understood that further studies are necessary to elucidate and extrapolate the data presented.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Conceptual frameworks of postoperative recovery: a scoping review J Surg Res Many BT Hasan M Raval MV Holl JL Abdullah F Ghomrawi H 26527326320213374057410.1016/j.jss.2021.01.031 · doi ↗ · pubmed ↗
- 2What does it really mean to "recover" from an operation?Surgery Lee L Tran T Mayo NE Carli F Feldman LS 21121615520142433175910.1016/j.surg.2013.10.002 · doi ↗ · pubmed ↗
- 3A matter of perspective - Objective versus subjective outcomes in the assessment of quality of recovery Best Pract Res Clin Anaesthesiol Bowyer A Royse C 2872943220183052271910.1016/j.bpa.2018.02.003 · doi ↗ · pubmed ↗
- 4The post-anesthesia recovery score revisited J Clin Anesth Aldrete JA 899171995777236810.1016/0952-8180(94)00001-k · doi ↗ · pubmed ↗
- 5Evaluation of the quality of recovery and the postoperative health status after elective surgery [article in Portuguese]Braz J Anesthesiol Ferraz SM Moreira JP Mendes LC Amaral TM Andrade AR Santos AR Abelha FJ 5775836820183019727010.1016/j.bjane.2018.06.002PMC 9391732 · doi ↗ · pubmed ↗
- 6Recovery from outpatient anaesthesia. Factors affecting outcome Anaesthesia Korttila K 222850 Suppl 1995748591310.1111/j.1365-2044.1995.tb 06186.x · doi ↗ · pubmed ↗
- 7Measuring quality of recovery in perioperative clinical trials Curr Opin Anaesthesiol Myles PS 3964013120182984619310.1097/ACO.0000000000000612 · doi ↗ · pubmed ↗
- 8Development and psychometric evaluation of a postoperative quality of recovery score: the Qo R-15Anesthesiology Stark PA Myles PS Burke JA 1332134011820132341172510.1097/ALN.0b 013e 318289 b 84b · doi ↗ · pubmed ↗