Effects of Cigarette Smoking and 3‐Day Smoking Abstinence on Translocator Protein 18 kDa Availability: A [18F]FEPPA Positron Emission Tomography Study
Arthur L. Brody, Andre Y. Sanavi, Renee Beverly‐Aylwin, Natalie Guggino, Anna K. Mischel, Alvin Wong, Ji Hye Bahn, Mark G. Myers, Brinda Rana, David Vera, Kishore K. Kotta, Jeffrey H. Meyer, Jared W. Young, Carl K. Hoh

TL;DR
Smoking lowers brain levels of a marker linked to brain cell stress, but this effect reverses after just three days of not smoking.
Contribution
This study shows that short-term smoking abstinence normalizes a brain marker of gliosis previously suppressed by smoking.
Findings
Smokers who smoked before scanning had 15.3% lower brain marker levels than nonsmokers.
Three-day abstinence normalized the brain marker to nonsmoker levels.
Higher marker levels in abstinent smokers correlated with worse mood ratings.
Abstract
With the many negative health consequences of cigarette smoking, quitting is known to improve health in multiple domains. Using positron emission tomography/computed tomography (PET/CT) scanning, our group previously demonstrated that smokers have lower levels than nonsmokers of translocator protein binding both acutely and following overnight abstinence. Here, we sought to determine the effects of longer smoking abstinence on this marker of gliosis for microglia and astroglia, as well as explore associations between the marker and smoking‐related symptoms. This observational study was performed in an academic VA medical centre. Fifty‐nine generally healthy Veterans who were either nonsmokers (n = 15) or smokers (n = 44) participated in the study. Participants completed an intake visit to evaluate for inclusion/exclusion criteria, [18F]FEPPA PET/CT scanning and a structural magnetic…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
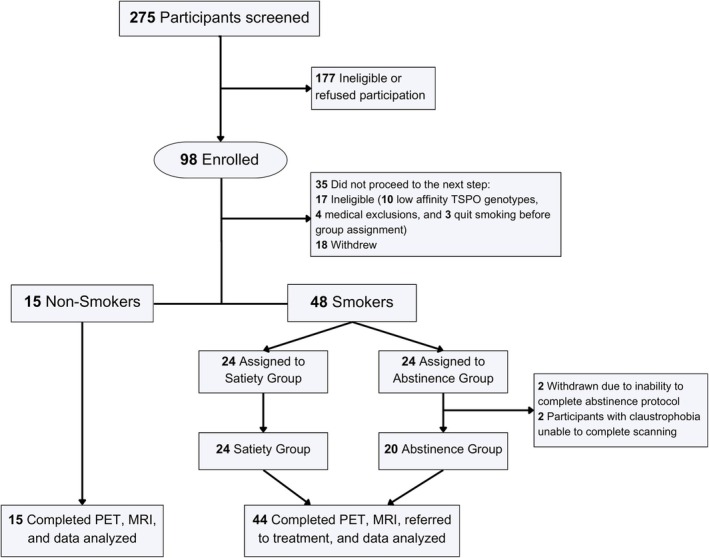 FIGURE 1
FIGURE 1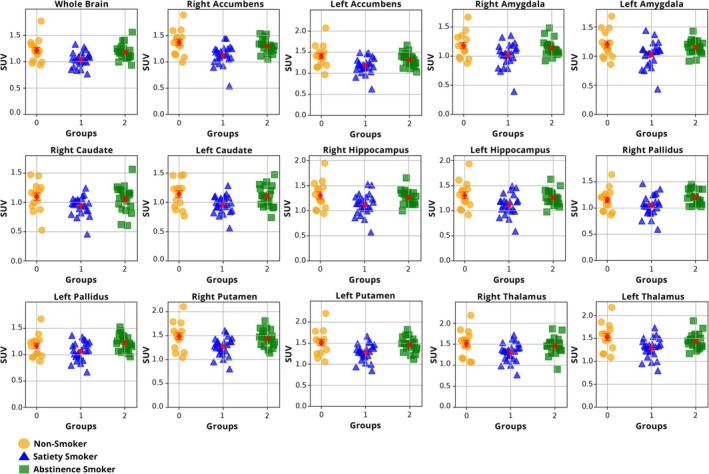 FIGURE 2
FIGURE 2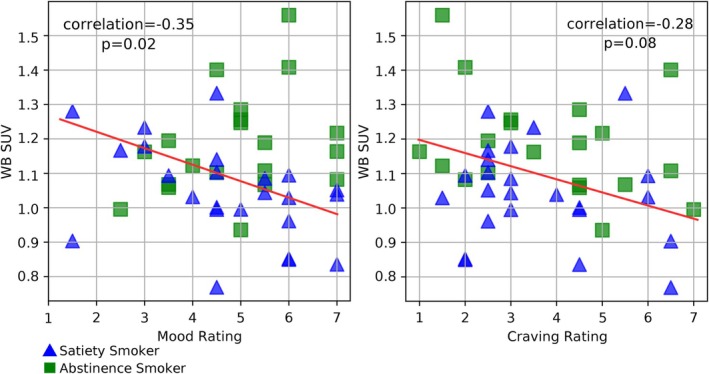 FIGURE 3
FIGURE 3| Variable | Nonsmokers ( | Smoker satiety ( | Smoker abstinent ( |
|---|---|---|---|
| Demographic | |||
| Age | 55.8 (± 13.4) | 54.2 (± 11.2) | 54.6 (± 12.4) |
| Sex (% female) | 26.7 | 16.7 | 20.0 |
| Race (%) | |||
| Asian/PI | 13.3 | 16.7 | 20.0 |
| Black | 26.7 | 25.0 | 10.0 |
| White | 53.3 | 50.0 | 60.0 |
| > 1 or other | 0 | 8.3 | 10.0 |
| Ethnicity (%Hispanic) | 0 | 8.3 | 10.0 |
| Education (years) | 14.9 (± 2.5) | 14.6 (± 2.4) | 14.2 (± 1.8) |
| Health‐related | |||
| Height (centimetres) | 171.5 (± 8.7) | 172.6 (± 8.8) | 175.5 (± 7.5) |
| Weight (kilograms) | 86.1 (± 13.8) | 85.3 (± 16.6) | 91.2 (± 17.7) |
| Body mass index | 29.3 (± 4.7) | 28.7 (± 5.8) | 29.5 (± 5.1) |
