Adolescent and Young Adult Cancer Representation in Claims Data
Jacob N. Stein, Christopher Baggett, Jennifer L. Lund, Hannah C. Winslow, KyungSu Kim, Katherine E. Reeder-Hayes

TL;DR
This study examines how well adolescent and young adult cancer patients are represented in insurance claims data.
Contribution
The study introduces a new method to evaluate representation using continuous insurance coverage criteria.
Findings
Adolescent and young adult cancer patients may be underrepresented in claims data.
Continuous insurance coverage criteria can affect the accuracy of claims-based research.
Abstract
This cohort study evaluates the representation of adolescent and young adult patients with cancer in claims research based on continuous insurance coverage criteria.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure
Figure| Characteristic | Registry (N = 20 361), No. (%) | No claims (n = 11 024), No. (%) | Continuous enrollment, No. (%) | |||||
|---|---|---|---|---|---|---|---|---|
| 0 to 12 mo (n = 5912) | −2 to 12 mo (n = 4707) | |||||||
| Total | Private | Medicaid | Total | Private | Medicaid | |||
| Age at diagnosis | ||||||||
| Adolescent (13-19 y) | 1793 (8.8) | 847 (7.7) | 646 (36.0) | 173 (9.6) | 473 (26.4) | 544 (30.3) | 167 (9.3) | 377 (21.0) |
| Emerging adult (20-29 y) | 5655 (27.8) | 2932 (26.6) | 1657 (29.3) | 715 (12.6) | 942 (16.7) | 1291 (22.8) | 650 (11.5) | 641 (11.3) |
| Young adult (30-39 y) | 12 913 (63.4) | 7245 (65.7) | 3609 (27.9) | 1747 (13.5) | 1862 (14.4) | 2872 (22.2) | 1617 (12.5) | 1255 (9.7) |
| Sex | ||||||||
| Female | 12 009 (59.0) | 6356 (57.7) | 3639 (30.3) | 1548 (12.9) | 2091 (17.4) | 2933 (24.4) | 1415 (11.8) | 1518 (12.6) |
| Male | 8348 (41.0) | 4655 (43.3) | 2272 (27.2) | 1087 (13.0) | 1185 (14.2) | 1773 (21.2) | 1019 (12.2) | 754 (9.0) |
| Race and ethnicity | ||||||||
| Hispanic or Latino | 1240 (6.1) | 870 (7.9) | 210 (16.9) | 61 (4.9) | 149 (12.0) | 164 (13.2) | 60 (4.8) | 104 (8.4) |
| Non-Hispanic Black | 3809 (18.7) | 1520 (13.8) | 1521 (39.9) | 248 (6.5) | 1273 (33.4) | 1150 (30.2) | 218 (5.7) | 932 (24.5) |
| Non-Hispanic White | 14 207 (69.8) | 7983 (72.4) | 3886 (27.4) | 2201 (15.5) | 1685 (11.9) | 3153 (22.2) | 2042 (14.4) | 1111 (7.8) |
| Other | 1105 (5.4) | 651 (5.9) | 295 (26.7) | 125 (11.3) | 170 (15.4) | 240 (21.7) | 114 (10.3) | 126 (11.4) |
| Cancer type | ||||||||
| Breast | 5730 (28.1) | 3094 (28.1) | 1754 (30.6) | 745 (13.0) | 1009 (17.6) | 1345 (23.5) | 679 (11.8) | 666 (11.6) |
| Leukemia | 2357 (11.6) | 1154 (10.5) | 809 (34.3) | 229 (9.7) | 580 (24.6) | 604 (25.6) | 209 (8.9) | 395 (16.8) |
| Lymphoma | 4230 (20.8) | 2064 (18.7) | 1374 (32.5) | 474 (11.2) | 900 (21.3) | 1064 (25.2) | 436 (10.3) | 628 (14.8) |
| Melanoma | 3925 (19.3) | 2429 (22.0) | 858 (21.9) | 644 (16.4) | 214 (5.5) | 779 (19.8) | 604 (15.4) | 175 (4.5) |
