Extended Approaches to the Maxillary Sinus are not Associated With an Increased Risk of Empty Nose Syndrome
Oloruntobi Rotimi, Isabelle Williams, Catherine Rennie, Saleh Okhovat, Rishi Sharma, Peter‐John Wormald, Neil C.‐W. Tan

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
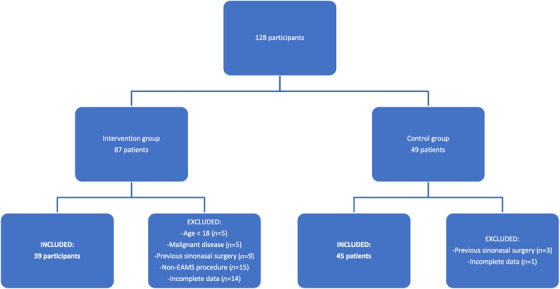 FIGURE 1
FIGURE 1| EAMS (intervention) | ESS (control) |
| |
|---|---|---|---|
| Gender |
22 Male 17 Female |
26 Male 19 Female |
|
| Median age ± SD | 60 ± 14.4 | 56 ± 16.5 |
|
| ENS6Q subscore | EAMS group | ESS group |
|
|---|---|---|---|
| Nasal dryness | 0.62 ± 1.09 | 0.64 ± 1.07 |
|
| Sensation of poor nasal airflow | 0.69 ± 1.32 | 1.11 ± 1.42 |
|
|
|
|
|
|
| Sensation of Nasal openness | 0.15 ± 0.71 | 0.24 ± 0.74 |
|
| Nasal crusting | 0.97 ± 1.22 | 0.24 ± 0.77 |
|
| Nasal burning | 0.15 ± 0.71 | 0.44 ± 1.16 |
|
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsSinusitis and nasal conditions · Head and Neck Surgical Oncology · Nasal Surgery and Airway Studies
Introduction
1
Empty nose syndrome (ENS) is a rare complication of sinonasal surgery which is characterized by the paradoxical sensation of nasal obstruction despite a widely patent nasal cavity [1, 2]. ENS is a debilitating condition that has negative physical and psychological impacts on quality of life [3]. Several studies found no significant association between turbinate resection and the development of ENS [4, 5]. Notably, there is a paucity of data examining the association between more extensive sinonasal surgery and ENS [6]. The study aims to assess the association between extended approach to the maxillary sinus procedures (EAMS) and ENS.
Summary
- Extended approaches to the maxillary sinus are not associated with an increased risk of Empty Nose Syndrome.
- No difference in the ENS6Q scores between turbinate sparing and turbinate sacrificing procedures.
Methods
2
A retrospective cohort compared the association of ENS in adult patients who have undergone EAMS against adult patients who underwent endoscopic sinus surgery (ESS) in four tertiary centers across the United Kingdom. Consecutive patients who underwent EAMS for benign sinonasal disease were included. Exclusion criteria included: pediatric patients, malignant disease, incomplete data, and previous sinonasal surgery. Control participants underwent ESS for chronic rhinosinusitis (CRS). EAMS and ESS groups were matched to minimize bias due to demographics. EAMS included radical medial maxillectomy (RMM), modified medial maxillectomy (MMM), or prelacrimal approach (PLA) [7] (Appendix S2). ESS was defined as full house ESS without formation of a mega‐antrostomy. Outcome measures were obtained during outpatient reviews. The primary measure was the 6—item empty nose syndrome questionnaire score (ENS6Q).
Mann–Whitney U test, Fischer exact test, and descriptive characteristics were conducted using IBM SPSS (Version 29.0.2.0). All tests were two‐tailed (significance threshold of 0.05).
Results
3
A total of 136 patients were screened for eligibility. Out of them, 84 patients were included in this study. The rationale for the excluded patients are displayed in Figure 1.
Flow diagram of study participants.
A total of 39 patients underwent EAMS (23 RMM; 16 MMM/PLA) and 45 patients underwent ESS. The EAMS and ESS groups were matched for gender and age as shown in Table 1.
87% of patients in the EAMS group (n = 34) underwent surgery for inverted papilloma with no evidence of atypia or malignant transformation on histology. The remaining five patients underwent surgery for benign vascular lesions. The patients in the ESS group underwent surgery for refractory CRS to appropriate medical therapy.
There was no statistically significant difference in mean ENS6Q scores in patients who underwent EAMS compared with ESS (2.77 ± 3.94 vs. 3.27 ± 4.29, p = 0.65). There was no statistically significant difference in ENS6Q scores in patients who underwent turbinate preserving procedures (e.g., MMM/PLA) compared with turbinate sacrificing procedures (e.g., RMM) (2.57 ± 3.46 vs. 3.06 ± 4.64, p = 0.81). There was a statistically significant difference in nasal suffocation subscore between the EAMS group and ESS group (nasal suffocation, p = 0.009). There were no statistically significant differences in the remaining ENS6Q subscores between the EAMS group and the ESS group, as shown in Table 2.