| Alcohol drinks/week | 2.0 (± 3.8) | 2.7 (± 4.1) | 3.5 (± 6.0) |
| TSPO (% high affinity genotype) | 66.7 | 66.7 | 70.0 |
| Smoking‐related (baseline) | |||
| Cigarettes per day | n/a | 16.5 (± 7.4) | 16.1 (± 7.5) |
| Pack‐year smoking history | n/a | 28.7 (± 21.4) | 30.3 (± 24.5) |
| Menthol cigarette smokers (%) | n/a | 37.5 | 30.0 |
| FTND | n/a | 4.2 (± 2.7) | 4.3 (± 1.8) |
| Smoking‐related (PET/CT scan) | |||
| MNWS | n/a | 15.2 (± 9.7) | 15.0 (± 9.0) |
| Craving (analogue) | n/a | 3.6 (± 1.6) | 3.8 (± 1.8) |
| Anxiety (analogue) | n/a | 2.6 (± 1.3) | 2.7 (± 1.1) |
| Mood (analogue) | n/a | 4.7 (± 1.6) | 4.9 (± 1.3) |
| Exhaled CO (ppm) | 1.9 (± 0.7) | 17.0 (± 10.1)*** | 2.1 (± 1.0) |
| Brain region | Nonsmoker group ( | Smoker satiety group ( | Smoker abstinence group ( |
| |
|---|---|---|---|---|---|
| Whole brain | 1.22 (± 0.21) | 1.04 (± 0.14) | 1.18 (± 0.15) | 0.003 | |
| Accumbens | R | 1.37 (± 0.23) | 1.13 (± 0.19) | 1.30 (± 0.13) | <0.001 |
| L | 1.40 (± 0.27) | 1.18 (± 0.20) | 1.32 (± 0.16) | 0.005 | |
| Amygdala | R | 1.18 (± 0.21) | 1.01 (± 0.21) | 1.14 (± 0.14) | 0.02 |
| L | 1.20 (± 0.23) | 1.03 (± 0.21) | 1.15 (± 0.12) | 0.02 | |
| Caudate | R | 1.10 (± 0.24) | 0.94 (± 0.16) | 1.06 (± 0.23) | 0.06 |
| L | 1.14 (± 0.23) | 0.97 (± 0.15) | 1.11 (± 0.18) | 0.01 | |
| Globus Pallidus | R | 1.16 (± 0.21) | 1.05 (± 0.20) | 1.20 (± 0.14) | 0.02 |
| L | 1.17 (± 0.21) | 1.07 (± 0.18) | 1.22 (± 0.15) | 0.02 | |
| Hippocampus | R | 1.31 (± 0.27) | 1.12 (± 0.21) | 1.27 (± 0.15) | 0.02 |
| L | 1.31 (± 0.26) | 1.12 (± 0.21) | 1.26 (± 0.15) | 0.02 | |
| Putamen | R | 1.49 (± 0.28) | 1.27 (± 0.19) | 1.44 (± 0.17) | 0.004 |
| L | 1.51 (± 0.29) | 1.28 (± 0.20) | 1.46 (± 0.18) | 0.003 | |
| Thalamus | R | 1.51 (± 0.31) | 1.31 (± 0.22) | 1.46 (± 0.21) | 0.02 |
| L | 1.53 (± 0.29) | 1.29 (± 0.22) | 1.44 (± 0.17) | 0.005 | |
- —National Institute on Drug Abuse 10.13039/100000026
- —Tobacco‐Related Disease Research Program 10.13039/100005188
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsNeuroinflammation and Neurodegeneration Mechanisms · Smoking Behavior and Cessation · Tryptophan and brain disorders
Introduction
1
Chronic cigarette smoking (CS) is associated with many negative health outcomes [1], including immune system–related illnesses, cancer, cardiovascular disease, lung disease, diabetes [2, 3] and impaired wound healing [4, 5]. When cigarette smokers quit and maintain abstinence, positive health changes begin to occur within minutes and the elevated risks of diseases and other detrimental effects decline over time [2, 3]. A specific effect of CS that likely contributes to some of the health consequences listed above is abnormal inflammatory function.
