The implementation of knowledge‐based planning with partial OAR contours for prostate radiotherapy
Ositomiwa O. Osipitan, David Wiant, Han Liu

TL;DR
This paper proposes using partial organ contours in prostate radiotherapy to reduce contour uncertainty and improve treatment planning.
Contribution
The novelty lies in using partial contours with knowledge-based planning to achieve dosimetry comparable to full contours.
Findings
Partial contours showed higher concordance compared to full contours in geometric evaluations.
RP_Part_Un plans reduced bladder doses in patients with SpaceOAR and rectum doses in those without.
MIM AI_Part_Un plans showed lower rectum doses in both patient groups.
Abstract
Intra‐ and inter‐observer contour uncertainty is a continuous challenge in treatment planning for radiotherapy. Our proposed solution to address this challenge is the use of partial contours for treatment planning, focusing on uninvolved or non‐overlapping portions of the organs‐at‐risk (OARs) with the planning target volume (PTV). The partial contours systematically eliminate overlapping regions. The partial contours were evaluated against fully contoured OARs. We incorporated advanced tools like knowledge‐based planning (KBP) to create treatment plans and artificial intelligence (AI) to create auto‐segmented contours. We developed two models, Rapid Plan (RP) and Rapid Plan partial uninvolved (RP_Part_Un), using 70 previous clinically approved volumetric arc therapy (VMAT) plans each prescribed with 70 Gy/28 fractions. From these models, we created three plans, RP, RP_Part_Un, and MIM…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
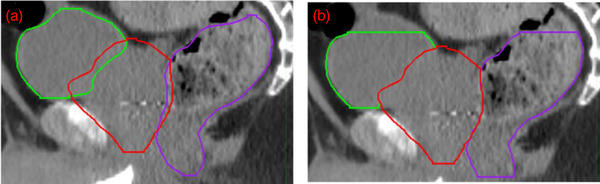 FIGURE 1
FIGURE 1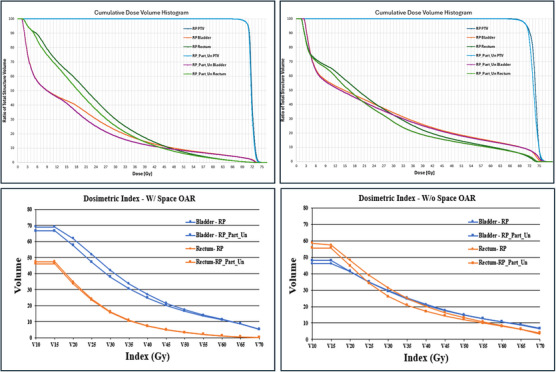 FIGURE 2
FIGURE 2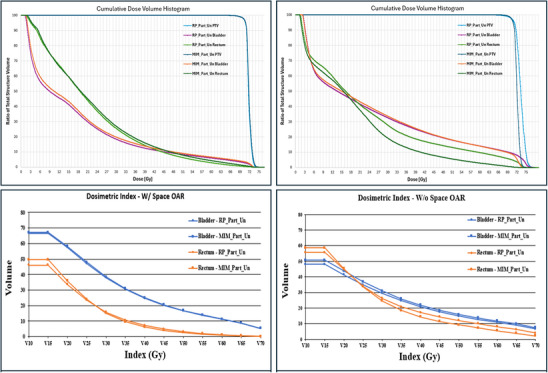 FIGURE 3
FIGURE 3| Full contours | Partial contours | |||
|---|---|---|---|---|
| DSC | OI | DSC | OI | |
| Bladder | ||||
| SpaceOAR | 0.92 ± 0.05 | 0.92 ± 0.05 | 0.96 ± 0.03 | 0.94 ± 0.06 |
| No SpaceOAR | 0.94 ± 0.02 | 0.95 ± 0.04 | 0.96 ± 0.02 | 0.96 ± 0.04 |
| Rectum | ||||
| SpaceOAR | 0.81 ± 0.05 | 0.78 ± 0.07 | 0.85 ± 0.04 | 0.85 ± 0.06 |
| No SpaceOAR | 0.79 ± 0.10 | 0.72 ± 0.14 | 0.86 ± 0.08 | 0.82 ± 0.11 |
| SpaceOAR | No SpaceOAR | |||||
|---|---|---|---|---|---|---|
| RP | RP_Part_Un | MIM AI_Part_Un | RP | RP_Part_Un | MIM AI_Part_Un | |
| Rectum | 64.82 ± 9.13 | 65.53 ± 8.42 | 64.45 ± 9.12 | 72.64 ± 5.77 | 74.72 ± 1.10 | 72.98 ± 2.69 |
| Rectum | 17.16 ± 3.84 | 16.95 ± 3.49 | 17.18 ± 3.36 | 24.11 ± 4.70 | 22.24 ± 4.56 | 21.84 ± 4.85 |
| Bladder | 73.04 ± 0.48 | 72.85 ± 0.44 | 72.92 ± 0.45 | 69.96 ± 16.40 | 72.77 ± 13.33 | 74.95 ± 1.07 |
| Bladder | 28.26 ± 8.29 | 27.21 ± 8.12 | 27.42 ± 8.23 | 20.85 ± 9.29 | 22.03 ± 8.13 | 23.21 ± 7.25 |
| SpaceOAR | No SpaceOAR | |||||
|---|---|---|---|---|---|---|
| RP | RP_Part_Un | MIM AI_Part_Un | RP | RP_Part_Un | MIM AI_Part_Un | |
| Left femur | 0.02 ± 0.10 | 0.19 ± 0.77 | 0.12 ± 0.32 | 1.56 ± 5.24 | 1.23 ± 4.37 |