Discussion
4
This study was unable to identify any significant association between EAMS procedures and increased total ENS6Q scores. There were also no significant differences in ENS6Q between patients undergoing EAMS procedures and patients undergoing ESS. This suggests there is no additional risk of developing ENS when comparing patients undergoing EAMS with those undergoing ESS. There was no evidence for an additional risk of developing ENS when comparing turbinate sacrificing surgery turbinate sparing procedures, which is consistent with the findings in existing literature [4, 5]. Patients undergoing EAMS experienced less nasal suffocation than those undergoing ESS. Although this was statistically significant, this is unlikely to be clinically significant as the subscores were less than 1.
The evidence refuting altered turbinate morphology as a cause of ENS is mounting and suggests other mechanisms may be present as predisposing factors in the pathogenesis of this condition, that is, altered nasal airflow dynamics, disrupted nasal mucosal function, and impaired neurosensory mechanisms [8, 9]. Li et al. [9] assessed nasal airflow using computational fluid dynamics in ENS patients and found that nasal airflow was disproportionately directed to the middle meatus compared with controls (56.2 ± 14.7% of total flow). Nasal mucosa contains receptors that detect cool airflow to trigger nasal heating and humidification [8]. Disruption of nasal humidification impacts on the laminar nasal airflow and encourages crust formation which can subsequently alter neurosensory mechanisms [8]. These preexisting factors may predispose certain individuals to developing ENS following turbinate resection.
This is the first study of its kind to explore the association between ENS and EAMS procedures, laying the groundwork for further experimental research. The authors adopted a multicenter approach which enhanced the external validity of the findings and minimized recruitment bias, while the matching of patient demographics helped to minimize confounding variables.
Limitations include a small sample size and the retrospective design of the study. Furthermore, the observational nature of this study does not demonstrate temporality therefore causation cannot be easily inferred. Last, the control participants were obtained from a single center, limiting generalizability (Appendix S1).
The authors recommend further research with diagnostic studies to reliably identify predisposing factors for ENS. This would aid clinical decision‐making in terms of patient selection preoperatively and the extent of resection intraoperatively, ultimately reducing the incidence of patients with post‐operative ENS symptoms.
Conflicts of Interest
The authors declare no conflicts of interest.
Supporting information
Supporting Information
Supporting Information
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1M. O. Scheithauer , “Surgery of the Turbinates and “Empty Nose” Syndrome,” GMS Current Topics in Otorhinolaryngology ‐ Head and Neck Surgery 9 (2010): Doc 03, 10.3205/CTO 000067.22073107 PMC 3199827 · doi ↗ · pubmed ↗
- 2E. C. Kuan , J. D. Suh , and M. B. Wang , “Empty Nose Syndrome,” Current Allergy and Asthma Reports 15, no. 1 (2015): 1–5, 10.1007/S 11882-014-0493-X/FIGURES/1.25430954 · doi ↗ · pubmed ↗
- 3J. Manji , J. V. Nayak , and A. Thamboo , “The Functional and Psychological Burden of Empty Nose Syndrome,” International Forum of Allergy & Rhinology 8, no. 6 (2018): 707–712, 10.1002/ALR.22097.29443458 · doi ↗ · pubmed ↗
- 4H. R. Hong and Y. J. Jang , “Correlation Between Remnant Inferior Turbinate Volume and Symptom Severity of Empty Nose Syndrome,” Laryngoscope 126, no. 6 (2016): 1290–1295, 10.1002/LARY.25830.26692010 · doi ↗ · pubmed ↗
- 5N. C. W. Tan , R. Goggin , A. J. Psaltis , and P. J. Wormald , “Partial Resection of the Middle Turbinate During Endoscopic Sinus Surgery for Chronic Rhinosinusitis Does Not Lead to an Increased Risk of Empty Nose Syndrome: A Cohort Study of a Tertiary Practice,” International Forum of Allergy & Rhinology 8, no. 8 (2018): 959–963, 10.1002/ALR.22127.29633570 · doi ↗ · pubmed ↗
- 6K. Wada , T. Ishigaki , Y. Ida , Y. Yamada , S. Hosono , and H. Edamatsu , “Endoscopic Modified Medial Maxillectomy for Resection of an Inverted Papilloma Originating From the Entire Circumference of the Maxillary Sinus,” Case Reports in Otolaryngology 2015, no. 1 (2015): 952923, 10.1155/2015/952923.26146581 PMC 4469785 · doi ↗ · pubmed ↗
- 7A. Ashman , A. J. Psaltis , P. J. Wormald , and N. C. W. Tan , “Extended Endoscopic Approaches to the Maxillary Sinus,” Journal of Laryngology and Otology 134, no. 6 (2020): 473–480, 10.1017/S 0022215120000882.32508301 · doi ↗ · pubmed ↗
- 8A. S. Gill , M. Said , T. T. Tollefson , and T. O. Steele , “Update on Empty Nose Syndrome: Disease Mechanisms, Diagnostic Tools, and Treatment Strategies,” Current Opinion in Otolaryngology & Head and Neck Surgery 27, no. 4 (2019): 237–242, 10.1097/MOO.0000000000000544.31116142 · doi ↗ · pubmed ↗