When functioning normally, neuroinflammation has the positive effects of tissue repair in response to central nervous system (CNS) injury, enhanced plasticity and neuroprotection [6, 7]. In contrast, abnormally low levels of neuroinflammation impair response to CNS injury and can lead to cognitive impairment [6], while abnormally high levels of neuroinflammation are associated with neurological illnesses (e.g., Alzheimer's disease, Parkinson's disease and amyotrophic lateral sclerosis) [7, 8]. Put simply, dysfunction of normal neuroinflammatory processes (either decreased or increased) is a health risk. Therefore, it is important to characterize the impact of CS on neuroinflammation, as it can have significant implications for brain health and cognitive function.
Because of the role of neuroinflammation in disease processes, much research has focused on the development of positron emission tomography (PET) radioligands for measuring markers of neuroinflammatory change. In this context, the translocator protein 18 kDa (TSPO) has been a molecule of interest because it is located in the mitochondrial membrane of microglia [7], microglia are the main resident immune cells of the CNS [9, 10, 11] and TSPO expression increases when microglia are activated [10, 12]. Furthermore, TSPO levels are elevated in conditions and illnesses in which microglia and astroglia are activated or changing toward an activated state [7, 10, 11, 13, 14, 15]. While TSPO is associated with microglial and, to a lesser extent, astroglial activation, it has incomplete cellular specificity and may be present in other cells, such as endothelial and infiltrating peripheral inflammatory cells [7, 14].
For the study presented here, ^18^F‐labelled fluoroethoxybenzyl‐N‐(4‐phenoxypyridin‐3‐yl) acetamide ([^18^F]FEPPA) was used with PET scanning, as it labels TSPO reliably [16] with high affinity [17, 18] and therefore has sensitivity to account for small between‐group differences [16, 17, 18, 19] and genetic TSPO predispositions [20]. Prior studies using [^18^F]FEPPA PET scanning include ones examining healthy populations [21, 22, 23], psychotic disorders [24, 25], Parkinson's disease [26, 27], major depressive disorder [28, 29] and cognitive impairment [30, 31].
Recent literature reviews of preclinical research [32, 33, 34] conclude that nicotine has more anti‐ than pro‐inflammatory effects, including overall anti‐inflammatory effects on pathways including microglia. These reviews report that nicotine binding to α7 nicotinic acetylcholine receptors (nAChRs) on microglia triggers an anti‐inflammatory cascade that alters microglial polarization and activity, cytokine release and intracellular calcium concentrations, leading to neuroprotection. However, while most studies report anti‐inflammatory properties of nicotine, evidence of increased neuroinflammation with CS exposure [35, 36] and nicotine administration [36] has also been reported. Thus, the complete pathway of nicotine's effects has not been fully elucidated, likely because neuroinflammation is a complex process resulting from multiple genes and signalling pathways.
As for studies of human CS, two prior studies by our group demonstrate that cigarette smokers have low levels of TSPO binding compared with nonsmokers. In the first of these studies [37], a second‐generation PET radioligand for TSPO ([^11^C]DAA1106) was used to examine effects of acute CS on TSPO availability. Based on the studies cited above, we had hypothesized that smokers would have abnormally low binding of [^11^C]DAA1106 on PET scanning, indicating less gliosis and that effects would occur globally throughout the brain, since prior research demonstrates widespread effects of CS when studying systems (e.g., the nAChR system) distributed throughout the brain [38, 39, 40, 41, 42]. The central finding of this study was that the PET outcome measure (whole brain [WB] standardized uptake value [SUV]) was significantly lower (mean—16.8%) in smokers who smoked to satiety immediately before scanning than in nonsmokers. Consistent with this global finding, analysis of smaller subcortical volumes of interest (VOIs) revealed a that all VOIs had a significant between‐group effect, due to smokers having lower SUVs than nonsmokers (14.6% to 19.7%). In the second study [43], we examined smokers who maintained abstinence overnight and the effect of this abstinence on TSPO availability. Smokers and nonsmokers underwent the same procedures as in the preceding study, with the exception being that smokers initiated abstinence prior to midnight on the night before the [^11^C]DAA1106 PET session (verified by an exhaled carbon monoxide [CO] level ≤ 4 ppm). The central study finding was that overnight abstinent smokers had significantly lower mean WB SUVs (by roughly 16.3%) than nonsmokers. Also, smaller VOIs had significant between‐group effects (p values < 0.0005 to 0.03), with abstinent smokers having lower SUVs in all VOIs. Taken together, these studies indicate that gliosis is reduced with acute smoking and this reduction persists through overnight abstinence.
