Functional outcomes following injury in centenarians: a nationwide retrospective observational study
Ryo Yamamoto, Brian J. Eastridge, Ramon F. Cestero, Keitaro Yajima, Akira Endo, Kazuma Yamakawa, Junichi Sasaki

TL;DR
This study examines the outcomes of injuries in centenarians, identifying factors that predict mortality and loss of independence after injury.
Contribution
The study provides new insights into clinical predictors of mortality and functional decline in centenarians following injury.
Findings
Male gender, non-fall injuries, and lower GCS on arrival predicted higher in-hospital mortality.
Injury severity in extremities/pelvis predicted dependent living after injury.
Only 22.2% of centenarians regained independent living post-injury despite 50.9% being independent beforehand.
Abstract
Advances in healthcare and the development of various technologies have improved disease-free longevity. Although the number of healthy centenarians is gradually increasing, studies on postinjury functions among centenarians are lacking. Therefore, we aimed to determine the clinical predictors of mortality and unfavorable functions after injury among centenarians. A retrospective study was conducted using a nationwide trauma database, and data from patients aged ≥ 100 years across ≥ 250 institutions during 2019–2022 were analyzed. Patient demographics, comorbidities, mechanism of injury, injury severity, vital signs on arrival, and pre- and in-hospital treatments were compared between survivors and non-survivors as well as between survivors who had and did not have the ability to live independently at discharge, which was defined as Glasgow Outcome Scale (GCS) score of ≤ 3. Independent…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
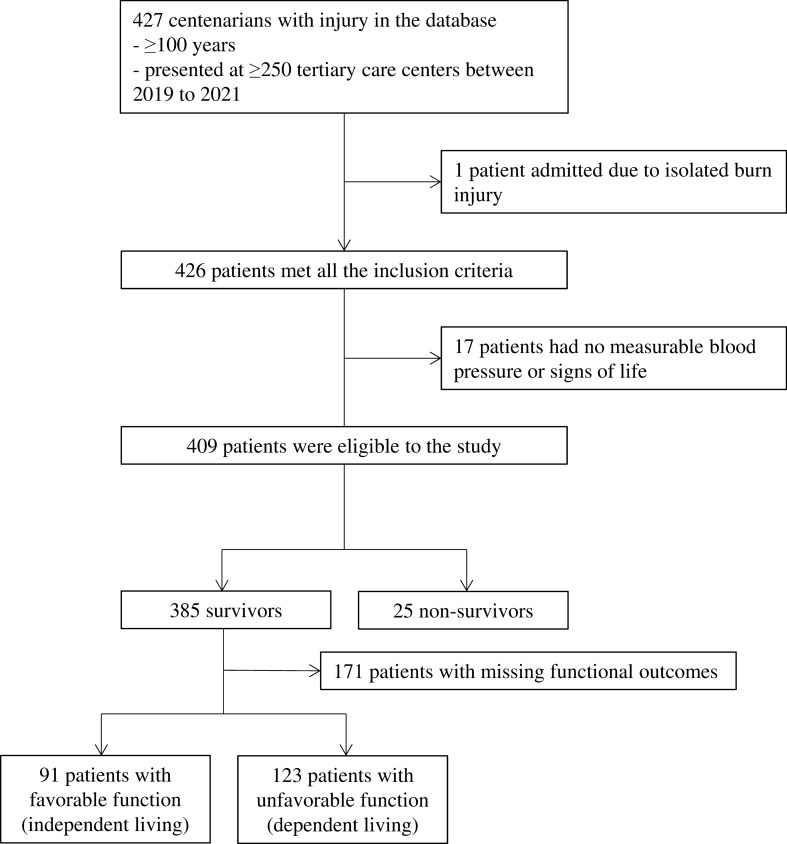 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsFrailty in Older Adults · Hip and Femur Fractures · Trauma and Emergency Care Studies
Background
Advances in healthcare and the development of various technologies have improved the field of preventive medicine and disease-free longevity [1]. Although life expectancy varies across countries/regions depending on socioeconomic status [2], the number of healthy centenarians is gradually increasing globally [3]. Notably, early recovery from severe diseases and tailored rehabilitation can sustain physical functions even among centenarians with several comorbidities [4].
