Recruitment strategies used to enrol healthy volunteers in the first pneumococcal human infection study in Africa: Lessons from Blantyre, Malawi
Edna Nsomba, Anthony E. Chirwa, Clara Ngoliwa, Vitumbiko Nkhoma, Pemphero Liwonde, Edward Mangani, Modesta Reuben, Lorensio Chimgoneko, Lumbani Makhaza, Evaristar Kudowa, Marc Y R Henrion, Neema Toto, Stephen B. Gordon, Dingase Dula, Oren Ziv, Dorcas M Kamuya, Edna Nsomba

TL;DR
This paper describes how healthy volunteers were recruited for a first-of-its-kind pneumococcal infection study in Malawi, highlighting the effectiveness of word-of-mouth recruitment.
Contribution
The study introduces controlled human infection models in Africa and evaluates recruitment strategies for such trials.
Findings
Snowball recruitment (word of mouth) was the most successful method, accounting for 72.3% of participants.
The majority of participants (76.3%) were recruited from the local community rather than college students.
Abstract
Human infection studies (HIS) also known as Controlled Human Infection Models (CHIM) are a relatively new concept in African countries to clinicians, scientists, and communities alike. We have introduced HIS/CHIM studies to Malawi during the last four years by developing an experimental human pneumococcal carriage model. This CHIM was used to test the efficacy of a licensed 13-valent Pneumococcal Conjugate Vaccine (PCV13) against experimental nasal pneumococcal carriage. Traditional and digital recruitment strategies into this novel trial were explored. To describe various methods of recruitment in this first CHIM study in Malawi. The clinical trial within the context of which these data were recorded was registered with the Pan African Clinical Trials Registry (REF: PACTR202008503507113) on 03 August 2020. The project was conducted at the Malawi Liverpool Wellcome Programme (MLW) in…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
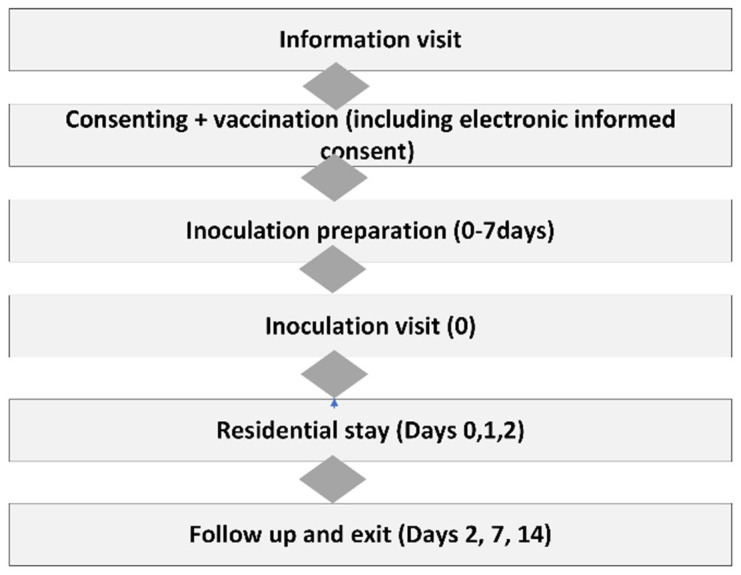 Figure 1
Figure 1| Inclusion criteria | Exclusion criteria |
|---|---|
| • Adults aged 18–40 years
| • Previous pneumococcal vaccination
|
| Total
| Snowball
| Sensitization
| Radio and
| Poster
| |
|---|---|---|---|---|---|
| Male | 209 | 160 (76.6) | 48 (23.0) | 1 (0.4) | 0 (0.0) |
| Female | 90 | 55 (61.1) | 34 (37.8) | 0 (0.0) | 1 (1.1) |
| Total
| Snowball
| Sensitization
| Radio and
| Poster
| |
|---|---|---|---|---|---|
| Male | 195 | 149 (76.4) | 45 (23.1) | 1 (0.5) | 0 (0.0) |
| Female | 83 | 52 (62.7) | 30 (36.1) | 0 (0.0) | 1 (1.2) |
| Column1 | Strongly
| Agree n(%) | Neutral
| Disagree
| Strongly
|
|---|---|---|---|---|---|
| The approach used for study recruitment was appropriate | 146(68.5) | 62(29.1) | 5(2.3) | 0 | 0 |
| The information provided before consenting was appropriate | 155(72.8) | 58(27.2) | 0 | 0 | 0 |
| The medical questions and tests used before consenting were appropriate | 142(66.7) | 66(31.0) | 5(2.3) | 0 | 0 |
| There was sufficient time to consider the study before consenting | 147(69.0) | 60(28.2) | 5(2.3) | 1(0.5) | 0 |