Here, we sought to determine if a longer period of smoking abstinence would result in normal levels of TSPO binding. Because nicotine, a primary addictive constituent of tobacco smoke, has a half‐life of about 2–3 h [44] and its major metabolite (cotinine) [45, 46] and the combination of all its major metabolites [47] have half‐lives of approximately 16–19 h, we hypothesized that smokers abstinent for 3 days would have levels of the PET marker for gliosis similar to nonsmokers. In addition, because prior research found associations between the PET marker for gliosis and smoking withdrawal symptoms [37] (and depression [48]), we conducted an exploratory analysis examining associations between the marker for gliosis and withdrawal symptoms at the time of PET/CT scanning.
Methods
2
Fifty‐nine generally healthy adult Veterans (n = 15 nonsmokers and n = 44 smokers) completed the study and had usable data. Participants underwent the following study procedures (described in more detail below): telephone screening, in‐person intake visit, a satiety or 3‐day smoking abstinence protocol prior to PET/computed tomography (CT) scanning for participants who were smokers (alternate assignment), an [^18^F]FEPPA PET/CT scan, a structural magnetic resonance imaging (MRI) scan and (for smokers) referral to smoking cessation treatment. The study was approved by the IRB at the VA San Diego Healthcare System (#1204452). An additional four cigarette smokers were enrolled and assigned to the abstinence protocol, but two did not complete it and two started PET/CT scanning but were unable to complete it due to claustrophobia (Figure 1).
Consort diagram showing flow of participants through the study.
At the intake visit, participants were evaluated to determine if they met inclusion/exclusion criteria. Inclusion criteria were (1) adult Veterans (18–75 years old) who were daily cigarette smokers meeting criteria for tobacco use disorder [49] and interested in attempting to quit or nonsmokers (never users or > 1 year tobacco free); (2) ability to read, write and provide informed consent; and (3) smoking status confirmed by exhaled CO levels (≥ 8 ppm for smokers, < 8 ppm for nonsmokers). Exclusion criteria were (1) any acute psychiatric diagnosis (including mood, anxiety, psychotic and substance use disorders) within the past year; occasional drug/alcohol use not meeting criteria for abuse/dependence was not exclusionary, but participants were instructed to abstain from use for > 48 h prior to PET/CT scanning; (2) history of conditions that could affect the CNS at the time of scanning (e.g., history of severe head trauma, epilepsy, or other neurological diseases); (3) daily use of anti‐inflammatory medications; (4) unstable cardiovascular, liver or renal disease, which might make tolerating procedures difficult; (5) low affinity TSPO genotype; and (6) pregnancy, due to the theoretical risk of radiation exposure to the foetus.
During the intake visit, medical records were reviewed, and rating scales were administered to confirm eligibility and collect basic background and symptom information. Rating scales included the smoker's profile form [38] (demographic, race/ethnicity, educational level, medications, smoking history and other information) and Fagerström Test for Nicotine Dependence [50, 51] (FTND; severity of nicotine dependence). Because prior research demonstrates that genotyping can determine an individual's TSPO affinity subtype (high, medium or low), and these affinities affect binding for radioligands determining TSPO availability [20, 52], a saliva sample was also collected at the intake visit for genotyping of rs6971 within the TSPO gene. Using this sample, DNA was extracted from buccal cells using the Oragene OG‐500 kit (DNA Genotek; Ottawa, Ontario, Canada) according to manufacturer protocol. Genotyping of rs6971 within the TSPO gene was performed by polymerase chain amplification (Forward Primer: 5′‐AAGCGTGACGGCCACCACATCA‐3′; Reverse Primer: 5′‐CCTGACTCCCAAATCCAGTG‐3′) of a 362 base pair fragment of the TSPO gene containing the rs6917 followed by restriction enzyme digestion with NruI (New England Biolabs; Ipswich, MA) in the laboratory of a study co‐investigator (B.R.). Only participants with the high or medium affinity genotypes (> 90% of North Americans [22]) were included in PET/CT data analysis to avoid a potential confound.
