Fish oil and probiotic food supplements: consumptions and attitudes of pregnant women in four European countries
Kristiina Jaakkola, Ella Koivuniemi, Kathryn Hart, Natalia Mazanowska, Romana Roccaldo, Laura Censi, Bernadette Egan, Lilja Mattila, Pasquale Buonocore, Eliisa Löyttyniemi, Monique Raats, Stefania Ruggeri, Miroslaw Wielgos, Kirsi Laitinen

TL;DR
This study looked at how pregnant women in four European countries use fish oil and probiotic supplements and their awareness of health recommendations.
Contribution
The study provides new insights into the use and awareness of fish oil and probiotic supplements among pregnant women across diverse European countries.
Findings
About half of the pregnant women used fish oil supplements, while probiotic use was less common.
Finnish women were most likely to know there is no recommendation for probiotic use during pregnancy.
Polish women had the highest awareness of fish oil recommendations for pregnancy.
Abstract
Fish oil and probiotic supplements may be of benefit during pregnancy, but no information on their use across geographically and socioeconomically diverse countries exists. Our aim was to investigate (1) usage of fish oil and probiotic food supplements by pregnant women, (2) awareness amongst pregnant women of the prevailing recommendations and (3) the characteristics of the users and their beliefs regarding potential health effects of food supplement use, and to compare these variables between women from four European countries. The survey was carried out by online questionnaires (n = 1780) in Finland (n = 536), Italy (n = 539), Poland (n = 584), and the United Kingdom (UK) (n = 121). Product information of the supplements used was collected from participants (n = 1356). Of the participants 49% (n = 670) used fish oil, and 10% (n = 132) used probiotic supplements. The median intake…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
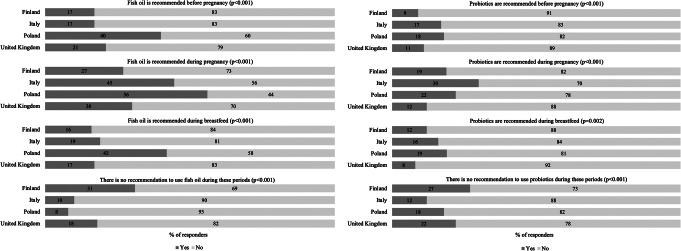 Figure 1
Figure 1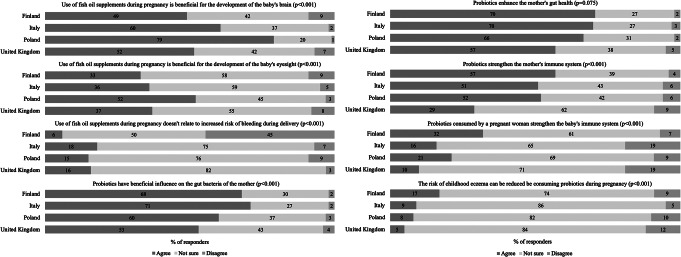 Figure 2
Figure 2- —University of Turku (including Turku University Central Hospital)
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsBreastfeeding Practices and Influences · Child Nutrition and Feeding Issues · Infant Nutrition and Health
Introduction
Food supplements are defined in Europe by the European Food Safety Authority (EFSA) as foods that are concentrated sources of nutrients, (e.g. vitamins or minerals), or other substances with a nutritional or physiological effect and are dosed e.g., in the form of tablets, capsules, or liquids [1]. Supplements are commonly used during pregnancy to support increased requirements due to maternal tissue growth and fetal growth and development [2], or to prevent potential pregnancy related problems including anaemia [3]. Some countries recommend the use of particular food supplements for pregnant women, most commonly iron and folic acid [3, 4].
Fatty fish is the major dietary source of omega-3 (n-3) long-chain polyunsaturated fatty acids (LC-PUFAs) which include docosahexaenoic acid (DHA) and eicosapentaenoic acid (EPA), the important fatty acids for fetal brain development and neurocognitive capabilities [5]. The amount of DHA that the human body can synthesize from its’ precursor, an essential fatty acid alpha linolenic acid (ALA), is insufficient considering the requirements of pregnancy and fetal and child development [6]. Therefore, maternal DHA intake from the diet is of importance and affects the amount that the fetus receives by placental transfer [7]. As fish consumption is variable [8], LC-PUFAs consumption as supplements may be beneficial. European food legislation permits the health benefits of LC-PUFA to be communicated to consumers as a health claims: ‘maternal DHA consumption contributes to normal brain and eye development in the fetus’ [9]. Further, some countries including Poland have included in their dietary recommendations for pregnant women to consume fish oil during pregnancy [10], whilst others, including Finland, Italy and the United Kingdom (UK), consider that the scientific evidence is insufficient to set a recommendation for this specific group of individuals. A daily intake of 200 mg DHA has been proposed to be required during pregnancy which may be achieved either by consuming fish or fish oil supplements [11].
