Spontaneous isolated brachiocephalic artery dissection with subsequent type-A acute aortic dissection
Hisato Takagi

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
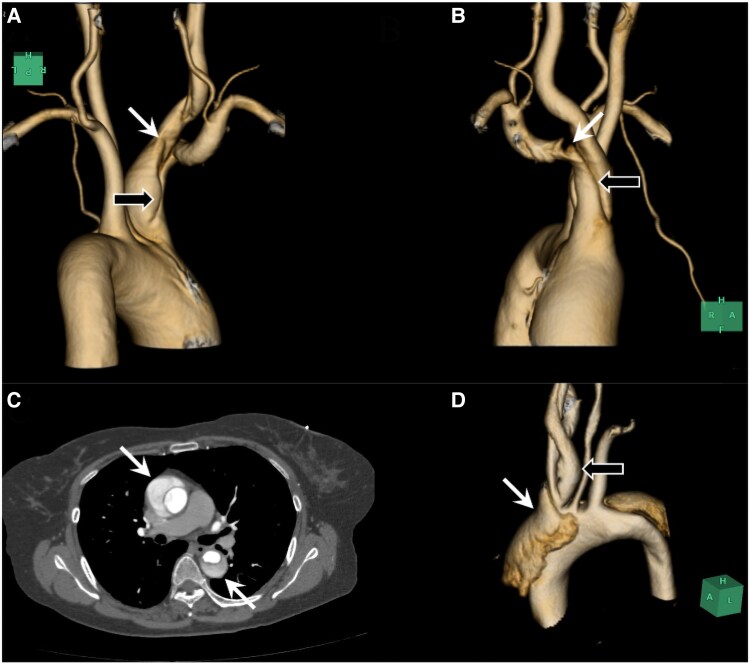 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAortic Disease and Treatment Approaches · Cardiac Structural Anomalies and Repair · Aortic aneurysm repair treatments
A 66-year-old woman with neither relevant co-morbidity except for treated hypertension nor history of trauma suffered sudden right neck pain radiating to the right upper extremity. Contrast-enhanced CT scans revealed limited dissection from the brachiocephalic aretry (BCA) (Figure 1A and B, black arrows) to the right common-carotid (Figure 1A, white arrow) and subclavian artery (Figure 1B, white arrow) with the patent false lumen. There was no dissection in the ascending, transverse, or descending-thoracic aorta. Spontaneous isolated BCA dissection (BCAD) was diagnosed, and the patient underwent conservative medical (antihypertensive and analgesic) treatment. No genetic testing was performed because the patient presented no physical characteristics of connective tissue disorders such as Marfan, Ehlers–Danlos, or Loeys–Dietz syndrome. Three years later, the patient suffered sudden chest pain, and type-A acute aortic dissection (AD) (TA-AAD) was diagnosed on contrast-enhanced CT scans (Figure 1C, white arrows). The false lumen of the AD (Figure 1D, white arrow) was not continued to that of the antecedent BCAD (Figure 1D, black arrow). Urgent ascending aortic replacement was successfully performed. Aortic arch replacement was not considered because previously-dissected BCA was not enlarged and no aortic entry was intraoperatively identified in the ascending or transverse aorta. A histologic examination of the resected aorta merely demonstrated slight medial myxoid changes. The postoperative course was uneventful. Repeated CT scans during the following 6 years indicated no significant change of the BCAD and the residual AD. Several patients with traumatic BCAD have been often reported (Supplementary References S1–S6). Spontaneous isolated BCAD, however, is extremely rare. Merely 12 cases^1–3^ (Supplementary References S7–S14) including the preset patient (see Supplementary material online, Table S1) were identified. Subsequent TA-AAD and preceding type-B acute AD occurred in three patients (including the present case)^1,2^ and one patient,^3^ respectively; i.e. a total of four patients (33.3%) complicated metachronous AD, which suggests some common aetiology between isolated BCAD and AD.
Supplementary Material
ytaf142_Supplementary_Data
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Oura K, Sato M, Yamaguchi Oura M, Itabashi R, Maeda T. Ischemic stroke due to spontaneous dissection of the brachiocephalic to the common carotid artery with a fatal course after expansion to the ascending aorta. Intern Med 2022;61:2483–2487.35110491 10.2169/internalmedicine.8931-21PMC 9449606 · doi ↗ · pubmed ↗
- 2Munakata H, Okada K, Tanaka H, Yamashita T, Nakagiri K, Okita Y. Acute dissection of the innominate artery: a case of report. Gen Thorac Cardiovasc Surg 2008;56:131–133.18340513 10.1007/s 11748-007-0205-8 · doi ↗ · pubmed ↗
- 3Kanady K, Hartz R, Massad M, Melen O, Russell E, Feingold R. Spontaneous isolated innominate artery dissection. Neurology 1990;40:1315–1317.10.1212/wnl.40.8.1315-a 2199850 · doi ↗ · pubmed ↗