Duodenal Ulcer and Gastrointestinal Bleeding as a Late Complication of Over-The-Scope Clip Placement
Aditya Avula, Ahmed Al-Chalabi, Erin Jenkins

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
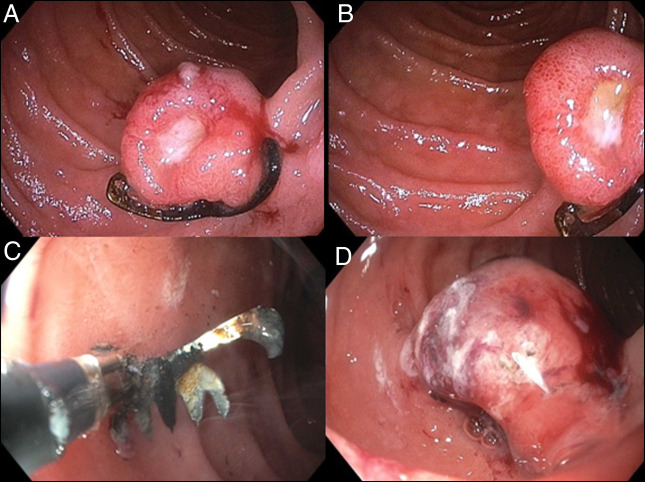 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCardiac Valve Diseases and Treatments · Shoulder and Clavicle Injuries · Shoulder Injury and Treatment
CASE REPORT
These images (Figure 1) are from a 70-year old man who presented with a 5-day history of melena and concomitant lightheadedness. Thirty-one months earlier, he experienced similar symptoms and was found to have a duodenal Dieulafoy lesion. This lesion was managed through the application of an over-the-scope clip (OTSC) (Ovesco Endoscopy USA), achieving hemostasis and subsequent clinical improvement.
(A and B) Retained OTSC from prior endoscopy found in the second portion of the duodenum that was found to be surrounding an oozing ulceration. This ulceration was determined to be the source of the patient's melena. (C) Bipolar cutting instrument (remOVE direct current Cutter) used to fragment the retained OTSC into 3 pieces. (D) Duodenal ulceration post-OTSC removal with residual oozing. OTSC, over-the-scope clip.
Endoscopy on this presentation revealed a 15 mm mucosal nodule with an oozing ulcer in the second portion of the duodenum. There was a foreign body at the base of the nodule consistent with a retained OTSC from previous endoscopy (Figure 1). Biopsies of the ulcer showed no evidence of malignancy. This ulceration was deemed to be the bleeding source, and repeat endoscopy was performed to remove the OTSC, which was fragmented into 3 pieces using a bipolar cutting instrument (remOVE direct current Cutter) and retrieved with grasping forceps (Figure 1). The patient's melena resolved shortly after this intervention.
While acute adverse events associated with OTSC implementation have been documented, prolonged complications have not been widely reported. This case illustrates the potential for chronic ulceration and subsequent hemorrhage in association with a retained OTSC, and the importance of familiarity with removal techniques.
DISCLOSURES
Author contributions: A. Avula and E. Jenkins: design of the work; acquisition, analysis, and interpretation of data for the work. A. Avula: drafting and reviewing intellectual content including formations of text and images; submission of final text and imagery. E. Jenkins: design of the work; acquisition of endoscopic images and initial endoscopy. A. Al-Chalabi: design of the work; initial endoscopy, improving text and images; draft revision, and review of final text and imagery. A. Avula is the article guarantor.
Financial disclosure: None to report.
Previous presentation: This case was presented at the American College of Gastroenterology (ACG) Annual Scientific Meeting and Postgraduate Course; October 27, 2024; Philadelphia, PA.
Informed consent was obtained for this case report.