Another food supplement that has raised interest through its potential health benefits if consumed during pregnancy are probiotics, defined by a consensus statement as “live microbes that, when administered in adequate amounts, confer a health benefit on the host” [12]. Consuming probiotics during pregnancy may reduce the risk of diseases in the offspring, such as eczema [13], as indicated by some randomized clinical trials [14, 15]. Further, mothers may benefit from consumption due to their anti-inflammatory potential which could reduce the risk of urogenital infections and mastitis [16]. Due to insufficient scientific evidence a general recommendation on the use of probiotics during pregnancy is not included in the guidance from many countries including those studied in this research (Finland, Italy, Poland, and the UK). The strongest evidence for the benefit of probiotic consumption during pregnancy relates to the lowered risk of childhood allergy and thus the World Allergy Organization (WAO) has issued an evidence-based recommendation for consumption of probiotics by allergy risk families [17]. It is of note that “probiotics” is considered a health claim in the European legislation, thus food supplement packages or marketing material may contain only the bacteria names as part of the ingredient list.
Although the research data on the health effects of the use of fish oil and probiotics during pregnancy is to some extent inadequate, and thus general recommendations for use during pregnancy have not been made, these food supplements are commercially available for consumers and no recommendation against their use during pregnancy has been made either. We have previously demonstrated that the use of multivitamin supplements is common, with 84% of the supplement users consuming these, during pregnancy [2]. The aim of this present study was to investigate (1) usage of fish oil and probiotic food supplements by pregnant women, (2) awareness amongst pregnant women of the prevailing recommendations and (3) the characteristics of the users and their beliefs regarding potential health effects of food supplement use, and to compare these variables between women from four European countries that are geographically and socioeconomically diverse: Finland, Italy, Poland, and the UK. This was carried out by survey and collection of information from food supplement product packages provided by the responders.
Materials and methods
Study design and population
Pregnant women were recruited through social media to participate in a cross-sectional survey on food supplements. The study information was targeted at women aged 18 to 45 years in Finland, Italy, Poland, and the UK and distributed via social media (Facebook) from July 2018 to June 2019. These countries were chosen because of the geographical and socio-economic differences, and because of the differences in the markets for food supplements. A target sample size of 500 participants per country was set, which is comparable to previous studies on food supplement use during pregnancy [18–20]. Additional recruitment channels including childbirth charity web pages were used in the UK. The criteria for inclusion were that the woman was pregnant and understood the main language of the home country. The study was conducted in accordance with the Declaration of Helsinki and approved by the Ethics committee for Human Sciences at the University of Turku, Turku, Finland for all countries (statement 63/2017). Additional ethical approval for Italy was received from the Ethics Committee of Lazio-2, Rome, Italy. Here we focus on the analysis of data relating to pregnancy use of probiotics and LC-PUFA (DHA + EPA), commonly known as fish oil, supplements, with data relating to other food supplements and to the requirements for breastfeeding provided for comparison only.
Survey
Data collection, including information about the use of fish oil and probiotics supplements, knowledge of national recommendations, beliefs regarding the supplement use during pregnancy and participants characteristics, as well as product specific information, was conducted using an electronic questionnaire. Participant characteristics were collected and pre-pregnancy body mass index (BMI) [21] and physical activity level i.e. metabolic equivalent (MET) index [22] were calculated. Two pilot studies were conducted in each country before the main recruitment to test the feasibility of the recruitment method and the understandability of the survey.
Whilst filling in the survey, the responders were asked to add pictures of their food supplement packages, to add weblinks of the products or alternatively to describe the supplements they used (i.e. to provide product name, producer, trademark, nutritional content, and the dose taken). Based on the information provided, the daily intakes of fish oil, more specifically DHA and EPA, and probiotics were calculated, and the probiotic species used were specified. If the number of e.g. capsules was not reported by the women, the guide amount specified in the product information was used to calculate the intake, and if the guide amount was a range, e.g. 1–2, the smaller amount was used for the calculations. In addition, the frequency of fish oil and/or probiotic supplement use during pregnancy was requested (response options: I don’t use this supplement, options 1 to 7 days a week, less than 1 day a week, not sure).
Awareness of the prevailing recommendations provided by governmental or national health bodies regarding the use of fish oil and/or probiotics before and during pregnancy, and during breastfeeding was investigated by statements with response options: yes/no and I cannot say (statements listed in Fig. 1). The beliefs regarding the potential health effects of fish oil and probiotic supplement use during pregnancy were investigated by asking the participants’ level of agreement with statements with response options: strongly agree, agree, disagree, strongly disagree, not sure (statements listed in Fig. 2).
