Isolated Adrenocorticotropic Hormone Deficiency Mimicking Systemic Sclerosis: A Diagnostic Challenge in Patients With Rheumatoid Symptoms
Yohei Fujita, Masahiro Hatazaki

TL;DR
A case of isolated ACTH deficiency mimicked systemic sclerosis, but was correctly diagnosed and treated with hydrocortisone, improving symptoms like joint swelling and skin changes.
Contribution
This case highlights the diagnostic challenge of IAD presenting with rheumatoid symptoms and emphasizes the importance of adrenal function testing in such patients.
Findings
Hydrocortisone therapy improved symptoms of joint swelling, skin sclerosis, and thyroid dysfunction in a patient with IAD.
IAD can mimic autoimmune diseases like systemic sclerosis, leading to potential misdiagnosis.
Thyroid dysfunction in IAD patients may resolve with cortisol replacement therapy.
Abstract
Isolated adrenocorticotropic hormone (ACTH) deficiency (IAD) is characterized by selective impairment of ACTH secretion while other anterior pituitary hormones remain unaffected. It is more common in men in their fifties, with autoimmune mechanisms likely playing a major role. Symptoms include fatigue, weight loss, and appetite loss. Some IAD patients also experience rheumatoid symptoms, such as muscle pain and joint stiffness. A 74-year-old male patient with type 2 diabetes mellitus developed worsening symptoms, including impaired consciousness, fatigue, and edema. A month before hospitalization, he was diagnosed with primary hypothyroidism and started on levothyroxine. However, his symptoms worsened, with finger contractures and joint swelling, prompting referral to our hospital. On admission, he showed signs of general malaise and facial changes. His skin showed sclerosis without…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
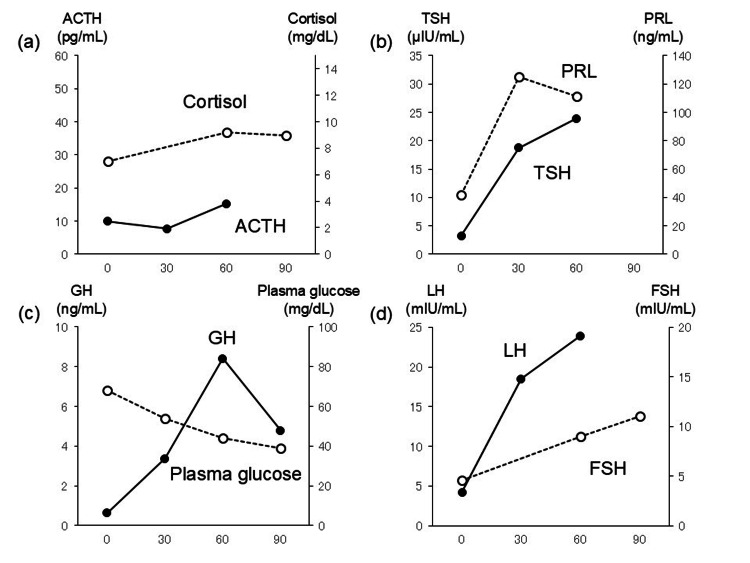 Figure 1
Figure 1| Variables | Patient value | Reference ranges |
| Complete blood count | ||
| White blood cell counts | 8,900 /µL | 3,300-8,600 /µL |
| Neutrophils | 65.50% | 25-72% |
| Eosinophil | 9.00% | 0-7.0% |
| Basophil | 0.40% | 0-1.0% |
| Monocytes | 9.20% | 4.0-7.0% |
| Lymphocytes | 15.90% | 30-45% |
| Red blood cell counts | 3.89x106 /µL | 4.2-5.6x106 /µL |
| Hemoglobin | 10.9 g/dL | 13-17 g/dL |
| Hematocrit | 32.20% | 39-52% |
| Platelet counts | 9.9x104 /µL | 1.3-3.6x104 /µL |
| Biochemistry | ||
| Albumin | 3.0 g/dL | 3.8-5.3 g/dL |
| Aspartate aminotransferase | 25 IU/L | 13-33 IU/L |
| Alanine aminotransferase | 12 IU/L | 8-42 IU/L |
| Lactate dehydrogenase | 206 IU/L | 119-229 IU/L |
| Alkaline phosphatase | 191 IU/L | 115-359 IU/L |
| γ-glutamyltransferase | 17 IU/L | 10-47 IU/L |
| Creatine kinase | 107 IU/L | 62-287 IU/L |
| Total bilirubin | 0.7 mg/dL | 0.3-1.2 mg/dL |
| Blood urea nitrogen | 10 mg/dL | 8-22 mg/dL |
| Serum creatinine | 0.41 mg/dL | 0.60-1.10 mg/dL |
| Serum uric acid | 1.2 mg/dL | 2.6-6.4 mg/dL |
| Serum sodium | 119 mEq/L | 138-146 mEq/L |
| Serum potassium | 4.9 mEq/L | 3.6-4.9 mEq/L |
| Serum chloride | 85 mEq/L | 99-109 mEq/L |
| Serum calcium | 7.7 mg/dL | 8.7-10.3 mg/dL |