Although optimal physical abilities help maintain the quality of life of centenarians [5], independent living can be a risk factor for injury, which is an emerging medical concern in matured health systems [6]. A recent single-center observational study involving 13 centenarians admitted due to trauma within the past 3 years showed that 12 of them could walk with a frame or stick before injury [7]. Another retrospective study involving 69 centenarians with hip fractures showed that > 50% of them could walk independently without supervision before injury [8]. Although there is limited evidence suggesting an increase in trauma incidence due to walking [9], the occurrence of injury during normal daily activities may be common among centenarians.
However, studies on postinjury outcomes, specifically functional outcomes, among centenarians are lacking. Most previous studies have been conducted among a small number of patients, with mortality being the only targeted outcome [10–12]. A retrospective study involving 474 injured nonagenarians/centenarians (aged ≥ 90 years) extensively examined patient characteristics and cumulative mortalities. Although head and spine injuries, high injury severity, and mechanical ventilation use were identified as predictors of mortality, functional outcomes were not provided or analyzed [11]. Considering that centenarians have unique physiological features, such as vulnerability to chronic inflammation and infectious diseases [13, 14], it is necessary to determine the clinical consequences after injury, including functional abilities, in this specific population.
Using a nationwide trauma database, we examined patient, injury, and treatment characteristics associated with mortality and unfavorable functions after injury among centenarians. We aimed to determine the clinical predictors of mortality and unfavorable functions after injury among centenarians.
Methods
Study design and setting
We conducted a retrospective cohort study using the Japan Trauma Data Bank (JTDB), which was established as a nationwide trauma registry in 2003 and maintained by the Japanese Association for the Surgery of Trauma (JAST) and the Japanese Association for Acute Medicine [15]. The JTDB database includes data from > 250 tertiary care centers, with most high-level tertiary care centers participating in the JTDB. The current research involving humans was approved by the institutional review boards of all participating hospitals. The need for informed consent was waived because of data anonymity.
The management protocol for trauma patient resuscitation in Japan, including the older population, was developed by the JAST based on the Advanced Trauma Life Support training program of the American College of Surgeons. As some hospitals in Japan do not always have trauma surgeons, emergency physicians sometimes independently decide and conduct the initial resuscitation. Japan is one of the countries with the longest life expectancy [16]; thus, trauma among centenarians is not rare and it is seen in most tertiary care centers without consultation with a geriatric physician.
Study population
We reviewed data from the JTDB between 2019 and 2022. We included patients (1) who were aged ≥ 100 years and (2) admitted due to nonburn injury. Moreover, we excluded those without measurable blood pressure or signs of life (pupillary response, spontaneous ventilation, extremity movement, or cardiac electrical activity) upon hospital arrival.
Data collection and definition
JTDB data included age; gender; physical disability before injury; mechanism of injury; vital signs on arrival; Abbreviated Injury Scale (AIS) score; Injury Severity Score (ISS); prehospital treatments, including intubation, fluid administration, and transfusion; presence of a physician at the prehospital stage; transportation time; resuscitative procedures after hospital arrival, including surgery/angiography; length of intensive care unit stay; length of ventilator use; survival status at discharge; and Glasgow Outcome Scale (GOS) at discharge.
Outcome measures
GOS was used to evaluate functional outcome at discharge, which was the primary outcome [17]. Unfavorable and favorable functional outcomes were defined as GOS scores of ≤ 3 and ≥ 4, respectively (1, dead; 2, vegetative state and unable to interact; 3, severe disability and unable to live independently; 4, moderate disability and unable to resume previous social activities; 5, good recovery and able to resume previous social activities).