Statistical analyses
Reported food supplements were included in the analysis if the woman had used them at least once a week during pregnancy. Comparison between countries was performed for nominal variables using the chi-squared or Fisher’s exact test, and for continuous data using the Kruskal-Wallis test. The figure on awareness of the recommendations (Fig. 1) did not take into account answers “I cannot say”. The response options “agree” and “strongly agree”, and the response options “disagree” and “strongly disagree” to the eight statements on fish oil or probiotics were combined for the figures, total n = 1780, 6–14 participants missing from the analyses (Fig. 2).
The statistical modelling for the use of fish oil and probiotics was conducted separately. The dependent variables, use of fish oil and probiotics, have three categories (no use of fish oil/probiotics, use of fish oil/probiotics, not using supplements at all). First, the association between each explanatory variable (country, parity, mother’s age, BMI, civil status, education, is mother working in health sector, smoking, alcohol use, MET index, does mother eat vegetables, fruit and berries, whole grain products or fish regularly) and use of fish oil/probiotics were analyzed with chi-square test or Fisher’s exact test. The chi-square test was also used to examine the relations between explanatory variables. If strong associations occurred between explanatory variables, only one was chosen to be entered into the multivariable modelling.
The multinomial logistic regression model for both dependent variables was built based on the results on a univariate approach (i.e. one explanatory variable at a time) explained above. Multivariable multinomial models were constructed including all significant explanatory variables from the univariate approach. The complete case analyses were performed using 1474 participants while all participants with missing data were automatically removed from the analyses. Full data of other food supplement users (i.e. prenatal multivitamin, iron, folic acid etc. vitamins and minerals), have been reported elsewhere [2]).
P-values (two-tailed) less than 0.05 were interpreted as statistically significant and the 95% confidence intervals were calculated. Statistical analyses were performed with SAS System version 9.4 (SAS Institute Inc., Cary, NC, USA) and SPSS version 27 (IBM Corp. Released 2020. IBM SPSS Statistics for Windows, Version 27.0. Armonk, NY: IBM Corp).
Results
Participant characteristics
In all, 1780 women were included in the analysis, 536 from Finland, 539 from Italy, 584 from Poland, and 121 from the UK (flowchart in the Online Resource 1). Of these 1356 participants provided product information for food supplements.
The demographic characteristics of the participants are shown in Table 1. The youngest participants were from Poland and the oldest from the UK and Italy. Two thirds of the participants were primipara. Based on BMI, 63% (1099/1758) had a healthy weight, whilst the highest percentages of participants with overweight or obesity were in Finland and the UK. Self-reported participant morbidity is listed in Online Resource 2. Most of the participants were well educated with university level education. Differences in smoking and drinking habits during pregnancy were observed between countries.
Table 1. Demographic characteristics of the participating women by country (total n = 1780)Total n^c^AllFinlandItalyPolandThe UKP-valueMaternal age,** years**, median (IQR)1778/535/539/583/12130.0 (27.0–33.0)30.0 (27.0–33.0)32.0 (29.0–35.0)28.0 (25.0–31.0)32.0 (28.5–35.0)< 0.001^b^< 25 years, n (%)187 (10.5)45 (8.4)21 (3.9)105 (18.0)16 (13.2)< 0.001^a^25–29 years, n (%)657 (37.0)217 (40.6)140 (26.0)280 (48.0)20 (16.5)30–34 years, n (%)630 (35.4)201 (37.6)219 (40.6)162 (27.8)48 (39.7)≥ 35 years, n (%)304 (17.1)72 (13.5)159 (29.5)36 (6.2)37 (30.6)Weeks of gestation, median (IQR)1779/536/538/584/12124.7 (16.7–32.4)24.4 (15.2–31.7)24.4 (16.7–31.1)25.6 (17.4–33.5)25.1 (17.9–33.5)0.016^b^Pre-pregnancy BMI^d^, median (IQR)1758/534/535/582/10723.1 (20.7–26.3)24.1 (21.5–27.7)22.5 (20.4–25.5)22.7 (20.5–25.5)23.4 (21.5–27.1)< 0.001^b^Underweight, n (%)101 (5.7)11 (2.1)39 (7.3)48 (8.2)3 (2.8)< 0.001^a^Normal weight, n (%)1099 (62.5)313 (58.6)356 (66.5)366 (62.9)64 (59.8)Overweight, n (%)361 (20.5)112 (21.0)93 (17.4)132 (22.7)24 (22.4)Obese, n (%)197 (11.2)98 (18.4)47 (8.8)36 (6.2)16 (15.0)Primipara, n (%)1779/535/539/584/1211195 (67.2)336 (62.8)352 (65.3)427 (73.1)80 (66.1)0.002^a^Diagnoses during this pregnancy, n (%)1776/536/538/581/121Gestational diabetes142 (8.0)62 (11.6)25 (4.6)52 (9.0)3 (2.5)< 0.001^a^Pre-eclampsia and/or hypertension29 (1.6)7 (1.3)10 (1.9)12 (2.1)0 (0.0)0.360^a^Pregnancy related nausea628 (35.4)213 (39.7)206 (38.3)157 (27.0)52 (43.0)< 0.001^a^Medical conditions, n (%)1747/536/528/565/118Allergy and/or asthma340 (19.5)170 (31.7)67 (12.7)86 (15.2)17 (14.4)< 0.001^a^Thyroid disease273 (15.6)52 (9.7)70 (13.39141 (25.0)10 (8.5)< 0.001^a^Migraine or frequent headaches270 (15.5)119 (22.2)50 (9.5)89 (15.8)12 (10.2)< 0.001^a^Rheumatism, arthritis29 (1.7)5 (0.9)12 (2.3)9 (1.6)3 (2.5)0.317^a^Heart disease/hypertension/high cholesterol38 (2.2)18 (3.4)6 (1.1)13 (2.3)1 (0.8)0.065^a^Type I and/or type II diabetesCeliac disease and/or IBS^e^ and/or IBD^f^17 (1.0)7 (1.3)5 (0.9)5 (0.9)0 (0.0)0.609^a^Food intolerance148 (8.5)50 (9.3)46 (8.7)32 (5.7)20 (16.9)< 0.001^a^111 (6.4)44 (8.2)42 (8.0)16 (2.8)9 (7.6)< 0.001^a^Marital status, n (%)1730/513/534/570/113< 0.001^a^Living with a partner611 (35.3)227 (44.2)222 (41.6)132 (23.2)30 (26.5)Married1119 (64.7)286 (55.8)312 (58.4)438 (76.8)83 (73.5)Mother’s education, n (%)1780/536/539/584/121< 0.001^a^Lower than university education540 (30.3)157 (29.3)226 (41.9)130 (22.3)27 (22.3)University education1240 (69.7)379 (70.7)313 (58.1)454 (77.7)94 (77.7)Smoking regularly, n (%)Before pregnancy1778/535/539/583/121549 (30.9)108 (20.2)239 (44.3)182 (31.2)20 (16.5)< 0.001^a^During pregnancy1775/534/539/581/12196 (5.4)14 (2.6)48 (8.9)32 (5.5)2 (1.7)< 0.001^a^Alcohol use,** at least sometimes**, n (%)Before pregnancy1777/535/538/583/1211422 (80.0)448 (83.7)388 (72.1)478 (82.0)108 (89.3)< 0.001^a^During pregnancy1776/535/538/583/12094 (5.3)8 (1.5)67 (12.5)4 (0.7)15 (12.5)< 0.001^a^Leisure time physical activity, categorized MET index value^g^, n (%)1760/531/531/577/121< 0.001^a^Low activity1247 (70.9)268 (50.5)440 (82.9)476 (82.5)63 (52.1)Moderate activity465 (26.4)224 (42.2)87 (16.4)98 (17.0)56 (46.3)High activity48 (2.7)39 (7.3)4 (0.8)3 (0.5)2 (1.7)Working in health sector, n (%)1698/502/505/572/119476 (28.0)229 (45.6)119 (23.6)88 (15.4)40 (33.6)< 0.001^a^ Diet Eats fish at least once a week, n (%)1776/535/538/583/120948 (53.4)276 (51.6)367 (68.2)241 (41.3)64 (53.3)< 0.001^a^Uses vegetables twice a day, n (%)1779/536/538/584/121773 (43.5)315 (58.8)113 (21.0)277 (47.4)68 (56.2)< 0.001^a^Uses whole-grain products daily, n (%)1777/535/539/583/120973 (54.8)420 (78.5)180 (33.4)296 (50.8)77 (64.2)< 0.001^a^^a^Comparison between countries, Chi-square test^b^Comparison between countries, Kruskal-Wallis test^c^Total number of included participants is 1780, 1–82 participants missing from the analyses^d^BMI categorized as underweight (BMI < 18.5), normal weight (BMI 18.5–24.9), overweight (BMI ≥ 25.0 and < 30.0) and obese (BMI ≥ 30.0)^e^Irritable bowel syndrome^f^Inflammatory bowel diseases (Crohn’s disease, Ulcerative colitis)^g^MET index scores < 5 indicating light, scores 5–30 moderate and scores > 30 high physical activity
Use of fish oil and probiotic supplements
Overall 49% (670/1356) of the participants from all the countries studied reported having used a food supplement containing fish oil and 10% (132/1356) had used probiotics during pregnancy (Table 2), most commonly daily for fish oil (daily users 62% in Finland, 74% in Italy, 83% in Poland and 68% in the UK) and for probiotics (daily users 54% in Finland, 47% in Italy, 52% in Poland and 57% in the UK).