| C-reactive protein | 3.39 mg/dL | < 0.40 mg/dL |
| Urinary sodium | 122 mmol/L | 110-250 mmol/L |
| Collagen disease-related tests | ||
| Antinuclear antibodies | < 40 | < 40 |
| Anti-topoisomerase I antibody | < 5.0 index | < 5.0 index |
| Anti-centromere antibodies | < 5 index | < 5 index |
| Anti-double-stranded deoxyribonucleic acid antibody | < 7.0 IU/mL | < 7.0 IU/mL |
| Anti-ribonucleoprotein antibody | < 5.0 index | < 5.0 index |
| Anti-smith antibody | < 5.0 index | < 5.0 index |
| Anti-Sjogren syndrome-A antibody | < 5.0 index | < 5.0 index |
| Anti-Sjogren syndrome-B antibody | < 5.0 index | < 5.0 index |
| Anti-Jo-1 antibody | < 7 index | < 7 index |
| Proteinase 3 anti-neutrophil cytoplasmic antibody | < 1.0 U/mL | < 1.0 U/mL |
| Myeloperoxidase-anti-neutrophil cytoplasmic antibody | < 1.0 U/mL | < 1.0 U/mL |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAdrenal Hormones and Disorders · Systemic Sclerosis and Related Diseases · Inflammatory Myopathies and Dermatomyositis
Introduction
The anterior pituitary gland secretes multiple hormones. When various causes, such as tumors, inflammation, trauma, bleeding, ischemia, and necrosis, damage the pituitary gland or hypothalamus, humans develop hyposecretion of pituitary hormones (generalized hypopituitarism, partial hypopituitarism) [1]. Among these, isolated adrenocorticotropic hormone (ACTH) deficiency (IAD) is characterized by selective impairment of ACTH secretion. Isolated adrenocorticotropic hormone deficiency is more common in men, with the average age of onset being in the fifties. The cause of IAD is unknown, but there are cases in which it is accompanied by other autoimmune diseases or in which anti-pituitary antibodies are present [1-3]. Clinical symptoms of IAD include generalized fatigue, loss of appetite, weight loss, and impaired consciousness [4]. Some patients with IAD may experience rheumatoid symptoms such as muscle pain, arthralgia, joint stiffness, and flexion contractures [5-7]. We report a case of a patient referred to our hospital with suspected systemic sclerosis (SSc) due to joint pain and finger contractures, who was ultimately diagnosed with IAD based on endocrinological tests.
Case presentation
A 74-year-old man with type 2 diabetes mellitus, diagnosed at age 57, had been visiting a local physician for routine care. About six months before hospitalization, he frequently experienced impaired consciousness. A blood test revealed hypoglycemia, leading to the discontinuation of oral hypoglycemic agents. The physician prescribed antihypertensive medication for low blood pressure, after which his episodes of impaired consciousness ceased. Concurrently, he developed lethargy, fatigue, and edema. One month before hospitalization, laboratory findings revealed elevated thyroid-stimulating hormone levels, leading to a diagnosis of primary hypothyroidism. He was started on levothyroxine (50 μg daily), after which impaired consciousness recurred. His fingers became thick and hard, and his joints swelled and contracted. Suspecting SSc, his local physician referred him to our hospital.
