Dysphagia following transcatheter mitral valve-in-ring replacement complicated by neo-left ventricular outflow tract obstruction: a case report
Stephanie Sargent, Eddy Xiong, Katherine Lau, Owen Christopher Raffel, Kim Greaves

TL;DR
A 77-year-old woman developed dysphagia after a heart valve procedure due to a rare complication involving blood vessel blockage and anemia.
Contribution
First reported case of TMVR causing reversible neo-LVOT obstruction leading to intravascular haemolysis and dysphagia.
Findings
Neo-LVOT obstruction after TMVR caused intravascular haemolysis and severe dysphagia.
Beta blocker therapy and volume resuscitation resolved the obstruction and reduced oesophageal spasm.
The case highlights a complex cycle of haemodynamic factors complicating management.
Abstract
Neo-left ventricular outflow tract (LVOT) obstruction is a dreaded complication following transcatheter mitral valve replacement (TMVR). Dynamic LVOT obstruction has been reported to cause mechanical intravascular haemolysis due to red cell fragmentation. Intravascular haemolysis can result in a rare but well-described phenomenon in which patients experience dysphagia due to oesophageal spasm. This phenomenon is classically associated with paroxysmal nocturnal haemoglobinuria and has never been reported following TMVR. A 77-year-old female presented 8 days following TMVR with presyncope, dyspnoea, and severe dysphagia. Transthoracic echocardiography revealed neo-LVOT obstruction with trivial paravalvular mitral regurgitation. Doppler echocardiography revealed dynamic late-peaking LVOT obstruction with a peak gradient of 71 mmHg with Valsalva manoeuvre. Laboratory investigations…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
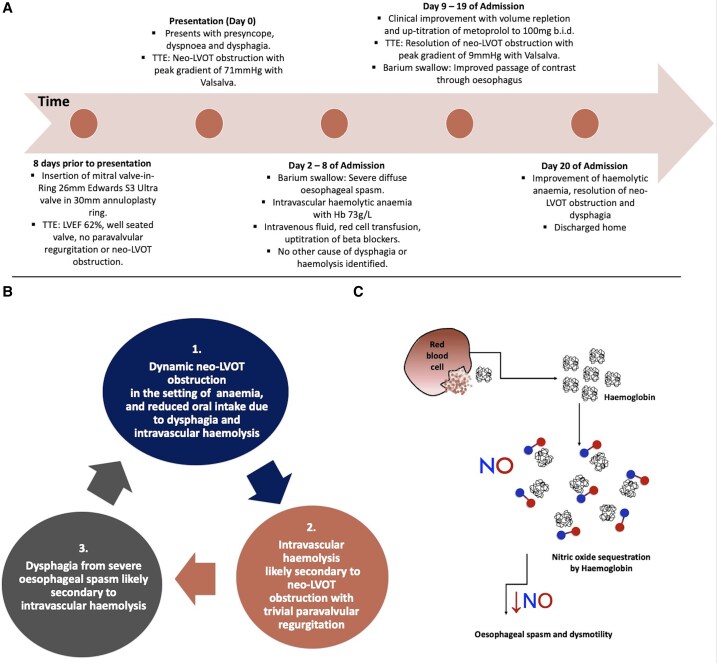 Figure 1
Figure 1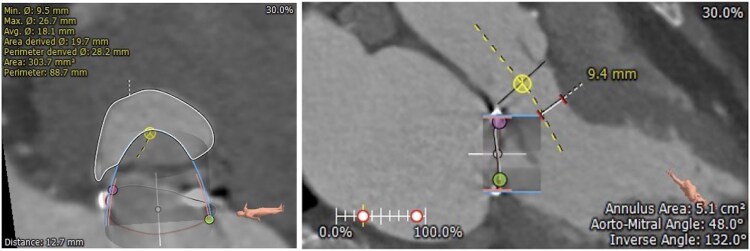 Figure 1
Figure 1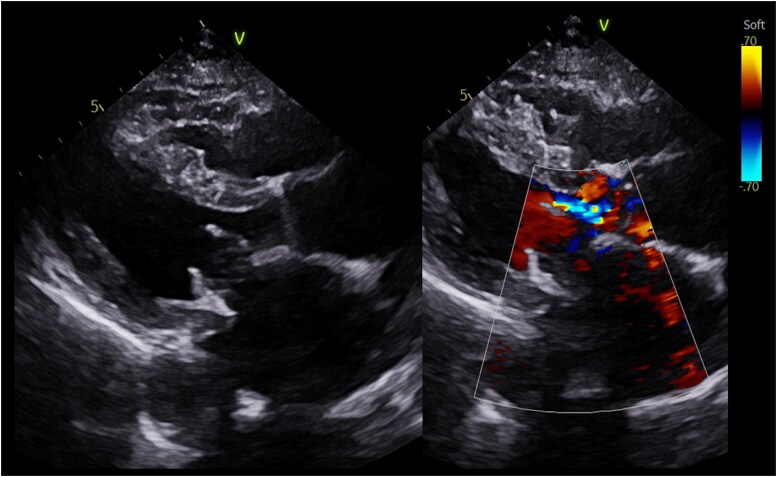 Figure 2
Figure 2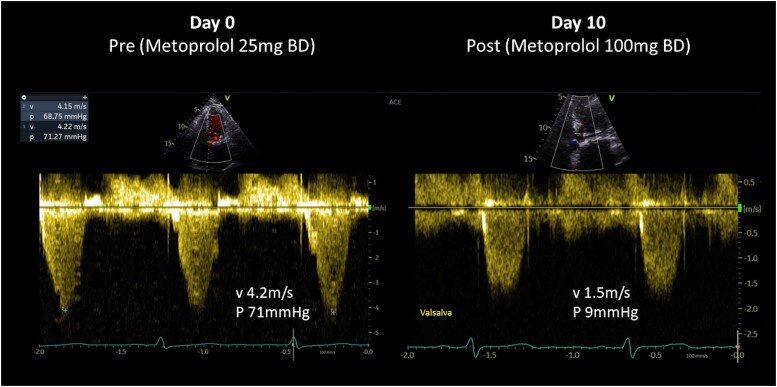 Figure 3