After the intake visit, participants who were smokers were alternately assigned to either the satiety group or the abstinence group. Smokers assigned to the satiety condition were instructed to smoke as per their usual habit until the day of PET/CT scanning. Smokers assigned to the abstinence condition were instructed to stop smoking or using any nicotine containing products three nights prior to PET/CT scanning. Participants assigned to this condition met with study personnel and had abstinence checks 2 days, 1 day and the day of PET/CT scanning where they were required to report continuous abstinence from smoking and use of nicotine‐containing products and have exhaled CO levels ≤ 8 ppm for the 2 days prior visit and ≤ 4 ppm for the day before and day of PET/CT scanning visits in order to continue to scanning. Contingency management (CM) was used to encourage smoking abstinence, with the following protocol: 30 for two nights of abstinence and an additional $120 for all three nights of abstinence. Participants in the CM group were told whether or not they would be receiving the extra payments at each abstinence check visit. All participants received compensation for study assessments and were paid by check or bank transfer after study completion.
On the PET/CT scanning day, participants arrived at the VA San Diego PET/CT Center at midday. State rating scales were obtained, including the Minnesota Nicotine Withdrawal Scale (MNWS) [53] and analogue scales for craving, mood and anxiety. The MNWS‐revised comprehensively assessed cigarette withdrawal symptoms (including irritability, anxiety, depression and craving). Analogue ratings of craving, mood and anxiety were single items ranked from 1 to 7 (none to extremely strong [craving and anxiety] or very bad to very good [mood]). Following rating scale administration, both a breathalyser (AlcoMatePro) and urine toxicology screen (Test Country I‐Cup Urine Toxicology Kit) were obtained. Given that roughly 18% of American adults use marijuana [54], CS and marijuana use are highly comorbid [55] and urine toxicology screens may remain positive for 3–7 days for marijuana with a single use [56], participants were not excluded for a positive urine toxicology screen for marijuana or other recreational drugs, but were instructed to abstain for at least 48 h prior to PET/CT scanning and verbally confirmed this point at the testing session. Height and body weight were obtained for all all participants, and a urine pregnancy test (β‐HCG) (Test Country Cassette Urine Pregnancy Test) was obtained for female participants of childbearing potential were also obtained.
Following the above tests (which took approximately 1–2 h to complete), participants had an intravenous line placed by a nuclear medicine technician in a room adjacent to the PET/CT scanner. Participants who were smokers in the satiety group were taken to an outdoor area 10 min prior to scanning and smoked to satiety (18 of 24 smokers smoked one cigarette [range 0.75 to 3 cigarettes]), while smokers in the abstinence group and nonsmokers did not smoke prior to scanning. Immediately prior to PET/CT scanning (after smoking to satiety for the smoker satiety group), an exhaled CO level was measured with the Micro+ Smokerlyzer Breath CO Monitor (Bedfont Scientific, Ltd, UK), with CO levels of ≥ 8 ppm considered to be consistent with recent smoking and levels ≤ 4 ppm considered consistent with nonsmoking status. Participants were then positioned on the PET/CT scanner and received a bolus injection of ~185 MBq of [^18^F]FEPPA, followed by a dynamic PET scan of the brain for 90 min. PET/CT scans were obtained on a Siemens Biograph mCT Flow PET/CT scanner (Siemens Healthcare, Erlangen, Germany) in 3D mode. Scans contained 64 transaxial slices with a 500‐mm field of view and a 5‐mm in‐plane spatial resolution (FWHM). Study investigators obtained an investigational new drug approval from the FDA (IND 141607) for the use of [^18^F]FEPPA here, and it was produced using an established method [57, 58]. Following the PET/CT scan, state rating scales (MNWS and analogue craving, anxiety and mood) were again administered.
A structural MRI scan of the brain was obtained within a few weeks of PET/CT scanning and co‐registered with the PET/CT scans to aid in localization of anatomical regions. Structural MRI scans were obtained on a Siemens 3T Skyra Fit using a 3D T1 MPRAGE sequence with FOV = 220 mm, TR = 2300, TE = 2.99 ms, flip angle = 9°, slice thickness = 1.2 and scan time = 5:06. Total MRI scanning time was < 20 min.
Similar to previous research by our group [37, 38, 39, 43, 59, 60, 61, 62], PET‐to‐MRI co‐registration was performed using the PMOD quantitative parametric mapping software (Bruker, U.S.), and automated VOIs were determined on MRI and transferred to co‐registered PET/CT scans. The primary VOI was WB determined with FSL FAST for reasons cited above. Since regional differences were possible, VOIs were also determined for the amygdala, caudate, globus pallidus, hippocampus, nucleus accumbens, putamen and thalamus, similar to prior research [63, 64].