On admission, he was in poor general condition, with a blank facial expression and slurred speech. Vital signs included a temperature of 37.5°C, blood pressure of 131/78 mmHg, a pulse of 78 beats/minute (regular), and oxygen saturation (SpO₂) of 98% on room air. He had anorexia and dysphagia. No cardiac murmurs were detected, and breath sounds were clear bilaterally. The abdomen was soft without tenderness. He exhibited finger flexion contractures and skin sclerosis but no Raynaud's phenomenon. He had no rash, digital ulcers, fingertip necrosis, or telangiectasia. His elbows, shoulders, and knees had limited, painful motion. Lower extremity weakness impaired his ability to walk.
Laboratory tests (Table 1) showed negative autoantibodies for collagen diseases. A chest X-ray ruled out interstitial lung disease. Blood tests were negative for anti-topoisomerase I and anticentromere antibodies. According to the 2013 American College of Rheumatology/European League Against Rheumatism Classification Criteria for SSc, the patient did not meet the criteria, as he scored only four points for skin sclerosis of the fingers and two points for gastrointestinal dysfunction (esophageal motility abnormalities) [8].
Hyponatremia and hypoglycemia were managed with intravenous fluids. Oral medications, including levothyroxine and vasopressors, were discontinued. Urinary sodium levels exceeded 20 mmol/L, suggesting euvolemic hyponatremia. Hypertonic saline improved his level of consciousness. Despite physiological stress, ACTH and cortisol levels remained low, suggesting anterior pituitary insufficiency. Brain computed tomography (CT) revealed atrophy but no pituitary abnormalities. Magnetic resonance imaging (MRI) confirmed an intact pituitary gland and hypothalamus. A trunk CT scan showed no adrenal abnormalities.
Anterior pituitary function tests confirmed low ACTH and cortisol responses to CRH (Figure 1a). The patient had normal responses to thyrotropin-releasing hormone (TRH), luteinizing hormone-releasing hormone, and insulin hypoglycemia tests (Figure 1b, Figure 1c, and Figure 1d, respectively). He was diagnosed with IAD and started on intravenous hydrocortisone. Hyponatremia, hypoglycemia, and hypotension rapidly improved. Hydrocortisone was tapered to an oral maintenance dose of 10 mg in the morning and 5 mg in the evening [1,2]. Skin sclerosis and joint swelling improved with treatment. Since thyroid autoantibodies (anti-thyroglobulin and anti-thyroid peroxidase antibodies) were negative, Hashimoto's disease was unlikely. His thyroid function normalized after starting hydrocortisone, so we did not restart levothyroxine. During his illness, disuse syndrome progressed, leading to lower limb muscle weakness and dysphagia. Swallowing function improved with speech therapy, and the patient transitioned to a normal diet (1,600 kcal/day). After physical therapy, he was discharged on hospital day 72.
Anterior pituitary loading test(a) CRH test; (b) TRH test; (c) insulin hypoglycemia test; (d) LHRH testACTH: adrenocorticotropic hormone; CRH: corticotropin-releasing hormone; TRH: thyrotropin-releasing hormone; TSH: thyroid-stimulating hormone; PRL: prolactin; LHRH: luteinizing hormone-releasing hormone; LH: luteinizing hormone; FSH: follicle-stimulating hormone; GH: growth hormone
Discussion
Symptoms of IAD include general fatigue, loss of appetite, impaired consciousness, weight loss, cognitive decline, and joint contractures [1,2,4,7]. In SSc, dysphagia is commonly observed due to fibrosis of the esophageal smooth muscle. Similarly, patients with IAD may develop dysphagia due to hyponatremia. In this case, the presence of dysphagia led to the suspicion of an esophageal motility disorder associated with SSc. However, many of these symptoms result from cortisol deficiency. Hydrocortisone, administered at a dose of 10-20 mg/day, is the standard treatment for IAD, leading to rapid improvement in symptoms such as hyponatremia, hypoglycemia, and hypotension [2].