Figure 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCardiac Valve Diseases and Treatments · Cardiac Structural Anomalies and Repair · Infective Endocarditis Diagnosis and Management
Introduction
Transcatheter mitral valve replacement (TMVR) is an emerging minimally invasive strategy for the management of severe symptomatic mitral regurgitation in patients who are considered high surgical risk. Due to the complexity of the mitral valve apparatus and its proximity to the left ventricular outflow tract (LVOT), neo-LVOT obstruction is a dreaded complication of TMVR. Whilst pre-procedural planning with computerized tomography (CT) is an essential step in determining patient suitability for TMVR, there is a dynamic component to the development of LVOT obstruction which needs consideration.^1^
Dynamic LVOT obstruction is a well-known sequelae of hypertrophic cardiomyopathy, and can produce intravascular haemolysis due to increased velocity of blood flow across the LVOT resulting in red blood cell destruction.^2^ Intravascular haemolysis can lead to dysphagia due to oesophageal spasm as a result of nitric oxide sequestration by free haemoglobin. This is a well reported phenomenon in patients with paroxysmal nocturnal haemoglobinuria occurring in up to 51% of patients.^3^ The link between intravascular haemolysis and dysphagia in patients with cardiac conditions has only been reported in two published case reports, in patients with left ventricular assist devices.^4,5^
Intravascular haemolysis following TMVR has been reported in the setting of neo-LVOT obstruction and concurrent significant paravalvular leak. Whilst haemolytic anaemia is a known complication following TMVR, it is usually in the setting of significant paravalvular regurgitation. This is the first case report, to our knowledge to describe dynamic neo-LVOT obstruction following TMVR without significant paravalvular regurgitation resulting in intravascular haemolysis and dysphagia.