Statistical analysis
Patient, injury, treatment, and outcome characteristics were compared between survivors and non-survivors at discharge and between survivors who had and did not have unfavorable functional outcomes. Characteristics related to in-hospital mortality and unfavorable functional outcomes (GOS ≤ 3) were analyzed using multivariate logistic regression analyses fitted with a generalized estimating equation (GEE) model [18], accounting for within-institution clustering to consider institutional and regional differences in the management of centenarians with injury. In the GEE model, relevant potential covariates were selected from known predictors of clinical outcomes in patients with trauma and older individuals based on previous studies [11, 19–21]. To account for the limited sample size, we selected covariates in the final GEE models from the patient, injury, and treatment variables that showed a difference in univariate analyses.
Two sensitivity analyses were performed to validate the predictors of in-hospital mortality and unfavorable functional outcomes. First, as endogeneity between the age of ≥ 100 years and low tendency to provide invasive treatment is expected, GEE models without treatment variables after hospital arrival were developed, and predictors of in-hospital mortality and unfavorable function were examined. Second, considering the low number of included patients, logistic regression models with bootstrapping (the model is resampled 1,000 times) were developed [22] using the same variables in the primary analysis.
Descriptive statistics were presented as means (standard deviations), medians (interquartile ranges), or numbers (percentages). In hypothesis testing, significance was considered at a two-sided α-threshold of 0.05. In the variable selection for the final GEE models, an α threshold of 0.1 indicated a significant difference in univariate analyses. The association between each clinical factor and in-hospital mortality or unfavorable functional outcome was presented as odds ratio (OR) with a 95% confidence interval. All statistical analyses were performed using Statistical Package for the Social Sciences (version 29.0; IBM Corp., Armonk, NY, USA).
Results
Patient characteristics
Among 427 centenarians with injury in the database, 409 had measurable blood pressure with vital signs and were admitted due to nonburn injury, making them eligible for the study (Fig. 1). Moreover, 385 (94.1%) centenarians survived at discharge, and 91/214 (42.5%) patients had favorable function with abilities to live independently at discharge.Fig. 1. Patient flow diagram. Among 427 centenarians with injury in the database, 409 had measurable blood pressure and vital signs and were admitted due to nonburn injury, making them eligible for this study. A total of 385 centenarians (94.1%) survived at discharge, and 91/214 (42.5%) patients had favorable function with abilities to live independently at discharge
Table 1 shows patient, injury, treatment, and outcome characteristics of survivors and non-survivors at discharge. Survivors had higher GCS and lower respiratory rate (RR) on arrival (14 [13–15] vs. 11 [5–14] and 19/min [16–21] vs. 22/min [17–26]), lower AIS in the head/neck, and higher AIS in the extremity/pelvis (0 [0–0] vs. 3 [0–5] and 3 [3] vs. 2 [0–3]) than non-survivors. Furthermore, a higher number of survivors experienced fall from standing and underwent surgery in the extremity/pelvis (339 [88.3%] vs. 16 [64.0%] and 222 [57.8%] vs. 3 [12.0%]).Table 1. Characteristics of centenarians with traumaSurvivorNonsurvivorp-valueCase38425Age, years, median (IQR)101(100–102)101(100–102)0.923Gender, male, n (%)48(12.5%)9(36.0%)0.001Charlson comorbidity index, median (IQR)1(0–1)1(1–2)0.116Physical disability before injury, n (%)192(53.8%)16(72.7%)0.083Mechanism