| The finger print scanner was acceptable way to confirm my identification | 164(77.0) | 46(21.6) | 3(1.4) | 0 | 0 |
| The clinical team treated you with respect and kindness. | 173(81.2) | 39(18.3) | 1(0.5) | 0 | 0 |
| The safety monitoring procedures for the study were appropriate | 151(70.9) | 59(27.7) | 3(1.4) | 0 | 0 |
| The study follow up procedures did not cause inconvenience | 122(57.3) | 73(34.3) | 14(6.6) | 4(1.9) | 0 |
| The accommodation provided after inoculation was satisfactory | 146(68.5) | 54(25.4) | 11(5.2) | 2(0.9) | 0 |
| The meals provided at the accommodation were satisfactory | 155(72.8) | 49(23.0) | 8(3.8) | 1(0.5) | 0 |
| The location of the accommodation was convenient | 137(64.3) | 65(30.5) | 8(3.8) | 3(1.4) | 0 |
| The compensation provided by the study was appropriate | 99(46.5) | 72(33.8) | 34(16.0) | 5(2.3) | 3(1.4) |
| I would recommend participant in this study to a friend | 142(66.7) | 63(29.6) | 7(3.3) | 1(0.5) | 0 |
- —Wellcome
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsVaccine Coverage and Hesitancy · Child and Adolescent Health · Global Maternal and Child Health
Introduction
Rationale
Human Infection Studies (HIS), also known as Controlled Human Infection Models (CHIM) involve introducing a pathogen to a healthy individual under carefully monitored conditions. These studies have made important contributions to prevention and treatment of many infectious diseases. High Income Countries (HIC) have utilized these studies to understand biology and develop vaccines for pathogens of clinical and population health importance such as human influenza viruses, respiratory syncytial virus, severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), Staphylococcus and Neisseria species. High literacy levels, equitable access to health care, advanced technology, superior physical and digital health services infrastructure, and high socio-economic status have facilitated the success of these novel studies in HICs.
Malawi, Kenya, Uganda, and Tanzania are four countries that have established HIS in Africa (Malawi: Streptococcus pneumoniae challenge ^ 1 ^ , Kenya ^ 2 ^ and Tanzania ^ 3 ^: Plasmodium falciparum challenge, Uganda: Schistosoma spp challenge ^ 4 ^).
Other countries such as Zambia ^ 5 ^, are following with other study pathogens, and priming their populations for introduction of these novel studies ^ 5 ^. Typically, HIS are conducted first in a HIC and after the technology, standard operating procedures and safety have been established, transferred to a collaborating Low-Income Country (LIC). For example, pneumococcal human challenge trials were conducted in Liverpool for a decade following which technology and standard operating procedures were transferred to Malawi for feasibility testing ^ 6 ^. Similarly, a study of blood-stage controlled human Plasmodium falciparum malaria infection that is ongoing in Tanzania, originated from Oxford University ^ 7 ^.