When inspecting the data from the product information (Table 2), the largest percentage of fish oil users, 77% (336/436), was in Poland, followed by Italy and the UK, whilst Finland had the lowest percentage of users. The median intake of DHA from the supplements was 220.0 mg/d, and 70.0 mg for EPA/d. Participants from Poland had the highest intake of DHA, whilst Italy had the lowest.
The use of probiotic food supplements also differed between countries, Finland had the highest percentages of probiotic users, 18% (85/470), followed by the UK and Italy, whilst Poland had the lowest, 3% (11/436) (Table 2). Lacticaseibacillus rhamnosus (formerly Lactobacillus rhamnosus) was the most common species in the food supplements consumed in Finland and in Poland, while Bifidobacterium lactis in Italy, and both Bifidobacterium lactis and L. acidophilus were common in the UK. All the species itemized from the reported product information are listed in the Online Resource 3.
Table 2. Frequency of fish oil and probiotic supplement users, calculated intakes of DHA and/or EPA (mg/d), and the most common probiotic species from participants’ self-reported product information by countryTotalAllFinlandItalyPolandUnited KingdomP-valueFish oil, n (%)1356/470/353/436/97670 (49.4)96 (20.4)205 (58.1)336 (77.1)33 (34.0)< 0.001^a^DHA intake (mg/d), median (IQR)667/93/205/336/33220.0 (200.0-600.0)272.0 (136.0-435.0)200.0 (200.0-200.0)500.0 (200.0-600.0)300.0 (300.0-300.0)< 0.001^b^EPA intake (mg/d), median (IQR)355/88/82/154/3170.0 (40.0-120.0)171.4 (73.6–360.0)40.0 (40.0–40.0)70.0 (70.0-71.3)60.0 (60.0–64.0)< 0.001^b^Probiotic users, n (%)1356/470/353/436/97132 (9.7)85 (18.1)27 (7.6)11 (2.5)9 (9.3)< 0.001^a^Most used probiotic species^d^, n (%) Lacticaseibacillus rhamnosus 1356/470/353/436/9787 (6.4)70 (14.9)8 (2.3)6 (1.4)3 (3.1)< 0.001^a^ Bifidobacterium lactis 1356/470/353/436/9766 (4.9)47 (10.0)12 (3.4)2 (0.5)5 (5.2)< 0.001^c^ L. acidophilus 1356/470/353/436/9757 (4.2)44 (9.4)5 (1.4)3 (0.7)5 (5.2)< 0.001^c^ L. casei 1356/470/353/436/9738 (2.8)30 (6.4)5 (1.4)2 (0.5)1 (1.0)< 0.001^c^^a^Comparison between countries, Chi-square test^b^Comparison between countries, Kruskal-Wallis test^c^Comparison between countries, Fisher’s exact test^d^To shorten the text the top three most used probiotic species by country listed in Online Recourse 3
Awareness of the supplement recommendations
Overall, participants from all countries studied had uncertainties about the recommendations for use (Fig. 1). In general participants thought that these food supplements are recommended for use during pregnancy, although Poland was the only country which had issued this recommendation for fish oil.
The largest proportion of the participants who were aware of the prevailing recommendation was in Poland where over half (328/584) of the women knew that fish oil supplements are recommended during pregnancy, while 31% (168/536) in Finland followed by 18% (22/121) in UK and 10% (52/539) in Italy knew that there is no recommendation to use fish oil during these periods. However, 27% (145/536) of the participants in Finland, 45% (240/539) in Italy and 30% (36/121) in UK mistakenly thought that it is recommended to use fish oil supplements during pregnancy.
There is no recommendation to use probiotic supplement in any of the countries, which was known by 27% (143/536) of the participants in Finland, 12% (65/539) in Italy, 18% (106/584) in Poland and 22% (27/121) in UK.
Beliefs of the health effects
Participants’ beliefs regarding the potential health effects of the two supplements were explored with statements presented in a form that corresponds to the correct answer based on the scientific literature. Participants’ knowledge of the health effects of fish oil and probiotic food supplements varied with statistically significant differences between the countries (Fig. 2). The highest proportion of participants agreeing with the statements that fish oil is beneficial for the baby’s brain and eyesight was in Poland, while the lowest was in Finland. In Finland 45% (239/536) of the participants disagreed incorrectly with the statement that fish oil does not relate to an increased risk of bleeding during delivery, whilst in other countries most of the participants responded unsure. Over half of the participants from all the countries agreed that probiotics have beneficial influence on the gut bacteria of the mother, enhance the mothers gut health, and strengthen the mother’s immune system, except in the UK where less than one-third agreed with this statement. In Finland, the highest proportion of the participants agreed with the statements regarding the effects of probiotics on the offspring’s health, less than 10% of the participants from Italy, Poland, and the UK agreed that the risk of childhood eczema can be reduced by consuming probiotics during pregnancy.