| Sarcoma | 1697 (8.3) | 849 (7.7) | 532 (31.3) | 193 (11.4) | 339 (20.0) | 429 (25.3) | 181 (10.7) | 248 (14.6) |
| Testicular (germ cell) | 2422 (11.9) | 1434 (13.0) | 585 (24.2) | 350 (14.5) | 235 (9.7) | 486 (20.1) | 325 (13.4) | 161 (6.6) |
| Location | ||||||||
| Urban | 15 771 (77.5) | 8875 (80.5) | 4342 (27.5) | 2069 (13.1) | 2273 (14.4) | 3512 (22.3) | 1920 (12.2) | 1592 (10.1) |
| Rural | 4546 (22.3) | 2119 (19.2) | 1565 (34.4) | 563 (12.4) | 1002 (22.0) | 1190 (26.2) | 511 (11.2) | 679 (14.9) |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsEconomic and Financial Impacts of Cancer · Health Systems, Economic Evaluations, Quality of Life · Palliative Care and End-of-Life Issues
Introduction
Adolescents and young adults (AYAs) (aged 13-39 years) represent a growing segment of the cancer population who face distinct challenges in receiving care, leading to adverse treatment experiences and stagnant survival outcomes.^1^ Research on AYA outcomes and care delivery remains scarce.^2^ A crucial need exists for clinical studies on AYA care delivery to improve care experiences and outcomes, with claims-based data offering valuable data.
Gaps in health insurance are more common among AYAs than any other US age group,^3^ and AYAs without insurance face shorter survival.^4^ Insurance patterns for AYAs are not well documented, hampering use of claims for research. Inclusion in claims-based research often requires continuous enrollment starting months before assessment for preexisting comorbidities and health care use. We evaluated various enrollment criteria and compared the resulting study-eligible populations of AYAs with cancer for claims research.
Methods
This retrospective cohort study used the Cancer Information and Population Health Resource (CIPHR), which links cancer registry and private and Medicaid payer data across North Carolina. Detailed database methods were described previously.^5^ The study was approved by the University of North Carolina Institutional Review Board with a waiver of written informed consent as the project involved a secondary data analysis. The study followed the STROBE reporting guideline.
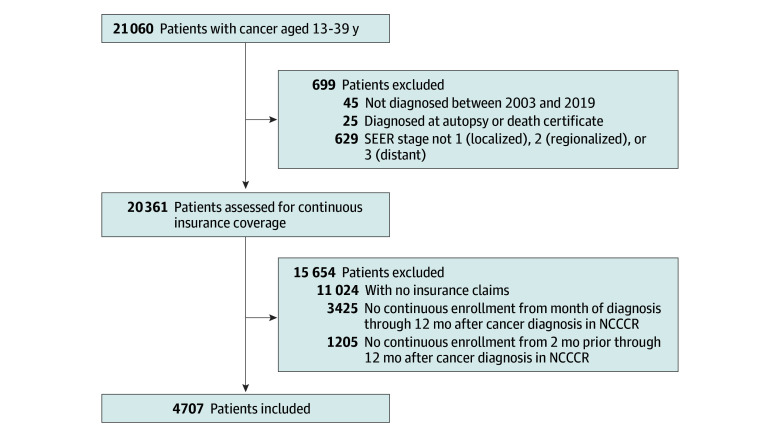
We included individuals aged 13 to 39 years diagnosed with common cancer types in the CIPHR from 2004 to 2019 linked with insurance claims from 2003 to 2020 (Figure). We compared 2 scenarios of continuous enrollment: 2 months before through 12 months after cancer diagnosis and month of diagnosis through 12 months after. We compared sociodemographic characteristics and insurance types across scenarios. Self-reported race and ethnicity (Black, Hispanic, White, other) data were included as variables because they are sociodemographic factors with a known association with differences in US health insurance coverage. The statistical analysis was performed on March 12, 2024, using SAS, version 9.4 (SAS Institute Inc).
