Reimplantation of a malleable penile prosthesis in a patient with urethral erosion: a case report
Moussaab Rachid, Omar Lazrak, Hamza Rais, Ghassane El Omri, Younes Houry, Abdeljalil Heddat

TL;DR
A man experienced a rare complication where his penile prosthesis eroded into the urethra and required removal and reimplantation.
Contribution
This case report highlights the management of a rare complication involving penile prosthesis erosion and successful reimplantation.
Findings
Penile prosthesis erosion through the urethra occurred one year after surgery.
Manual extraction, catheterization, and antibiotics resolved the issue.
Successful reimplantation was performed after urethral healing.
Abstract
A 58-year-old man, initially treated for erectile dysfunction, presented with erosion of a penile prosthesis through the urethra one year after his surgical intervention. Clinical examination revealed the extrusion of the left penile prosthesis through the urethral meatus, associated with mild local inflammation and a fever of 39°C. The patient underwent manual extraction of the prosthesis, careful and delicate urethral catheterization, and antibiotic therapy. Two months later, he was readmitted for the insertion of a new penile prosthesis in the left corpora cavernosa and was discharged on the second postoperative day without complications. Thus, erosion of a penile prosthesis is a serious complication requiring prompt removal of the prosthesis, effective antibiotic treatment, and proper urethral healing.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1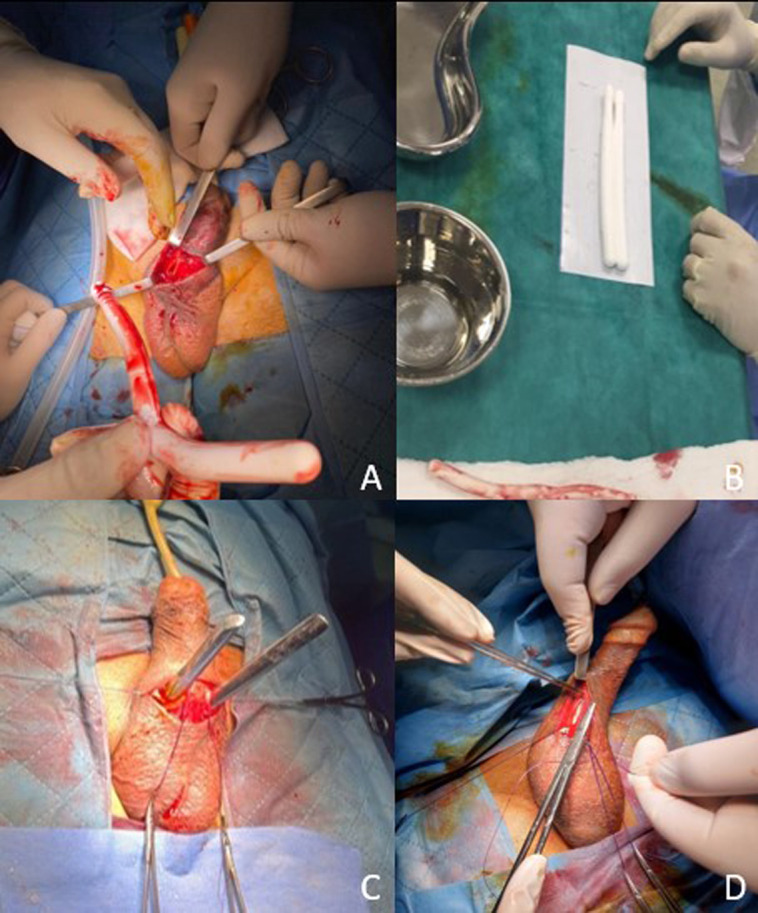 Figure 2
Figure 2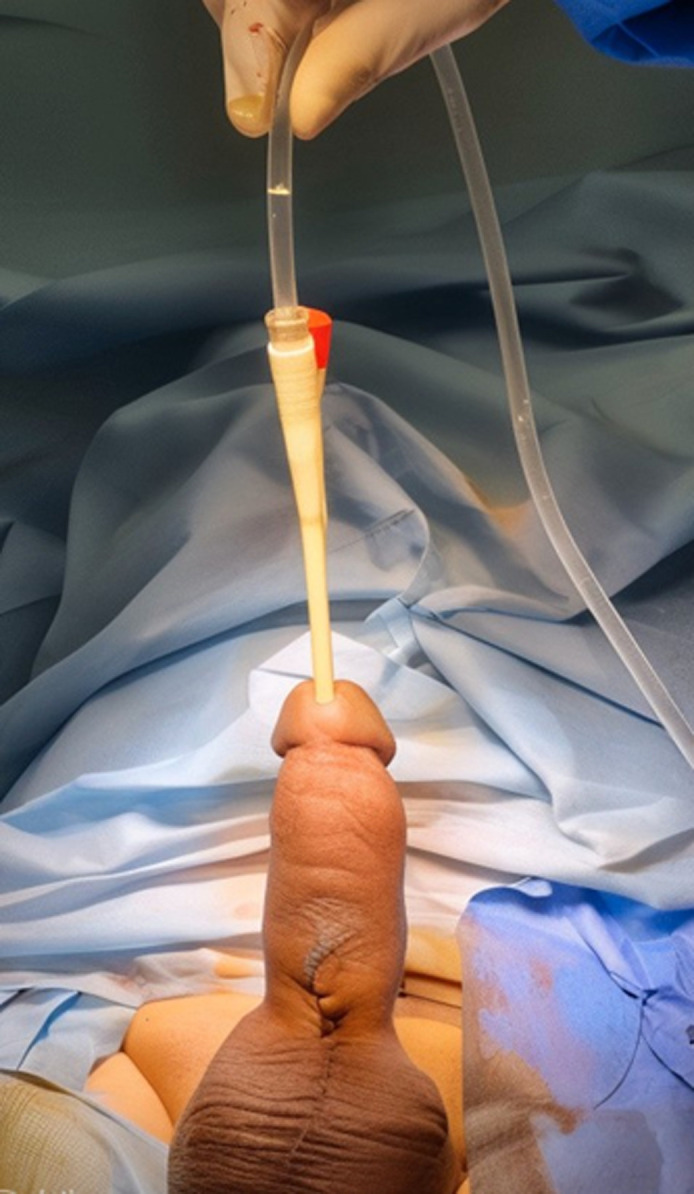 Figure 3
Figure 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsUrological Disorders and Treatments · Sexual function and dysfunction studies · Urologic and reproductive health conditions
Introduction
The penile prosthesis (PP) has evolved significantly since its development in the 1970s. It continues to be used not only to treat erectile dysfunction (ED) that is refractory to medical treatment but also to treat Peyronie's disease, psychological impotence, and penile fibrosis [1]. Despite a tendency to present fewer complications than inflatable implants, malleable implants are not without risks, particularly prosthesis erosion. This phenomenon is characterized by the exteriorization of the prosthetic components following repeated contact with the tunica albuginea, leading to skin perforation [2]. We report a case of erosion of the malleable penile prosthesis (MPP) in a 58-year-old patient who underwent successful reimplantation.
Patient and observation