0.16 ± 0.53 |
| Right femur | 0.02 ± 0.07 | 0.39 ± 0.98 | 0.49 ± 1.36 | 1.32 ± 6.88 | 0.29 ± 0.80 | 0.9 ± 1.97 |
| OAR/plans comparison |
|
|
|
|
|
|
|
| |
|---|---|---|---|---|---|---|---|---|---|
| Rectum ratio (RP_Part_Un/RP) | w/o space | 1.03 | 0.06 | 0.92 |
| 1.21 |
| 1.01 | 0.87 |
| space | 1.01 | 0.07 | 0.99 | 0.38 | 1.14 |
| 1.04 |
| |
| Rectum ratio (MIM AI_Part_Un /RP_Part_Un) | w/o space | 0.98 |
| 0.98 | 0.55 | 0.55 |
| 0.62 |
|
| space | 0.98 |
| 1.01 | 0.22 | 0.93 | 0.29 | 0.87 | 0.08 | |
| Bladder ratio (RP_Part_Un/RP) | w/o space | 1.04 | 0.48 | 1.06 | 0.50 | 1.02 | 0.83 | 1.02 | 0.85 |
| space | 1.00 |
| 0.96 |
| 0.98 |
| 0.98 |
| |
| Bladder ratio (MIM AI_Part_Un/RP_Part_Un) | w/o space | 1.03 | 0.38 | 1.05 | 0.12 | 1.12 | 0.06 | 1.10 | 0.08 |
| space | 1.00 | 0.31 | 1.01 |
| 1.02 |
| 1.01 |
|
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAdvanced Radiotherapy Techniques · Prostate Cancer Diagnosis and Treatment · Medical Imaging and Analysis
INTRODUCTION
1
Prostate cancer is the second most common form of cancer in men. Its incidence rate is continuously increasing among men, and contributing factors are increasing age population, ethnicity, and heredity.1, 2, 3, 4 Despite the increasing numbers, the mortality rates are low and decreasing.1, 2, 3, 4 Advancements in health care have allowed for better treatment over time. However, there are still some challenges. One of which, in the field of radiation therapy (RT), is the accuracy and efficiency of delineating anatomical structures, such as the target and organs‐at‐risk (OARs) during treatment planning. The challenge is to achieve precise delineation to ensure that radiation is delivered to the tumor while minimizing exposure to healthy tissues. Many factors can affect this success, including expertise, medical imaging interpretation, the understanding of human anatomy, knowledge of tumor characteristics, and individual anatomy variations. Inaccurate contouring could potentially lead to a reduction of the dose delivered to the tumor site, lower local control, and increased dose to OARs.
In radiation treatments, time to treat and contouring consistency are important aspects of the treatment process. From retrospective observational studies when a patient's RT treatment is delayed from first diagnosis to when treatment begins, local tumor recurrence is indirectly affected.5 When planning, accurate contouring of the OARs can be a time‐consuming component and can have large inter‐ and intra‐observer variabilities. For prostate cancer patients, the bladder and rectum are OARs that are typically of concern due to their close proximity to the prostate. Additionally, physiological filling or gas may contribute to differing sizes among individuals that lead to variations in delineation even by expert observers.6 Incorrect, inadequate, or over‐contouring of these OARs is a major source of error in RT delivery and can lead to poor normal tissue sparing and increased toxic effects.