Summary figure
**
Case presentation
A 77-year-old female who had previously undergone mitral valve repair with a 30 mm annuloplasty ring and P2 neochordae for mitral valve prolapse presented with severe symptomatic mitral regurgitation. Her comorbidities included rheumatoid arthritis on sulfasalazine 500 mg twice daily, chronic kidney disease, and hypertension on perindopril 2.5 mg once daily. She was deemed too high risk for re-do sternotomy with a EuroSCORE II of 11% and subsequently underwent a trans-septal transcatheter mitral valve-in-ring (TMVinR) with implantation of a 26 mm Edwards S3 Ultra transcatheter heart valve. The preoperative CT deemed her anatomy appropriate for TMVinR with a CT neo-LVOT area of 303.7 mm^2^ and short anterior mitral valve leaflet (Figure 1). She was discharged Day 1 following a successful and uncomplicated procedure on metoprolol 25 mg twice daily, frusemide 40 mg daily, aspirin 100 mg daily, and warfarin. Her transthoracic echocardiogram prior to discharge demonstrated normal left ventricular function with an ejection fraction of 62%, a well-seated valve, trivial transvalvular regurgitation without paravalvular regurgitation or neo-LVOT obstruction.
Pre-procedural computed tomography evaluation of the risk of LVOT obstruction. Predicted Neo-LVOT area and aorto-mitral angle based on virtual deployment of a 26 mm Edwards Sapien S3 valve are shown. A neo-LVOT area of 303.7 mm2 (>200 mm2) and an aorto-mitral angle of 132° (>90°) indicate a low risk of LVOT obstruction.
Eight days following her discharge, she presented to the emergency department with dyspnoea, presyncope, and dysphagia. Physical examination revealed a blood pressure of 90/60 mmHg, heart rate of 96 b.p.m., intravascular depletion, and a late peaking ejection systolic murmur. Laboratory parameters showed a haemoglobin (Hb) of 81 g/L (reference range: 115–165 g/L), lactate dehydrogenase (LDH) 2711 U/L (reference range: 120–250 U/L), and bilirubin 29 μmol/L (reference range: <20 μmol/L). Her echocardiogram upon re-presentation demonstrated LVOT obstruction secondary to native anterior mitral leaflet displacement with a peak gradient of 71 mmHg with Valsalva and trivial paravalvular regurgitation (Figures 2 and 3 and Supplementary material online, Video S1). Metoprolol was up-titrated to 50 mg twice daily, perindopril was withheld, and intravenous fluid therapy was administered.
Echocardiography. Parasternal long axis demonstrating crowding of the LVOT with chordal SAM secondary to native anterior mitral valve leaflet. Flow acceleration within the LVOT secondary to Edwards S3 Ultra within 30 mm Physio ring (26 mm).
Continuous wave Doppler through the LVOT. Late peaking systolic signal suggestive of dynamic LVOT obstruction secondary to native mitral leaflets with a peak gradient 71 mmHg with Valsalva manoeuvre. Repeat echocardiography 10 days later showing an improvement in gradients across the LVOT with a peak gradient of 9 mmHg with Valsalva manoeuvre.
Two days into her admission, she developed an acute severe intravascular haemolytic anaemia with a Hb nadir of 73 g/L, LDH 4022 U/L, bilirubin 47 μmol/L, reticulocytes 277 × 10^9^/L (reference range: 20–120 × 10^9^/L), haptoglobin 0.01 g/L (reference range: 0.3–2.0 g/L), and schistocytes on blood film. Her dysphagia progressed and was unable to tolerate any oral intake. She required multiple blood transfusions, and intravenous fluid therapy was continued.