Fig. 1. Participants (% of responders) awareness of the prevailing recommendations provided by governmental or national health bodies regarding the use of fish oil (on the left) and probiotic supplements (on the right) before and during pregnancy, and during breastfeeding (n = 1780), comparison between countries using Chi-square test
Fig. 2. Participants (% of responders) beliefs about the potential health effects of fish oil and probiotic supplement use during pregnancy (total n = 1780, 6–14 participants missing from the analyses), comparison between countries using Chi-square test
Characteristics of fish oil and other food supplement users
The characterization of fish oil supplement users and other food supplement users (i.e. prenatal multivitamin, iron, folic acid etc. vitamins and minerals) as compared to supplement non-users is presented in Table 3.
Participants who used fish oil supplement were most likely to be from Finland. Primipara women were more likely to be fish oil users than supplement non-users. Fish oil users’ pre-pregnancy BMI and habits of eating vegetables or using whole-grain products did not differ significantly to those not using supplements.
Table 3. Modelling the characteristics of selected sociodemographic and behavioral factors in fish oil supplement users (n = 664/1474) and other food supplement users (n = 678/1474) as compared to food supplement non-users (n = 132/1474)Fish oil food supplement userOther food supplement^b^ userAdjusted OR95% confidence intervalAdjusted OR95% confidence intervalOverall p-value^a^ Home country < 0.0001Finland11Italy0.180.08–0.420.030.01–0.07Poland0.630.27–1.490.050.02–0.11United Kingdom0.220.07–0.640.120.04–0.32 Pre-pregnancy BMI 0.8739Underweight / normal weight11Overweight0.830.51–1.330.850.52–1.40Obese1.040.50–2.161.20.58–2.50 Primipara 0.0009Yes11No0.480.32–0.700.570.38–0.86 Use vegetables twice a day 0.7501Yes11No0.840.54–1.310.860.54–1.36 Use whole-grain products daily 0.5021Yes11No1.180.78–1.791.290.84-2.00^a^Overall p-values in multinominal logistic regression model including selected sociodemographic and behavioural factors^b^Prenatal multivitamin supplements, other multivitamin supplements and supplements containing vitamin A, folate, vitamin B12, other B vitamins, vitamin C, vitamin D, vitamin E, iodine, calcium, iron, zinc, selenium, chromium, manganese, magnesium, and others of which the participants specified in writing
Characteristics of probiotic and other food supplement users
The characterization of probiotic supplement users and other food supplement users (i.e. prenatal multivitamin, iron, folic acid etc. vitamins and minerals) as compared to supplement non-users is presented in Table 4.
Probiotic supplement users were more likely to be from Finland, and primiparous participants were more likely probiotic users than supplement non-users. Pre-pregnancy BMI and women’s habits of eating vegetables or using whole-grain products did not differ significantly when probiotic users were compared to supplement non-users.
Table 4. Modelling the characteristics of selected sociodemographic and behavioral factors in probiotic supplement users (n = 130/1474) and other supplement users (n = 1212/1474) as compared to supplement non-users (n = 132/1474)Probiotic food supplement userOther food supplement^b^ userAdjusted OR95% confidence intervalAdjusted OR95% confidence intervalOverall p-value^a^ Home country < 0.0001Finland11Italy0.030.01–0.080.070.03–0.16Poland0.020.01–0.070.20.09–0.45United Kingdom0.070.02–0.230.150.05–0.42 Pre-pregnancy BMI 0.4791Underweight / normal weight11Overweight0.980.52–1.820.830.52–1.31Obese0.750.30–1.881.140.57–2.31 Primipara 0.0022Yes11No0.490.29–0.830.520.35–0.75 Use vegetables twice a day 0.0759Yes11No0.560.31–0.990.880.57–1.35 Use whole-grain products daily 0.6204Yes11No1.220.68–2.191.220.82–1.83^a^Overall p-values in multinominal logistic regression model including selected sociodemographic and behavioural factors^b^Prenatal multivitamin supplements, other multivitamin supplements and supplements containing vitamin A, folate, vitamin B12, other B vitamins, vitamin C, vitamin D, vitamin E, iodine, calcium, iron, zinc, selenium, chromium, manganese, magnesium, and others of which the participants specified in writing
Discussion
This study demonstrated that the use of fish oil and probiotic supplements during pregnancy differ between four European countries studied: Finland, Italy, Poland, and the UK. Overall, use of probiotic supplements was less common than that of fish oil supplements. There was uncertainty about the prevailing recommendations of the supplement use by the pregnant women in each country, as well as the health effects of the food supplements for pregnant women or for their unborn child.