To obtain a quantitative measurement of VOI binding of TSPO in brain, SUVs were the primary outcome measure and were calculated using the standard definition: SUV = mean tissue activity concentration (Bq/mL)/(injected dose [Bq]/body weight [g]). Mean tissue activity concentration from 18.5 to 80 min post‐injection was used, based on time activity curves from this line of research demonstrating relatively stable radioligand levels during this period. SUV was used as the primary outcome measure because it avoids invasive arterial blood sampling and this method was not feasible at our facility. It is also noted that SUV has been shown to strongly correlate with total volume of distribution (Vt) values [65, 66], has good test–retest reproducibility [66] and has less intersubject variability than that for Vt [65] in studies using similar radioligands. Following the PET/CT session, smokers were referred to a standard 12‐week smoking cessation program at the VA San Diego Healthcare System.
Statistical analyses were performed on PET/CT outcomes to test study hypotheses using the SPSS version 29.0 (SPSS Inc., Chicago, IL). For baseline variables, groups were compared with chi‐square (for categorical variables) and t‐tests (for continuous variables). For PET/CT data, study groups were compared with an overall analysis of variance (ANOVA), with WB SUV as the dependent variable, group (nonsmoker, satiety smoker and abstinent smoker) as the between‐subject factor, and genotype as a nuisance covariate. For completeness, statistical analyses with the same structure were performed for the smaller subcortical VOIs. In addition to the primary study analysis, an exploratory analysis was performed including all smokers to determine partial correlations (controlling for TSPO genotype and smoking group [satiety or abstinence]) between PET/CT WB SUVs and mean values from the MNWS and craving, mood and anxiety scales. Alpha was set to p < 0.05.
Results
3
Study groups were well‐matched for baseline variables (Table 1) with no significant differences in age, sex, race, ethnicity, education (years), height, weight, body mass index (BMI), alcohol drinks per week, or TSPO affinity genotype (p = 0.30–0.98). The two smoker groups did not differ at baseline in number of cigarettes smoked per day, pack‐year smoking history, percentage of menthol cigarette smokers or FTND scores (p = 0.60–0.90).
At the PET/CT scanning visit, all alcohol breathalyser and urine pregnancy tests were negative. All participants reported no drug use (including marijuana) for 48 h prior to PET/CT scanning; however, a small number of participants had urine toxicology screens that were positive for THC (n = 0, 3 and 2 for the nonsmoker, satiety smoker and abstinent smoker groups, respectively). Smoking symptom rating scales obtained at the PET/CT session were not significantly different between the two smoker groups (Student t‐tests, p = 0.63–0.93 for the MNWS and analogue rating scales; Table 1), which was likely due to scales being administered prior to and after the PET/CT scan (roughly 1 and 3 h after arriving for the study visit), such that both groups had moderate withdrawal symptoms. As expected, the smoker satiety group had a higher exhaled CO immediately prior to scanning than the other study groups (Student t‐tests, p's < 0.0001). The injected radioligand dose was similar for the nonsmoker, satiety smoker and abstinent smoker groups (196.4 ± 5.0, 195.9 ± 5.8 and 195.1 ± 5.0 MBq, respectively; p = 0.72).
The primary overall analysis of PET/CT data revealed a significant main effect of group (F [2, 55] = 6.3, p = 0.003), due to the smoker satiety group having significantly lower WB SUVs than both the nonsmoking control (−15.3%; F [1, 36] = 9.4, p = 0.004) and abstinent smoker (−12.3%; F [1, 41] = 9.4, p = 0.004) groups (Table 2 and Figure 2). The nonsmoking control and abstinent smoker groups had mean WB SUVs that were similar to one another (3.0% group difference; F [1, 32] = 0.4, p = 0.51). For the smaller VOIs, 13 of the 14 SUVs had a significant main effect of group (F [2, 55] = 4.0–9.1, p ≤ 0.001–0.02; Table 2), while the remaining VOI approached significance (F [2, 55] = 2.9, p = 0.06). These results were due to the smoker satiety group having lower SUVs than both the nonsmoking control (range: 8.9%–19.4%) and smoking abstinence (range: 10.9%–13.8%) groups. As an aside, since body weight was nonsignificantly higher in the abstinent smoker group (Table 1) and was used to calculate SUV, an analysis was run using the same variables as above with the addition of body weight as a nuisance covariate; in this analysis, the significant main effect of group was essentially unchanged (F [2, 54] = 6.7, p = 0.002).
Scatterplots showing standardized uptake values (SUVs) for the whole brain (WB) and smaller volumes of interest for the three study groups (nonsmokers, smokers in the satiated state and smokers in 3 days of continuous abstinence state).