Patient information: a 58-year-old patient was admitted to the emergency department with erosion of a penile prosthesis through the urethra. The patient had no previous medical history, except erectile dysfunction refractory to medical treatment, for which he had received a malleable penile prosthesis outside our establishment a year before his admission.
Clinical findings: the patient was conscious, hemodynamically and respiratorily stable on clinical examination, but presented with a fever of 39°C. General and abdominal examination revealed no notable abnormalities. Examination of the external genitalia revealed extrusion of the left penile prosthesis through the urethral meatus, associated with mild local inflammation (Figure 1).
erosion of the left malleable penile prosthesis into the urethra
Timeline: the patient indicated that he was being treated outside our establishment for erectile dysfunction refractory to medical treatment. He underwent malleable penile prostheses (11 x 18 cm) over a year ago, and immediate post-operative follow-up revealed no abnormalities. Symptoms began 24 hours before admission, with progressive pain in the distal part of the penis, accompanied by erosion and extrusion of the left penile prosthesis through the urethral meatus. Additionally, the patient began to experience dysuria, but without acute urinary retention, urethrorrhagia, or hematuria.
Diagnostic assessment: therefore, the diagnosis of a penile prosthesis complicated by extrusion was established.
Therapeutic intervention: initially, the patient underwent manual extraction of the prosthesis, careful and delicate urethral catheterization, and dual antibiotic therapy with 3^rd^ generation cephalosporin and gentamicin. His condition gradually improved, with the fever and urinary symptoms disappearing. The patient was hospitalized for seven days. Two months later, the patient was readmitted for the insertion of a new penile prosthesis in the left corpora cavernosa and the replacement of the right prosthesis with a new one. The initial incision was reopened with the release of the envelopes of the penis, followed by dilatation and fitting of a suitable malleable prosthesis (Figure 2). At the end of the operation, the prostheses were in place after skin closure (Figure 3).
stages of penile prosthesis reimplantation: A) extraction of the right penile prosthesis after incision of the corpora cavernosa; B) choice of new malleable penile prostheses; C) dilation of the corpora cavernosa; D) placement of penile prostheses fitted intra-cavernally
final result after penile prosthesis reimplantation
Follow-up and outcomes: the patient was discharged on the second postoperative day without complication. Recovery was marked by the complete restoration of erectile function and the resolution of pain. The patient was assessed at three and six months postoperatively, with clinical examinations revealing no abnormalities.