In children, IAD is often caused by genetic mutations, such as those in the TBX19 (TPIT) or POMC genes, leading to congenital ACTH deficiency [9,10]. In adults, IAD can develop after trauma or lymphocytic hypophysitis, the latter of which may be due to autoimmune etiology [11-13]. There are reports that the use of opioids and immune checkpoint inhibitors may lead to the development of IAD [14-16]. In our case, anti-pituitary antibodies were negative, and pituitary cavities, seen in approximately one-third of cases of IAD, were not observed [3]. In addition, because he was not using opioids or immune checkpoints, the mechanism of IAD development in this case was unclear.
Cortisol supplementation often improves abnormal responses of other hormones. Since cortisol acts in an inhibitory manner on TRH-thyroid-stimulating hormone (TSH) secretion, high TSH levels are observed in some cases of IAD. According to a report by Murakami et al., thyroid dysfunction is often observed in patients with IAD. In more than 70% of such cases, the abnormalities of the pituitary-thyroid axis were temporary and were reversed by glucocorticoid replacement [17]. In our case, IAD was presumed to have become manifest when he was started on thyroid hormone replacement at a local hospital.
Hoshino et al. reported the case of a 61-year-old man with IAD who presented with diffuse muscle and joint pain [5]. The widespread musculoskeletal pain resolved with physiological doses of hydrocortisone replacement therapy. In our case, his symptoms, such as skin sclerosis and finger swelling, improved after starting steroid hormone therapy. In patients with rheumatoid symptoms of unknown etiology, adrenal insufficiency may be the cause. Initially, the symptoms suspected to be SSc were presumed to be due to IAD.
Conclusions
Isolated adrenocorticotropic hormone deficiency can mimic autoimmune diseases like SSc, complicating diagnosis and delaying appropriate treatment. This case highlights the importance of considering endocrine disorders in patients with unexplained joint symptoms and skin changes. Additionally, thyroid hormone replacement therapy may unmask adrenal insufficiency, underscoring the necessity of adrenal function assessment before treatment initiation.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Isolated corticotrophin deficiency Pituitary Andrioli M Pecori Giraldi F Cavagnini F 289295920061707794910.1007/s 11102-006-0408-5 · doi ↗ · pubmed ↗
- 2Adrenal insufficiency Lancet Husebye ES Pearce SH Krone NP Kämpe O 61362939720213348463310.1016/S 0140-6736(21)00136-7 · doi ↗ · pubmed ↗
- 3Clinical heterogeneity of acquired idiopathic isolated adrenocorticotropic hormone deficiency Front Endocrinol (Lausanne) Fujita Y Bando H Iguchi G 5788021220213367961410.3389/fendo.2021.578802 PMC 7933588 · doi ↗ · pubmed ↗
- 4Isolated anterior pituitary dysfunction in adulthood Front Endocrinol (Lausanne) Prencipe N Marinelli L Varaldo E 11000071420233696776910.3389/fendo.2023.1100007 PMC 10032221 · doi ↗ · pubmed ↗
- 5Painful hypoadrenalism BMJ Case Rep Hoshino C Satoh N Narita M Kikuchi A Inoue M 02011201110.1136/bcr.01.2011.3735 PMC 307032022700071 · doi ↗ · pubmed ↗
- 6Isolated adrenocorticotropic hormone deficiency presenting with severe hyponatremia and rhabdomyolysis: a case report and literature review Am J Case Rep Komatsu T Ohara N Hirota N 185718632020193182706210.12659/AJCR.918427 PMC 6931390 · doi ↗ · pubmed ↗
- 7Isolated ACTH deficiency clinically presented as stiff-person syndrome, successfully treated by hormonal replacement: a case report (Article in Japanese)Rinsho Shinkeigaku Taneda T Okawara S Namekawa M Umeda Y Oyake M Fujita N 7367396220223603138110.5692/clinicalneurol.cn-001774 · doi ↗ · pubmed ↗
- 82013 classification criteria for systemic sclerosis: an American College of Rheumatology/European League Against Rheumatism collaborative initiative Arthritis Rheum van den Hoogen F Khanna D Fransen J 273727476520132412218010.1002/art.38098 PMC 3930146 · doi ↗ · pubmed ↗