In the exploratory analyses of symptom rating scales at the time of PET/CT scanning, a significant inverse relationship was found between WB SUV and mood ratings for the whole smoker group (partial correlation coefficient = −0.35, p = 0.02; Figure 3), while a trend toward a significant inverse relationship was found between WB SUV and the single item analogue craving rating for the whole smoker group (partial correlation coefficient = −0.28, p = 0.08). No other correlations between WB SUV and symptom ratings were significant (p values ranged from 0.27 to 0.38).
Scatterplots showing exploratory correlations between WB SUV and cigarette withdrawal ratings for mood and craving at the time of PET/CT scanning.
Discussion
4
The main study results were that smokers who smoked to satiety had lower levels of the marker for gliosis than nonsmokers and this effect was not present in smokers who maintained CS abstinence for 3 days. Using a different PET/CT radiotracer and an independent group of participants, this study strengthens support for previous findings of decreased TSPO binding with acute smoking [37] and is consistent with the finding of decreased binding with overnight abstinence [43]. Furthermore, the magnitude of the low binding here (−15.3%) was similar to that found in the previous studies (−16.8 and roughly −16.3%, respectively) and also similar to findings in chronic alcohol use disorder [67, 68]. These findings in the brain with acute CS are consistent with known effects of smoking in the body, namely, impaired inflammation and prolonged wound healing [4, 5].
The new finding that smokers abstinent for 3 days did not have decreased TSPO binding compared with nonsmokers suggests that lowered levels of gliosis from smoking resolve during the period between overnight and 3 days of smoking abstinence. As noted above, inhaled cigarette smoke has thousands of constituents [2, 69, 70] with a range of half‐lives. Nicotine, a primary addictive constituent of tobacco smoke, has a half‐life of about 2–3 h [44], while its major metabolite (cotinine) [45, 46] and the combination of all its major metabolites [47] have half‐lives of approximately 16–19 h. Other constituents of tobacco smoke (e.g., benzene, CO) have half‐lives ranging from 1 to 4.6 h [71, 72]. Therefore, PET/CT results from 3 days of smoking abstinence may be explained by elimination of CS constituents leading to normalization of gliosis, although other explanations are possible. For example, stopping smoking may result in alterations in radioligand delivery, change in radioligand clearance associated with removal of cigarette smoke constituents or lessening of elevated cholesterol levels [73], which has previously been shown to inversely correlate with TSPO radioligand binding [68]. It should also be noted that we did not find an association between plasma nicotine levels and WB SUV in our previous study [37], which may indicate that elimination of other CS constituents is responsible for the main study result here. As a possible example, CO is a constituent of tobacco smoke that has greater affinity for haemoglobin than oxygen and negatively affects oxygen delivery to tissue, which is known to be essential for wound healing in the body [74]; therefore, it may be inferred that elimination of CO from the body during short‐term abstinence is a contributor to the main finding here. Another possible interpretation of study findings is that removal of the anti‐inflammatory effect of CS/nicotine may lead to worse withdrawal symptoms (as implied by the exploratory inverse correlation found here between WB SUV and mood). These findings also point to the need to control for CS in brain imaging studies of populations that have high rates of CS, such as those with mental illness and/or substance abuse [75].
Normalization of the marker for gliosis implies an important health improvement in smokers who quit, namely improved ability to respond to CNS injury and decreased likelihood of cognitive impairment [6]. This finding potentially puts normalization of gliosis in the same category of health benefits of quitting smoking as other short‐term benefits (e.g., drop in heart rate/blood pressure, removal of CO from the body and improvements in taste/smell and lung mucus clearance) [76].
While exploratory in nature, the inverse associations between TSPO binding and symptoms are consistent with prior research. For the mood state scale, higher TSPO binding was associated with worse mood at the time of scanning in the whole smoker group. This result is consistent with much literature demonstrating increased TSPO binding in people with major depressive disorder (MDD) [48, 77]. Higher regional TSPO binding has also been found to correlate with both greater MDD symptom severity [78] and reductions in depressive symptoms with treatment [29], although it is recognized that mood in people with MDD and mood state related to smoking may have different biological substrates. For the craving scale, greater craving had a trend toward an association with lower levels of TSPO binding, which is consistent with our previous report of greater withdrawal stimulation being associated with lower TSPO availability [37]. While correlations are consistent with prior research, results should be interpreted with caution, as we did not have specific hypotheses about these relationships and multiple correlations were run which would not have passed strict multiple comparison correction.