of injury, blunt, n (%)374(100.0%)21(100.0%)–Fall—from standing, n (%)339(88.3%)16(64.0%)** < 0.001Fall—others, n (%)23(6.0%)3(12.0%)0.206Vital signs on hospital arrival, median (IQR)GCS14(13–15)11(5–14) < 0.001SBP, mmHg151(131–169)147(95–170)0.289HR, /min80(70–90)85(68–108)0.325RR, /min19(16–21)22(17–26)0.049SpO_2_, %97(95–98)97(95–99)0.633AIS, median (IQR)Head/neck0(0–0)3(0–5) < 0.001Face0(0–0)0(0–0)0.526Chest0(0–0)0(0–0)0.523Abdomen0(0–0)0(0–0)0.895Extremity/Pelvis3(3–3)2(0–3)0.003Body surface0(0–0)0(0–0)0.256ISS, median (IQR)9(9–9)16(9–25) < 0.001Prehospital procedure, n (%)Intubation0(0.0%)0(0.0%)–Fluid administration5(1.3%)3(12.0%)0.009Transfusion0(0.0%)0(0.0%)–Physician presence at prehospital2(0.5%)0(0.0%)0.880Transportation time, min, median (IQR)27(21–37)25(19–35)0.460Surgery/angiography, n (%)Head6(1.6%)1(4.0%)0.359Neck0(0.0%)0(0.0%)–Face1(0.3%)0(0.0%)0.939Chest0(0.0%)0(0.0%)–Abdomen0(0.0%)0(0.0%)–Extremity/pelvis222(57.8%)3(12.0%) < 0.001**Body surface1(0.3%)0(0.0%)0.939Clinical outcomes, days, mean (SD)Length of ICU stay1(2)1(2)0.892Ventilator use0(3)0(0)0.501Bold values indicate the significance is defined as* p*-value < 0.05IQR, interquartile range; GCS, Glasgow coma scale; SBP, systolic blood pressure; HR, heart rate; RR, respiratory rate; SpO_2_, peripheral oxygen saturation; AIS, Abbreviated Injury Scale; ISS, Injury Severity Score; ICU, intensive care unit
Table 2 shows the characteristics of centenarians who survived with and without favorable functional outcomes. Compared with those without favorable function, centenarians with favorable function had higher AIS in the head/neck, chest, and abdomen and lower AIS in the extremity/pelvis (3 [0–3] vs. 3 [3]). Moreover, centenarians with abilities to live independently at discharge underwent surgery in the extremity/pelvis less frequently (46 [50.5%] vs. 87 [70.7%]).Table 2. Characteristics of survivorsIndependent livingDependent livingp-valueCase91123Functional status at discharge, n (%)Able to resume previous social activities50(54.9%)––Unable to resume previous social activities41(45.1%)––Unable to live independently–122(99.2%)–Unable to interact–1(0.8%)–Age, years, median (IQR)101(100–102)101(100–102)0.300Gender, male, n (%)11(12.1%)10(8.1%)0.336Charlson Comorbidity Index, median (IQR)1(0–1)1(0–1)0.299Physical disability before injury, n (%)50(56.2%)80(65.6%)0.107Mechanism of injury, blunt, n (%)88(100.0%)118(100.0%)–Fall—from standing, n (%)78(85.7%)109(88.6%)0.527Fall—others, n (%)8(8.8%)7(12.0%)0.380Vital signs on hospital arrival, median (IQR)GCS14(13–15)14(13–15)0.515SBP, mmHg155(134–171)153(133–170)0.450HR, /min80(72–91)80(70–88)0.711RR, /min20(17–23)18(16–20)0.051SpO_2_, %97(94–98)96(94–98)0.226AIS, mean (SD), median (IQR)Head/Neck1 (1),0 (0–0)0 (1),0 (0–0)0.026Face0 (0),0 (0–0)0 (0),0 (0–0)0.182Chest0 (1),0 (0–0)0 (0),0 (0–0)0.001Abdomen0 (1),0 (0–0)0 (0),0 (0–0)0.041Extremity/Pelvis2 (1),3 (0–3)3 (1),3 (3–3)** < 0.001**Body surface0 (0),0 (0–0)0 (0),0 (0–0)0.204ISS, median (IQR)9(9–9)9(9–9)0.577Prehospital procedure, n (%)Intubation0(0.0%)0(0.0%)–Fluid administration2(2.2%)1(0.8%)0.388Transfusion0(0.0%)0(0.0%)–Physician presence at prehospital1(1.1%)1(0.8%)0.668Transportation time, min, median (IQR)30(22–37)25(19–39)0.139Surgery/angiography, n (%)Head1(1.1%)2(1.6%)0.612Neck0(0.0%)0(0.0%)–Face0(0.0%)0(0.0%)–Chest0(0.0%)0(0.0%)–Abdomen0(0.0%)0(0.0%)–Extremity/Pelvis46(50.5%)87(70.7%)0.003Body surface1(1.1%)0(0.0%)0.425Clinical outcomes, days, mean (SD)Length of ICU stay0(1)1(3)0.070Ventilator use0(0)1(5)0.652Bold values indicate the significance is defined as* p*-value < 0.05IQR, interquartile range; GCS, Glasgow coma scale; SBP, systolic blood pressure; HR, heart rate; RR, respiratory rate; SpO_2_, peripheral oxygen saturation; AIS, Abbreviated Injury Scale; SD, standard deviation; ISS, Injury Severity Score; ICU, intensive care unit
