Variations of partial anomalous pulmonary venous connection
Leqing Chen, Yukun Cao, Lixia Wang, Heshui Shi

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
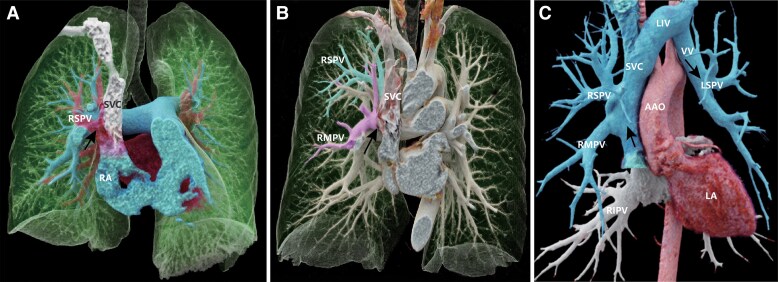 Figure 1
Figure 1 Figure 2
Figure 2- —Union Hospital10.13039/501100019230
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCongenital Heart Disease Studies · Pulmonary Hypertension Research and Treatments · Cardiovascular and Diving-Related Complications
Patient 1, a 50-year-old male with intermittent shortness of breath for 2 years (Figure 1A). CT pulmonary angiography revealed an anomalous connection between the right superior pulmonary vein (PV) and the superior vena cava (SVC), accompanied by mild pulmonary arterial hypertension (PAH) (Supplementary material online, Figure S1). The patient was managed conservatively and scheduled for regular follow-up examinations. Patient 2, a 59-year-old male, presented to our institution with bilateral lower limb oedema (Figure 1B). CT pulmonary angiography exhibited drainage of the right superior and middle PV into the SVC, along with PAH. Patient 3, a 40-year-old female, presented to our hospital complaining of chest tightness after exercise (Figure 1C). Transthoracic echocardiography revealed an enlarged right cardiac chamber and moderate tricuspid regurgitation. Subsequent CTPA demonstrated the left superior and lower PV draining into the left innominate vein, and the right superior and middle PV draining into the SVC. An atrial septal defect (ASD) was also detected, accompanied by severe PAH. This patient successfully underwent surgical correction.
Isolated PAPVC without ASD (Patient 1) as well as bilateral anomalous connection (Patient 3) are extremely rare anatomical findings. Partial anomalous pulmonary venous connection may develop symptoms such as PAH or right-sided volume overload depending on the number of abnormal connections.^1^ Compared to other existing studies, we visually present the relationship between different degrees of PAPVC and PAH.^2^ Although MRI enables Qp:Qs calculation and doesn't require iodine contrast administration, CTPA offers detailed anatomical information with high spatial resolution quickly and having broader availability. In cases of PAPVC without significant associated complications, regular follow-up with echocardiography to monitor pulmonary pressure and heart function is essential (Patients 1 and 2). For more severe cases involving ASD or severe PAH (Patient 3), surgical intervention may be considered to correct the anomalous connections and repair the septal defect.^3^
Supplementary Material
ytaf133_Supplementary_Data
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Sahay S, Krasuski RA, Tonelli AR. Partial anomalous pulmonary venous connection and pulmonary arterial hypertension. Respirology 2012;17:957–963.22509787 10.1111/j.1440-1843.2012.02180.x PMC 3409307 · doi ↗ · pubmed ↗
- 2Rajagopal R, Pandey NN, Sinha M, Sharma S. Cardiac type of partial anomalous pulmonary venous connection. Radiol Cardiothorac Imaging 2020;2:e 190100.33778536 10.1148/ryct.2020190100 PMC 7977932 · doi ↗ · pubmed ↗
- 3Hatipoglu S, Almogheer B, Mahon C, Houshmand G, Uygur B, Giblin GT, et al Clinical significance of partial anomalous pulmonary venous connections (isolated and atrial septal defect associated) determined by cardiovascular magnetic resonance. Circ Cardiovasc Imaging 2021;14:e 012371.34384233 10.1161/CIRCIMAGING.120.012371 · doi ↗ · pubmed ↗