In our study about half of the women reported using fish oil supplements and a tenth probiotic supplements during pregnancy. For fish oil these numbers indicate more frequent use than reported in the previous studies in which 4 to 16% of pregnant women in Denmark, Germany, Sweden, Australia and the United States had used the supplements [20, 25–26], but in Iceland the intake was similar, up to 50% among pregnant women [27], as in our study. The use of probiotic supplements during pregnancy has been 9% in other study [28], which is similar to our study. When we further characterized the users, both fish oil and probiotic users were most likely primipara, which is in line with previous findings [29–30, 26], in addition pregnant women use food supplements more often than non-pregnant women [31]. It is of note that our study focused on food supplement use and therefore may have been open to selection bias such that those women with an interest in supplementation were more likely to participate.
The median daily intake of DHA in the supplement consumers was in line with the consensus recommendation of 200 mg/d in each of the studied country (84% of all participants received 200 mg or more of DHA per day from the food supplements). It is of note that the consensus recommendation concerns intake from diet and from the supplements [11], whilst we had no information on the dietary intake of DHA. Nevertheless, intake of DHA from the supplements appears to be of importance as the intake from diet is typically insufficient: e.g. in a previous Polish study only 8% (n = 100) of the pregnant women had intake > 200 mg/d DHA from food (mainly fish and eggs), and only 10% of the pregnant women ate fish twice a week as recommended [32]. It was shown in a cross-sectional survey that pregnant women in the US had a mean intake of 67.5 mg/d of DHA from the food [24]. In our study Poland had the highest intakes of DHA from the supplements and the highest percentage of participants who used fish oil supplements compared to other countries studied. This is reasonable as Poland is the only country with a recommendation to use DHA as a food supplement (200 mg/d for all, and 1000 mg/d for those at risk) during pregnancy [10]. The knowledge of the prevailing recommendations varied in each country, the recommendations were most familiar in Poland where 56% knew about the recommendation to use fish oil during pregnancy, while 31% in Finland knew correctly that there is no recommendation for fish oil usage during these periods. Therefore, diet counselling is needed during health care visits to achieve sufficient intake, e.g. for DHA, which is important for fetal development. However, it has also been noticed that for some food supplements, the daily safe upper intake limit has been exceeded in pregnant women, for e.g. magnesium, folic acid [2] and Fe [33], which emphasizes the importance of instructions for proper use.
In comparison between the four countries, the consumption of probiotics supplements was most common in Finland. The most commonly used probiotic species was Lacticaseibacillus rhamnosus whilst the second most common species was Bifidobacterium lactis. These species are known for their effectiveness in preventing antibiotic-associated diarrhea [34], lowering risk of allergy [17] and supporting immune defence [35]. Since the potential health effects differ between probiotic species, the effects of one species cannot be directly generalized to all bacteria species. A systematic review concluded that healthy pregnant women tolerate probiotics well and their use in pregnancy is safe [36], further a randomized controlled trial reported no side effects to the newborn or mother [37].
When inspecting the participants’ responses to statements considering health effects of fish oil and probiotic supplements (based on timely evidence in literature), we observed that the responders were well aware of benefits of probiotics for the mother, while those for the unborn child less well. Approx. 45% of the participants from Finland erroneously considered that fish oil consumption leads to an increased risk of bleeding during delivery. It is of note that studies, including a scientific opinion by the European Food Safety Authority (EFSA), have demonstrated fish oil consumption up to 2.7 g/d during pregnancy safe [38]. Our results indicate that pregnant women have uncertainty about the possible health effects and safety of fish oil use during pregnancy, particularly in Finland. However, it should be noted that there are still knowledge gaps in research regarding the health benefits of the fish oil or probiotic supplements during pregnancy. We have shown before that health care professionals are the most common source of information for women regarding the use of vitamin and mineral food supplements during pregnancy [2]. Some country differences were observed as midwives and nurses were the primary source of information in Finland and in the UK, whilst doctors and general physicians in Italy and in Poland [2]. Similar findings have been seen in other studies too: nurses were identified as a primary source of information in Australian [39], and in US pregnant women [40]. In addition to health care personnel, women’s own intuition and governmental or ministerial web pages are important sources of information for pregnant women regarding the use of food supplements [2]. Further, the recommendation of the supplement use results in higher consumption of the food supplement in question, as appears to be the case for the use of fish oil supplements during pregnancy in Poland. However, it should be noted that further research is needed on whether the information sources differ according to food supplement type, i.e. fish oil or probiotics vs. vitamin and mineral supplements.