Haematology consultation was sought. Sulfasalazine was temporarily withheld as a potential drug-induced cause for haemolysis, however following haematology and immunology consultation, this was deemed an unlikely cause and sulfasalazine was re-commenced. After alternative causes for haemolysis were excluded including a CT neck to pelvis to investigate for possible malignancy, intravascular haemolysis was presumed secondary to cardiac pathology.
After seeking gastroenterology and speech pathology reviews, her dysphagia was investigated with a barium swallow which revealed diffuse oesophageal spasm (see Supplementary material online, Video S2A). She underwent an endoscopy which was normal. After excluding other causes for her dysphagia, a causal link between intravascular haemolysis and dysphagia was identified.
During her inpatient stay, beta blockers were up-titrated to maximally tolerated doses (metoprolol 100 mg twice daily). She had symptomatic improvement with resolution of dyspnoea, presyncope, and dysphagia. Her repeat echocardiogram prior to discharge demonstrated resolution of LVOT obstruction with a peak gradient with Valsalva of 9 mmHg (Figure 3, Supplementary material online, Video S3). A follow-up barium swallow revealed marked improvement in oesophageal spasm (see Supplementary material online, Video S2B). Her laboratory parameters improved with Hb 95 g/L, LDH 898 U/L, and bilirubin 7 μmol/L at discharge. Perindopril and frusemide were discontinued, and she was discharged on warfarin for three months post-procedure, metoprolol 100 mg twice daily, and sulfasalazine 500 mg twice daily.
Discussion
Mitral regurgitation is the most common valvular pathology worldwide, affecting an estimated 2% of the global population and ∼10% of patients over the age of 75 years.^6^ An estimated 50% of patients with mitral regurgitation are not suitable operative candidates which has led to the development of minimally invasive interventions, such as the TMVR.^7^
The risk of neo-LVOT obstruction following TMVR is ∼7%–9% and up to 12% for trans-septal TMVinR procedures. It is a feared complication which carries mortality risk.^1^ In contemporary clinical trials, ∼50% of patients have a threatened projected neo-LVOT on pre-procedural CT screening and therefore pre-procedural CT is considered a crucial step in appropriate procedural planning and success.^1,8^ Left ventricular outflow tract obstruction is a dynamic process which results in reduced cardiac output and occurs due to a complex interplay between anatomical factors and physiological status. Whilst, pre-procedural CT can accurately model the projected post-procedural neo-LVOT area and risk for LVOT obstruction, certain haemodynamic factors including heart rate, left ventricular contractility, and volume status which are less predictable with significant variability can influence the neo-LVOT and these factors need to be considered.^9^
Clinically relevant haemolysis with symptomatic anaemia is rare following TMVR with an estimated incidence of ∼3%.^10,11^ Intravascular haemolysis following TMVR is often a result of paravalvular regurgitation; however, it has been described once in the literature in the setting of neo-LVOT obstruction with concurrent significant paravalvular regurgitation.^9^ Haemolysis secondary to LVOT obstruction has also been reported in patients with hypertrophic obstructive cardiomyopathy due to the turbulence of high-velocity blood flow and subsequent shearing stress on red blood cells.^12^
Dysphagia secondary to intravascular haemolysis is well reported in patients with paroxysmal nocturnal haemoglobinuria; however, there are rare case reports of dysphagia secondary to intravascular haemolysis secondary to cardiac aetiology. There are currently two published case reports in the literature documenting the development of dysphagia secondary to intravascular haemolysis in patients with a left ventricular assistance device.^4,5^
This is a unique case for multiple reasons. Firstly, whilst intravascular haemolysis has been reported in the literature following TMVR with neo-LVOT obstruction, it is in the setting of significant paravalvular regurgitation. Our patient had only trivial paravalvular regurgitation, and it was postulated that the neo-LVOT obstruction was the most significant contributor to the development of intravascular haemolysis, similar to the pathophysiology responsible for LVOT obstruction in hypertrophic obstructive cardiomyopathy. Furthermore, dysphagia secondary to intravascular haemolysis has not been reported following TMVR. Whilst her presentation with dysphagia, neo-LVOT obstruction, and intravascular haemolysis was complex, the close relationship between these complications was successfully managed with simple fluid resuscitation, red blood cell transfusion, and up-titration of beta blocker therapy (Summary figure).