Clinical predictors of in-hospital mortality
To account for institutional differences in the management of centenarians, we developed the GEE model to predict in-hospital mortality, which included gender, physical disability before injury, mechanism of injury, GCS and RR on arrival, AIS in the head/neck and extremity/pelvis, ISS, prehospital fluid resuscitation, and surgery in the extremity/pelvis as covariates based on the results in univariate analyses (Table 3).Table 3. Clinical factors associated with in-hospital mortality of centenarianp-valueOR (95% CI)Patient characteristicsMale**0.0145.75(1.43–23.26)Physical disability before injury0.2242.74(0.57–10.64)Severity of injuryFall from standing < 0.0010.11(0.03–0.37)GCS on hospital arrival, by one point decrease0.0051.35(1.09–1.66)RR on hospital arrival, by 1/min increase0.1671.04(0.99–1.09)AIS in head/neck, by one point increase0.0962.12(0.88–5.11)AIS in extremity/pelvis, by one point increase0.2111.65(0.75–3.62)ISS, by one point increase0.2870.91(0.77–1.08)TreatmentPrehospital fluid administration0.1546.21(0.51–76.92)Surgery/angiography in the extremity/pelvis0.0570.05(0.00–1.10)Bold values indicate the significance is defined as p-value < 0.05OR, odds ratio; CI, confidence interval; GCS, Glasgow coma scale; RR, respiratory rate; AIS, Abbreviated Injury Scale; and ISS, Injury Severity Score
This adjusted model revealed several clinical factors related to in-hospital mortality: male gender (OR for in-hospital mortality, 5.75 [1.43–23.26]; p = 0.014) and lower GCS on arrival (OR for in-hospital mortality, 1.35 [1.09–1.66]; p = 0.005). Conversely, fall from standing was associated with lower in-hospital mortality among centenarians (OR, 0.11 [0.03–0.37]; p < 0.001).
In the sensitivity analyses with another GEE model without treatment variables after hospital arrival and a logistic regression model with bootstrapping, male gender, GCS on hospital arrival, and mechanism of injury other than fall from standing were independent predictors of in-hospital mortality (Table S1).
Clinical predictors of unfavorable functional outcomes
The final GEE model to predict dependency in daily life at discharge included physical disability before discharge; RR on hospital arrival; AIS in the head/neck, chest, abdomen, and extremity/pelvis; and surgery in the extremity/pelvis (Table 4). However, only AIS in the extremity/pelvis was associated with unfavorable functional outcomes following injury among centenarians (OR 1.98 [1.19–3.28]; p = 0.009). Moreover, sensitivity analyses showed that AIS in the extremity/pelvis was the only predictor of dependent living after injury (Table S1).Table 4. Clinical factors associated with unfavorable function of centenariansp-valueOR (95% CI)Patient characteristicsPhysical disability before injury0.6931.18(0.52–2.65)Severity of injuryRR on hospital arrival, by 1/min increase0.5460.98(0.91–1.05)AIS in head/neck, by one point increase0.1811.35(0.87–2.09)AIS in chest, by one point increase0.3530.79(0.47–1.31)AIS in abdomen, by one point increase0.8121.14(0.39–3.36)AIS in extremity/pelvis, by one point increase**0.0091.98(1.19–3.28)TreatmentSurgery/angiography in the extremity/pelvis0.7731.13(0.50–2.56)Bold values indicate the significance is defined as p-value < 0.05OR, odds ratio; CI, confidence interval; RR, respiratory rate; and AIS, Abbreviated Injury Scale
Discussion
This study identified that > 50% of centenarians had inadequate abilities to live independently after injury treatment, whereas > 90% could survive to discharge. In addition, injury severity in the extremity/pelvis was the only predictor of unfavorable function, whereas male gender, lower GCS, and mechanism of injury other than fall from standing were associated with increased in-hospital mortality.