Strengths and limitations
The strength of our study is the inclusion of participants from four different Western countries which are geographically and socioeconomically diverse and thus are anticipated to provide a comprehensive cross-sectional view on the use of fish oil and probiotics during pregnancy. Secondly, we collected product information about the food supplements used, from which we calculated the intakes of fish oil, and even more precisely about DHA and EPA, further we also specified the probiotic species, to get as much information as possible about the food supplement products used. The intake and frequency of use were the main focus in this study, while in many other studies, the information on the supplement consumption is reported as a secondary finding. In addition to product information, we collected extensive data on the participants using an electric questionnaire, and when preparing the study questionnaires, a translation process and successful pilot studies were conducted to ensure clarity of the questions as well as consistency among the countries [2].
Limitations include the need for additional recruitment methods in the UK, and, despite this, a lower sample size was gained in the UK as compared to the other countries. It should also be noted that 70% of the participants had a university level education, which might influence participants’ decisions to use dietary supplements. As it is generally known that the most highly educated individuals use nutritional supplements more frequently [33, 41], it can be assumed that the use of food supplements is less common in the entire pregnant population, highlighting the importance of health care professionals in counselling their patients in the appropriate use of food supplements. Further, food consumption habits and socio-economic status can possibly affect the participants’ decision-making regarding the use of food supplements, as studied before [26, 42], and for e.g., it has previously been reported that DHA intake is lower in low-income countries [8], and among those with lower socio-economic status [43]. In addition, we did not collect information about the women’s daily diet using a food diary, which could include e.g. fish oils in the form of fresh fish and foods containing probiotic bacteria, so the total daily intake, taking diet into account, has not been calculated.
Conclusions
In conclusion, half of the pregnant women in the study used food supplements containing fish oil and one-tenth used supplements containing probiotics. Not all pregnant women were familiar with the prevailing recommendations for fish oil and probiotics supplement use, and further differences between countries were observed. We demonstrated that those women who use fish oil supplements receive the amount of DHA recommended by the researchers’ consensus, and that the use during pregnancy was more common in the country in which a recommendation for use during pregnancy has been issued i.e. Poland. Food supplements that contain probiotics were used the most in Finland. This study provides information on the current use of fish oil and probiotics during pregnancy, the knowledge regarding the recommendations as well as beliefs on the potential health benefits in four European countries, which should be considered in the health counselling to ensure appropriate use of the supplements to optimise maternal and neonatal health.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Supplementary Material 1
Supplementary Material 2
Supplementary Material 3
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Food supplements| EFSA [WWW Document] (2024) URL https://www.efsa.europa.eu/en/topics/topic/food-supplements (accessed 4.25.24)
- 2WHO (2012) Guideline: daily iron and folic acid supplementation in pregnant women. Geneva, World Health Organization 23586119 · pubmed ↗
- 3Greenberg JA, Bell SJ, Ausdal WV Omega-3 fatty acid supplementation during pregnancy. Rev Obstet Gynecol 2008 Fall;1(4):162–169. PMID: 19173020; PMCID: PMC 2621042.PMC 262104219173020 · pubmed ↗
- 4Burdge GC, Calder PC (2005) Sep-Oct;45(5):581– 97 Conversion of alpha-linolenic acid to longer-chain polyunsaturated fatty acids in human adults. Reprod Nutr Dev. 10.1051/rnd:2005047. PMID: 1618820910.1051/rnd:200504716188209 · doi ↗ · pubmed ↗
- 5Gil-Sánchez A, Koletzko B, Larqué E (2012) Current understanding of placental fatty acid transport. Curr Opin Clin Nutr Metab Care.;15(3):265– 72. 10.1097/MCO.0b 013e 3283523 b 6e. PMID: 2245077410.1097/MCO.0b 013e 3283523 b 6e 22450774 · doi ↗ · pubmed ↗
- 6Rautava S, Kainonen E, Salminen S, Isolauri E (2012) Maternal probiotic supplementation during pregnancy and breast-feeding reduces the risk of eczema in the infant. J Allergy Clin Immunol.;130(6):1355-60. 10.1016/j.jaci.2012.09.003. Epub 2012 Oct 16. PMID: 2308367310.1016/j.jaci.2012.09.00323083673 · doi ↗ · pubmed ↗
- 7Knapik A, Kocot K, Witek A, Jankowski M, Wróblewska-Czech A, Kowalska M, Zejda JE, Brożek G (2018) Dietary supplementation usage by pregnant women in Silesia - population based study. Ginekol Pol.;89(9):506–512. 10.5603/GP.a 2018.0086. PMID: 3031857810.5603/GP.a 2018.008630318578 · doi ↗ · pubmed ↗
- 8Olsen SF, Mikkelsen TB, Knudsen VK, Orozova-Bekkevold I, Halldórsson TI, Strøm M, Osterdal ML (2007) Data collected on maternal dietary exposures in the Danish National Birth Cohort. Paediatr Perinat Epidemiol.;21(1):76–86. 10.1111/j.1365-3016.2007.00777.x. PMID: 1723918310.1111/j.1365-3016.2007.00777.x 17239183 · doi ↗ · pubmed ↗