This case highlights several important complications following TMVR. Neo-LVOT obstruction is a relatively frequent complication of TMVR and whilst appropriate pre-procedural planning is an important factor in appropriate patient selection, haemodynamic factors are not always considered and may be difficult to predict. Whilst intravascular haemolysis following TMVR is rare, this case report highlights the complexity of managing patients with neo-LVOT obstruction with haemolysis and the complex interplay between certain haemodynamic factors. Dysphagia as a result of the intravascular haemolysis contributed to the vicious cycle of neo-LVOT obstruction and subsequent haemolysis.
Lead author biography
Dr Stephanie Sargent is a cardiologist currently undertaking a fellowship in echocardiography at The Prince Charles Hospital in Queensland, Australia. She completed an undergraduate degree in Biomedical Science at University of Sunshine Coast followed by the completion of Bachelor of Medicine/Surgery at James Cook University, Australia. She completed a Masters in Internal Medicine at the University of Sydney.
Supplementary Material
ytaf081_Supplementary_Data
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Reid A, Ben Zekry S, Turaga M, Tarazi S, Bax JJ, Wang DD, et al Neo-LVOT and transcatheter mitral valve replacement: expert recommendations. JACC Cardiovasc Imaging 2021;14:854–866.33248959 10.1016/j.jcmg.2020.09.027 · doi ↗ · pubmed ↗
- 2Lin Y, Yu L, Liu F, Lin X, Li H, Xu X. Relationship between left ventricular outflow tract pressure gradient and hemoglobin in patients with hypertrophic cardiomyopathy. Acta Cardiol Sin 2020;36:343–350.32675926 10.6515/ACS.202007_36(4).20191206 APMC 7355115 · doi ↗ · pubmed ↗
- 3Muñoz-Linares C, Ojeda E, Forés R, Pastrana M, Cabero M, Morillo D, et al Paroxysmal nocturnal hemoglobinuria: a single Spanish center’s experience over the last 40 yr. Eur J Haematol 2014;93:309–319.24758317 10.1111/ejh.12346 PMC 4232878 · doi ↗ · pubmed ↗
- 4Wuschek A, Iqbal S, Estep J, Quigley E, Richards D. Left ventricular assist device hemolysis leading to dysphagia. World J Gastroenterol 2015;21:5735–5738.25987800 10.3748/wjg.v 21.i 18.5735 PMC 4427699 · doi ↗ · pubmed ↗
- 5Mentz RJ, Schlendorf K, Hernandez AF, Milano CA, Felker GM, Blue LJ, et al Dysphagia in the setting of left ventricular assist device hemolysis. ASAIO J 2013;59:322–323.23644623 10.1097/MAT.0b 013e 31828 bbb 00PMC 4158398 · doi ↗ · pubmed ↗
- 6Kumar V, Yadav MS, Dhir S. Transcatheter mitral valve replacement (TMVR) for degenerated mitral valve bioprosthesis—a case series. IHJ Cardiovasc Case Rep 2023;7:68–71.
- 7Taha FA, Naeim H, Alnozha F, Amoudi O, Abuelatta R. Transcatheter mitral valve replacement in high-surgical risk patients: a single-center experience and outcome. J Interv Cardiol 2022;2022:6587036.35847236 10.1155/2022/6587036 PMC 9242753 · doi ↗ · pubmed ↗
- 8Ludwig S, Ruebsamen N, Deuschl F, Schofer N, Kalbacher D, Schaefer A, et al Screening for transcatheter mitral valve replacement: a decision tree algorithm. Euro Intervention 2020;16:251–258.32287036 10.4244/EIJ-D-19-01051 · doi ↗ · pubmed ↗