The first workshop to be convened on human challenge work in Malawi by a technical working group, which included the authors, met in 2017 ^ 8 ^. Clinicians, scientists, ethicists, and community leaders discussed the potential benefits of human infection studies (accelerated vaccine development, capacity building) and risks (safety, acceptability, ethical concerns) ^ 8 ^. The workshop report highlighted: excellent international clinical standards, local capacity building and ownership, a rigorous informed consent process, mitigation of challenges with transport and access to health facilities, appropriate economic compensation, and managing community and media perceptions as key issues to address to ensure success of human infection studies in a setting like Malawi ^ 8 ^.
Next, the researchers conducted a study exploring acceptability of human infection studies using focus groups and key informant interviews with Blantyre-based research staff, medical students, and community representatives, clinicians, ethics committee members, and district health government officials ^ 9 ^. Overall, HIS studies were favourably perceived and potentially beneficial provided the following conditions were met; voluntary and informed consent, rigorous inclusion/exclusion criteria, provision of medical check-ups and monitoring, appropriate compensation, and robust community engagement ^ 9 ^.
Acceptability work paved way for feasibility testing of the human challenge model among 24 healthy volunteers, whose experiences with the trial from recruitment methods, compensation, inoculation with live bacteria, study procedures (nasosorption, nasal scrape with rhino probe, nasal wash, throat swab, saliva collection quarantine and residential stay post-challenge, were sought after trial completion ^ 10 ^. Motivation for joining the study despite initial reservations included altruism, patriotism, and monetary gains ^ 10 ^. Although the participants did not experience adverse events in the short duration of the study (21 days) they were concerned about future unanticipated risks ^ 10 ^. The volunteers admitted that the concept of human challenge trials was completely novel and recommended extending information and education about the model to the wider Malawian population ^ 10 ^.
In the present paper, we discuss experiences and lessons we have learnt about recruitment through the process of scaling up from a feasibility study in tens of participants to a randomized controlled vaccine trial requiring screening of more than 250 participants.
Objectives
We describe methods used in recruiting participants in a pneumococcal CHIM study in Blantyre Malawi and highlight lessons learned in the process.
Methods
Trial design
This was a qualitative description of recruitment methods used to recruit participants in a double-blinded, parallel-arm, randomized controlled trial investigating the efficacy of PCV13 or placebo (allocation ratio PCV13: placebo 1:1) against experimental pneumococcal carriage of Streptococcus pneumoniae serotype 6B (SPN6B). The study protocol has been published in Wellcome Research Open ^ 11 ^.
Methods
Sensitization meetings: Sensitization meetings were conducted at eight surrounding colleges in Blantyre namely Malawi College of Health Sciences ^ 2 ^, Malawi University of Business and Applied Sciences, formerly The Polytechnic ^ 2 ^, Kamuzu University of Health Sciences ^ 1 ^, Malawi Institute of Journalism ^ 1 ^ and Malawi Institute of Tourism ^ 1 ^. Each sensitization meeting was attended by approximately 50 students. Additional sensitization meetings were conducted at the Malawi-Liverpool-Wellcome Programme main site and invited research and clinical staff. Individuals interested in the study provided their telephone numbers to the study staff and verbally consented to be phoned to schedule an information session at the clinic. Sensitization meetings were interrupted from July to August 2021 by school closures due to the fourth COVID wave but resumed in September 2021.
Snowball recruitment: Snowball recruitment or sampling, also called chain-referral sampling, is an informal spread of study-related information to potential participants by word of mouth ^ 11 ^. Snowball recruitment in this study occurred naturally without study staff influence. Potential participants and existing participants shared study information with their peers, who came to volunteer for the study as a result.
Radio and Television: While initially the study team was careful to perform only targeted sensitization during the feasibility study, the proven safety of the model demonstrated for over three years provided later confidence to expand awareness of human infection studies to the wider community. In May 2022, four weekly radio broadcasts about human infection studies and the PCV13 study were conducted by study clinic and laboratory team members. The broadcasts were one hour long, with a text and phone dial in segments for listener engagement. These broadcasts were all live and recorded in both English and Chichewa. There was very high engagement from the listeners during the radio programmes. Similarly, a television programme was recorded with a live studio audience and aired twice in June 2022. The live audience engaged well with the study team and asked relevant questions.