**Patient perspective: “**Experiencing the extrusion of my penile prosthesis was alarming and painful, but the prompt and careful treatment I received made a significant difference. The removal, infection management, and subsequent placement of a new prosthesis restored my function and relieved my pain. I am grateful for the attentive and effective care”.
Patient consent: informed consent was obtained from the patient for the publication of this article in a journal.
Discussion
Since their development in the 1970s, penile prostheses have played an increasingly important role in the management of erectile dysfunction refractory to medical treatment. They currently represent the last option in the treatment of erectile dysfunction. Implantation of malleable penile prostheses is a simple procedure with good results, but it is not without complications. Although mechanical complications are rare, they are still possible, such as urethral perforation, hematoma, infection, pain, and erosion. Erosion is an uncommon late complication of malleable penile prosthesis surgery. Erosion generally manifests itself by the protrusion of the prosthesis through the glans, the urethral meatus, or the distal part of the penis [3]. It is most often the result of a progressive weakening of the tunica albuginea [4]. This can be caused by excessive dilation of the corpora cavernosa or prolonged pressure from oversized cylinders [5]. The patients most at risk are those with reduced penile sensitivity, such as diabetics and paraplegics, and those who have undergone several operations on the urethra [6].
The clinical symptoms are dominated by dysuria, urethral discharge, and infection of the prosthesis, which may be complicated by balanitis [3]. In fact, a prosthesis that is oversized in width or length could be responsible for urethral compression, causing ischemia of the urethral wall and thereby promoting erosion. On the other hand, erosion of the penile prosthesis has also been reported by several authors as a complication of urethral catheterization. In a study by Steidle et al. [7] of nine patients using clean intermittent catheterization or having an indwelling catheter, the incidence of urethral erosion was high. Although the effective course of action is the removal of the entire device followed by replacement with a MPP, some authors recommend a conservative approach in the absence of infection and necrosis [1]. Additionally, small scrotal erosions can be treated conservatively [8]. Surgery may be reserved for patients with recurrent erosions that do not respond to conservative management. In the reported case, the patient presented with sepsis of urinary origin, so the conservative approach was not indicated. Treatment of erosion depends on the clinical context. One common option is to remove the cylinders and replace the prosthesis after one or two months. Other practitioners opt for a rescue lavage, removing the prosthesis and immediately inserting a malleable prosthesis on the non-eroded parts of the penis [4,5].
Conclusion
Erosion of the penile prosthesis is a complication that should not be underestimated. All surgeons must be alert to this complication. The prosthesis must be removed and the patient covered with an effective course of antibiotics, as well as ensuring that the urethra has healed properly after four to six weeks. On the other hand, patients should be warned of the risk and should seek medical advice if there is any sign of extrusion, to avoid the risk of imminent erosion.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Basiri A Zahir M Successful re-implantation of eroded penile prostheses: Report of two cases and review of the literature Clin Case Rep 20231112 e 83653814426210.1002/ccr 3.8365 PMC 10740338 · doi ↗ · pubmed ↗
- 2Cavayero CT Mc Intosh GV Penile Prosthesis Implantation Stat Pearls 2024 Stat Pearls Publishing
- 3Minhas S Urethral Perforation During Penile Implant Surgery: What to Do J Sex Med 20171478678692867343110.1016/j.jsxm.2017.05.003 · doi ↗ · pubmed ↗
- 4Levine LA Becher EF Bella AJ Brant WO Kohler TS Martinez-Salamanca J Iet al Penile Prosthesis Surgery: Current Recommendations From the International Consultation on Sexual Medicine J Sex Med 20161344895182704525510.1016/j.jsxm.2016.01.017 · doi ↗ · pubmed ↗
- 5Cayetano-Alcaraz AA Yassin M Desai A Tharakan T Tsampoukas G Zurli Met al Penile implant surgery-managing complications Fac Rev 202110733463245910.12703/r/10-73PMC 8483239 · doi ↗ · pubmed ↗
- 6Kim YD Yang SO Lee JK Jung TY Shim HB Usefulness of a malleable penile prosthesis in patients with a spinal cord injury Int J Urol Off J Jpn Urol Assoc 2008151091992310.1111/j.1442-2042.2008.02115.x 18651861 · doi ↗ · pubmed ↗
- 7Steidle CP Mulcahy JJ Erosion of penile prostheses: a complication of urethral catheterization J Urol 19891423736739276985110.1016/s 0022-5347(17)38871-7 · doi ↗ · pubmed ↗
- 8Talib RA Shamsodini A Salem EA Canguven O Al Ansari A Isolated pump erosion of an inflatable penile prosthesis through the scrotum in a diabetic patient Arch Ital Urol Androl Organo Uff Soc Ital Ecogr Urol E Nefrol 2013851535510.4081/aiua.2013.1.5323695409 · doi ↗ · pubmed ↗