Several beneficial features of the identified predictors should be considered for clinical implications. First, injury in the musculoskeletal system may highly disrupt the ability to live independently among centenarians. Although previous studies have reported that fracture fixation in the extremity/pelvis was associated with unfavorable outcomes [23, 24], our study indicated that this relationship might have been due to the confounding effects of injury severity. Thus, surgery should be performed as needed. Second, the physiological rather than anatomical severity of traumatic brain injury would be a significant predictor of in-hospital mortality among centenarians. Although AIS in the head was not independently associated with mortality in this study, GCS on arrival substantially affected survival to discharge, which was consistent with previous reports of a linear correlation between the initial GCS and mortality from TBI [25, 26]. Third, the mechanism of injury would be associated with in-hospital mortality but not with functional outcomes in centenarians. Although fall from standing was related to lower in-hospital mortality, a considerable number of centenarians did not regain adequate ability to live independently after fall from standing, indicating that this is a serious mechanism in this population.
Notably, among the centenarians who could live independently at discharge, > 50% had lived with physical disability before injury, which might be due to appropriate rehabilitation and optimal installation of assistive equipment at home during hospital stay [27, 28]. Therefore, we do not recommend limiting treatment based on preinjury physical disability. Conversely, one-third of the centenarians with dependency in daily life at hospital discharge did not have a physical disability before trauma. As this loss of capability would significantly impede the quality of life of healthy centenarians, further investigation should be conducted to manage the subpopulation of centenarians whose ideal physical function is impaired by severe extremity/pelvis injury.
Although several prognostic factors were identified for in-hospital mortality and functional consequences following trauma, we only examined survival status and functions at discharge. Considering that long-term outcomes, such as abilities for daily living a year after injury, are more clinically feasible as a goal of treatment, other predictors of favorable function may exist. However, because the age of ≥ 100 years is longer than the life expectancy in any countries/regions and treatment tends to be easily deviated from the standard [29], the identified predictors in this study might help in the decision-making process while treating centenarians with injury.
Limitations
Our study results must be interpreted within the context of the study design. We analyzed data obtained from the JTDB, which does not record treatment details. Therefore, our results may differ with existing unmeasured confounding factors, such as patient preference and resources related to geriatric medicine. However, sensitivity analyses after excluding in-hospital treatment variables had similar results, wherein possible endogeneity between the age of ≥ 100 years and low tendency to provide invasive treatment in centenarians was minimized. Another limitation is the lack of data on strategies for rehabilitation. In addition to injury treatment, we could not evaluate the timing and intensity of rehabilitation, which were related to unfavorable functional outcomes. Furthermore, the database did not include ability for each daily activity, such as eating, dressing, toileting, and working. Although some of the abilities are more important depending on the living environment, we could not evaluate predictors of each ability. Moreover, the outcome used in this study was GOS, which is generally evaluated ≥ 6 months after injury. Considering that physical function gradually improves in some patients, unfavorable functional outcomes might have been overestimated. Although we used a nationwide database, the sample size was still limited due to the nature of the targeted population. The identified predictors of in-hospital mortality and unfavorable functional outcomes following injury should be validated using a large cohort of centenarians.
Conclusions
Our study showed that > 50% of centenarians could not live independently at hospital discharge after injury treatment, whereas > 90% could survive. Injury severity in the extremity/pelvis was the only predictor of unfavorable functions after injury, whereas male gender, mechanisms of injury other than fall from standing, and GCS on arrival were associated with higher in-hospital mortality.
Supplementary Information
Additional file 1.