Digital media: The study team recorded a video for MLW’s YouTube channel describing the importance of human infection studies in Africa and detailing the PCV13 trial. In addition, a digital study flyer was circulated on WhatsApp.
Increased visibility: The study team utilized branded clothing for participants and staff members to increase visibility and generate interest about the study.
Clinic recruitment: Recruitment to the pneumococcal CHIM study itself was as follows. Potential participants who showed interest were invited via telephone to an in-person information visit (visit A) to the research clinic. The information visits were conducted in groups and lasted approximately an hour. During this visit, A study nurse or clinician provided detailed information about the study including screening, vaccination, inoculation, quarantine, and safety procedures and follow up. Risks were discussed in detail. Materials used to collect samples were also demonstrated. At this stage, participants did not require to disclose whether they will join the study or not but were encouraged to think about it and to decide later. At the end of the visit, the potential participant’s information, including their name, contact number, age, sex, residence, and their information sources regarding the study were recorded. Information sources included college sensitization campaigns, snowballing, adverts, social media and digital programs on radio and television. In addition, information to define the participants’ community category was collected. They were defined as a college student or not a college student (referred to as ‘the community’).
During a second visit intended to obtain individual consent (visit B), data were collected to show how many participants from each category showed interest in joining the study and how many of each category were both eligible and were successfully recruited, consented and vaccinated.
Following screening and recruitment, participants underwent randomization, vaccination, inoculation and follow up including residential stay and exited the study. Study procedures are summarized in Figure 1.
Summary of recruitment and follow up procedures in the main trial; PCV13 trial.This figure is an original figure produced by the author(s) for this review article.
Ethical approvals
The CHIM study including recruitment strategies was approved in Malawi by the National Health Sciences Research Committee on 1 May 2020 (REF: 16/07/2519) and Pharmacy Medicines and Regulatory Authority (REF: PMRA/CTRC/III/10062020121) and in the United Kingdom by the Liverpool School of Tropical Medicine on 23 April 2021 (REF: 20-021). The trial was registered with the Pan African Clinical Trials Registry (REF: PACTR202008503507113) and can be found on https://pactr.samrc.ac.za/TrialDisplay.aspx?TrialID=12124.
Results
A total of 299 participants were screened for the study, of which 278 were recruited. 209 (69.9% and 195 (70.1%) of the screened and recruited volunteers, respectively, were males.
Screening and recruitment by recruitment strategy
Snowballing: 215 of 299 (71.9%) screened indicated that they were motivated to join through snowball recruitment. Of these, 201 were eventually enrolled in the study. 21 volunteers were excluded for not meeting one or more of the inclusion criteria ( Table 1).
Sensitization: 82 of 299 (21.4%) screened were motivated after a sensitization event ( Table 2a and Table 2b).
Radio and television: This strategy motivated only one individual to screen and enrol in the study ( Table 2a and Table 2b).
Poster: Only one individual was screened and enrolled after seeing a study poster ( Table 2a and Table 2b).
Participant feedback on exiting the PCV13 study
213 participants accepted to be interviewed regarding their experience in a CHIM at study exit. Responses were recorded using a Likert scale survey. The majority either strongly agreed or agreed that study processes from informed consent, through recruitment, safety monitoring, compensation and quarantine-were a positive experience. 95.3% stated that they would recommend study participation to a friend ( Table 3).
Discussion
In this article, we describe recruitment methods utilized in a pneumococcal human infection study. An overwhelming number of participants were recruited via snowballing or word of mouth networking.