Limitations of the study were primarily related to the complex nature of CS and the PET/CT method used. Because CS contains thousands of constituents [79, 80], it is not possible to know which (if any) resulted in the lower levels of radioligand binding found here in smokers who smoked to satiety. In our prior study [37], we found an inverse association between cigarettes smoked per day and a PET marker for gliosis but did not find associations between the PET marker and plasma nicotine/cotinine. Because of modest sample sizes, it was not possible to definitively conclude that nicotine does not cause decreased gliosis. Given the growing prevalence of vaping [81, 82, 83, 84], which typically delivers nicotine, future research of this type could focus on people who vape to help determine the role of nicotine in the findings in this study. Additionally, building upon initial studies [85], longitudinal research could be conducted using animals to determine CS and vaping effects on TSPO binding over time. As for the PET/CT method, while radioligand binding to TSPO is thought to be substantially related to its expression during microglial and to a lesser extent, astroglial activation, TSPO is not fully selective [14, 48] and such binding may reflect inflammatory cell density [86]. In addition, the absence of arterial blood sampling precluded determination of Vt, which is a gold standard outcome measure for this type of research. Vt may control for potential confounds of between‐subject differences in radioligand delivery and binding to plasma protein [87, 88]. Finally, the cross‐sectional nature of the study did not allow for a definitive determination of normalization of TSPO levels, since participants were not scanned repeatedly over time, related to concerns about feasibility and tolerability.
Despite these limitations, several aspects of the study lend confidence to the findings. First, this study represents the third time (using independent groups of participants and two different radioligands) that acute CS (or brief abstinence) was found to result in lower TSPO binding. Second, results are consistent with the known effects of smoking in the body, including impaired inflammation and prolonged wound healing. Third, study groups were well‐matched on all variables obtained. And fourth, the time frame for resolution of lower TSPO binding was consistent with the known clearance of constituents of tobacco smoke from the body. Future research could focus on establishing which constituents of cigarette smoke alter levels of the marker for gliosis. Taken together, these findings may demonstrate a previously unknown health benefit of quitting smoking.
Author Contributions
A.L.B., M.G.M., B.R., D.V., J.H.M., J.W.Y., and C.K.H. designed the study. A.L.B., A.Y.S., R.B.A., N.G., A.K.M., A.W., J.H.B., M.G.M., K.K.K., and C.K.H. acquired the data. A.L.B., A.Y.S., R.B.A., J.H.M., and C.K.H. analyzed and interpreted the data. All authors contributed to the writing and gave final approval for the manuscript.
Ethics Statement
The study was approved by the IRB at the VA San Diego Healthcare System (#1204452).
Conflicts of Interest
The authors declare no conflicts of interest.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1X. Dai , G. F. Gil , M. B. Reitsma , et al., “Health Effects Associated With Smoking: A Burden of Proof Study,” Nature Medicine 28, no. 10 (2022): 2045–2055, 10.1038/s 41591-022-01978-x.PMC 955631836216941 · doi ↗ · pubmed ↗
- 2US Department of Health and Human Services , “The Health Consequences of Smoking—50 Years of Progress. A Report of the Surgeon General,” U.S. Department of Health and Human Services, Centers for Disease Control, National Center for Chronic Disease Prevention and Health Promotion, Office on Smoking and Health, (2014).
- 3“How Tobacco Smoke Causes Disease: The Biology and Behavioral Basis for Smoking‐Attributable Disease: A Report of the Surgeon General,” (Atlanta, GA: U.S. Department of Health and Human Services, Centers for Disease Control and Prevention, National Center for Chronic Disease Prevention and Health Promotion, Office on Smoking and Health, 2010).
- 4J. Towler , “Cigarette Smoking and Its Effects on Wound Healing,” Journal of Wound Care 9, no. 3 (2000): 100–104, 10.12968/jowc.2000.9.3.25962.11933289 · doi ↗ · pubmed ↗
- 5R. B. Goncalves , R. D. Coletta , K. G. Silverio , et al., “Impact of Smoking on Inflammation: Overview of Molecular Mechanisms,” Inflammation Research 60, no. 5 (2011): 409–424, 10.1007/s 00011-011-0308-7.21298317 · doi ↗ · pubmed ↗
- 6D. J. Di Sabato , N. Quan , and J. P. Godbout , “Neuroinflammation: The Devil Is in the Details,” Journal of Neurochemistry 139, no. 2 (2016): 136–153, 10.1111/jnc.13607.26990767 PMC 5025335 · doi ↗ · pubmed ↗
- 7S. Salerno , M. Viviano , E. Baglini , et al., “TSPO Radioligands for Neuroinflammation: An Overview,” Molecules 29, no. 17 (2024): 4212, 10.3390/molecules 29174212.39275061 PMC 11397380 · doi ↗ · pubmed ↗
- 8W. Zhang , D. Xiao , Q. Mao , and H. Xia , “Role of Neuroinflammation in Neurodegeneration Development,” Signal Transduction and Targeted Therapy 8, no. 1 (2023): 267, 10.1038/s 41392-023-01486-5.37433768 PMC 10336149 · doi ↗ · pubmed ↗