Flow Diagram for Study Cohort InclusionNCCCR indicates North Carolina Central Cancer Registry; SEER, Surveillance, Epidemiology, and End Results.
Results
We identified 20 361 AYAs from the cancer registry during the study period (median [IQR] age, 32 [26-36] years; 59.0% female and 41.0% male) (Table), of whom 54.1% did not match to any insurance claims. A total of 4707 patients (22.4%) had continuous enrollment from 2 months before to 12 months after their cancer diagnosis vs 5912 (28.1%) starting from month of diagnosis, which was driven by an increase in Medicaid-insured patients.
Less restrictive continuous enrollment criteria increased representation of Black patients from 30.2% to 39.9% of the total registry cohort, rural patients from 26.2% to 34.4%, and patients with leukemia from 30.2% to 34.3% and lymphoma from 25.2% to 32.5%. Clinical and demographic characteristics were similar across cohorts.
Discussion
This cohort study found that less restrictive continuous enrollment criteria increased the number of AYAs with cancer eligible for inclusion in claims-based research while broadening the diversity, reflecting the processes involved in accessing health insurance for these patients. Many health systems assist patients with gaining insurance at the time of a cancer diagnosis, leading to an uptick in coverage in the month of diagnosis (1205 patients in our cohort). Notable differences were observed across insurers and eligibility scenarios. Rural and Black patients and patients with hematologic cancers were more likely have Medicaid.
A limitation of the less restrictive inclusion criteria is the lack of a lead-in period during which baseline comorbidities or prior care delivery can be assessed, acknowledging that comorbidities may be less common among AYAs. While conducted within a single state, North Carolina is representative of national demographics, and CIPHR reflects similar patterns as Surveillance, Epidemiology, and End Results and Medicare analyses.^6^
We found that AYAs with cancer are underrepresented in claims-based research and recommend that researchers use more lenient continuous enrollment criteria when studying AYAs through claims data to achieve a larger and more representative sample, which may lead to more generalizable findings. This approach is needed to better characterize the care for this underserved population.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Nass SJ, Beaupin LK, Demark-Wahnefried W, . Identifying and addressing the needs of adolescents and young adults with cancer: summary of an Institute of Medicine workshop. Oncologist. 2015;20(2):186-195. doi:10.1634/theoncologist.2014-026525568146 PMC 4319626 · doi ↗ · pubmed ↗
- 2Smith AW, Seibel NL, Lewis DR, . Next steps for adolescent and young adult oncology workshop: an update on progress and recommendations for the future. Cancer. 2016;122(7):988-999. doi:10.1002/cncr.2987026849003 PMC 7521143 · doi ↗ · pubmed ↗
- 3Vaca Lopez PL, Warner EL, Waters AR, . Adaptation and development of a health insurance education program for adolescent and young adult cancer patients. J Adolesc Young Adult Oncol. 2023;12(5):692-700. doi:10.1089/jayao.2022.010336706435 PMC 10611966 · doi ↗ · pubmed ↗
- 4Rosenberg AR, Kroon L, Chen L, Li CI, Jones B. Insurance status and risk of cancer mortality among adolescents and young adults. Cancer. 2015;121(8):1279-1286. doi:10.1002/cncr.2918725492559 PMC 5231922 · doi ↗ · pubmed ↗
- 5Baggett CD, Jackson BE, Green L, . Cancer information and population health resource: a resource for catchment area data and cancer outcomes research. J Natl Cancer Inst Cancer Spectr. 2024;8(5):pkae 069. doi:10.1093/jncics/pkae 06939141446 PMC 11410194 · doi ↗ · pubmed ↗
- 6Reeder-Hayes KE, Wheeler SB, Meyer AM, . Adoption and effectiveness of de-escalated radiation and endocrine therapy strategies for older women with low-risk breast cancer. J Geriatr Oncol. 2021;12(5):731-740. doi:10.1016/j.jgo.2021.01.00333551323 · doi ↗ · pubmed ↗