This is the first study of its kind of which we are aware. The strengths of this study are that several institutions and potential volunteer groups were observed, and many methods of recruitment were attempted. The limitation is that not all of the recruitment processes and decision making can be observed.
We suggest that hearing about the study from a former or current volunteer may reinforce trust in the safety of the study in potential volunteers and encourage them to join. There has been evidence suggesting this in participant studies in Malawi and in Kenya ^ 9 ^.
On reflection, we consider that the tools used by the study team to inform and educate the community about the study may not have been well understood or accepted by the targeted audience and may need to be reviewed. While radio and television, done in both English and Chichewa, attracted an audience and active participation, this did not directly translate to an increased number of volunteers. The suitability of the messaging tools needs further exploration. Engaging former and current volunteers to participate in study sensitization activities may need to be considered.
Our study recruited more male than female volunteers. Possible reasons for this could be greater autonomy and decision-making power regarding consent to research participation among men than women in Malawi, although this was not formally explored in this study ^ 12 ^. Another reason could be that the information visits reached more men than women and via snowballing they predominantly enlisted their friends, mostly men too. Thirdly, if the study was viewed as risky, males may have had a greater risk tolerance. Targeting women through women church groups and community village banks might increase participation of women in CHIM studies in Malawi.
Conclusions
In conclusion, engaging current and former volunteers in novel trials like human infection studies is a possible strategy that can encourage community acceptance and participation in settings like Malawi. More work needs to be done to explore how increased participation from women can be ensured.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Morton B Burr S Chikaonda T : A feasibility study of controlled human infection with Streptococcus pneumoniae in Malawi. E Bio Medicine. 2021;72: 103579. 10.1016/j.ebiom.2021.103579 34571365 PMC 8479630 · doi ↗ · pubmed ↗
- 2Hodgson SH Juma E Salim A : Lessons learnt from the first controlled human malaria infection study conducted in Nairobi, Kenya. Malar J. 2015;14: 182. 10.1186/s 12936-015-0671-x 25927522 PMC 4416324 · doi ↗ · pubmed ↗
- 3A Study of Blood-stage Controlled Human Plasmodium Falciparum Malaria Infection in Tanzania. Accessed 06 April 2023. Reference Source
- 4Egesa M Ssali A Tumwesige E : Ethical and practical considerations arising from community consultation on implementing controlled human infection studies using Schistosoma mansoni in Uganda. Glob Bioeth. 2022;33(1):78–102. 10.1080/11287462.2022.2091503 35814190 PMC 9258062 · doi ↗ · pubmed ↗
- 5Chilengi R Simuyandi M Chibuye M : A pilot study on use of live attenuated rotavirus vaccine (Rotarix™) as an infection challenge model. Vaccine. 2020;38(46):7357–7362. 10.1016/j.vaccine.2020.09.023 33032844 · doi ↗ · pubmed ↗
- 6Morton B Burr S Jambo K : A pneumococcal controlled human infection model in Malawi: Transfer of an established pneumococcal carriage model from Liverpool, UK to Blantyre, Malawi – A feasibility study [version 2; peer review: 2 approved]. Wellcome Open Res. 2020;5:25. 10.12688/wellcomeopenres.15689.2 32399498 PMC 7194502 · doi ↗ · pubmed ↗
- 7Gordon SB Rylance J Luck A : A framework for Controlled Human Infection Model (CHIM) studies in Malawi: Report of a Wellcome Trust workshop on CHIM in Low Income Countries held in Blantyre, Malawi [version 1; peer review: 2 approved]. Wellcome Open Res. 2017;2:70. 10.12688/wellcomeopenres.12256.1 29018841 PMC 5627502 · doi ↗ · pubmed ↗
- 8Kapumba BM Jambo K Rylance J : Stakeholder views on the acceptability of human infection studies in Malawi. BMC Med Ethics. 2020;21(1): 14. 10.1186/s 12910-020-0454-y 32024497 PMC 7003337 · doi ↗ · pubmed ↗