Incorporating advanced tools like knowledge‐based planning (KBP) and artificial intelligence (AI) represents a pivotal step toward ameliorating issues‐concerning contouring consistency, and ensuring uniformity in contouring methodologies. KBP is based on a statistical model that estimates dose‐volume histograms (DVHs) and generates dose‐volume objectives that can be used for photon optimization from a library of clinically accepted plans with high quality. The benefits of using this technique, which include the reduction in plan quality variance and planning time, have been described previously.7, 8, 9, 10 Prostate is a highly investigated disease site using KBP methods.11, 12 Many have highlighted that KBP can create comparable or at times better dosimetric results than manually optimized plans.7, 8, 9, 10, 11, 12
The prominence of AI is steadily escalating within radiation oncology, responding to the evolving demands of a technically challenging field like radiotherapy. One area in which AI is implemented is contouring. These auto‐contouring applications could revolutionize radiotherapy treatments. Delineating radiotherapy target volumes and OARs is a key step in the treatment process. However, it is a very strenuous step that produces variability and can take a long time depending on the planner's experience and skills. The generalized benefits of auto‐contouring are decreased time required, improved quality, consistency, accuracy, and standardization.13, 14 RT in combination with AI as a proposed tool for auto‐contouring could potentially improve patient treatments.15
In this work, we present a novel solution based on partial OAR contouring that saves time and improves consistency for contours delineation and treatment planning. Partial OAR contouring is a technique where OARs are contoured only at a specified distance to a patient's planning target volume (PTV). In this study, we evaluated the efficacy of the partial uninvolved OAR technique using custom KBP models. To then refine and enhance the process we introduced AI. We created a separate plan utilizing AI contouring with our KBP model based on partial OARs uninvolved and contrasted it with the plans generated using the KBP model relying on manual full contours and a KBP model relying on manual partial uninvolved OARs.
METHODS AND MATERIALS
2
Patient selection
2.1
Sixty prostate patients with a prescription of 70 Gy/28Fx were chosen at random from a database of delivered treated plans to be retrospectively studied. They were anonymized and divided into two groups, 30 patients with a SpaceOAR, and 30 patients without SpaceOAR. Groups were created to see any potential advantages or disadvantages of our model in the presence of SpaceOAR. A SpaceOAR is an injectable rectal spacer made of polyethylene glycol (PEG).16
Partial uninvolved contours
2.2
The partial uninvolved OAR contours are constructed such that only OAR volumes on CT slices within 1 cm distance to the PTV edge superiorly and inferiorly are considered. The overlapping region with PTV is then removed in all dimensions. This was the case for both the bladder and rectum (Figure 1).
(a) Full planning target volume (PTV), bladder, and rectum contours. (b) Partial uninvolved bladder and rectum contours, that is, contours that are within 1 cm of the PTV in the superior–inferior dimension and do not overlap with the PTV.
KBP models and plans
2.3
We developed two KBP models, Rapid Plan (RP) and Rapid Plan partial uninvolved (RP_Part_Un), for this study (Varian Medical Systems, Palo Alto, CA, USA). RP, a commercially available version of KBP that has been described in previous works,17, 18 was used. Seventy previous clinically approved volumetric modulated arc therapy (VMAT) plans each prescribed with 70 Gy/28 fractions were used to develop the models. From these plans, full organ contours were defined for the RP model; while partial uninvolved contours were defined for the RP_Part_Un model. Using these models, three plans were then created and compared for each validation patient. All plans generated in this study have RP models based on PTV, rectum, bladder, and femoral heads, and all these structures were using for plan optimization. RP_Part_Un model and plan use partial uninvolved rectum and bladder structures. Plan 1 was named RP plan, which used the RP model and fully contoured structure set. Plan 2 was named RP_Part_Un plan, which used the RP_Part_Un model and partial uninvolved contour set. For further analysis, we implemented AI to see if any additional benefits were provided. MIM Contour ProtegeAI (MIM Maestro, Cleveland, OH) was used to perform AI‐based segmentation.19 Plan 3 was named MIM AI_Part_Un which used the RP_Part_Un model; however, AI segmentation was used to create the partial contours, unlike plan 2.
Plan evaluation
2.4
For determining OAR (bladder and rectum) sparing, D max and D mean along with the percent volume receiving a dose over a range (V 10 Gy–V 70 Gy) were compared. Percent volume receiving 40 Gy (V 40 Gy) was analyzed for both left and right femoral heads. These values were compared for the fully contoured plan (RP) against the partially contoured plan (RP_Part_Un). To ensure fairness in all dosimetric comparisons, entire OAR contours were used for all comparisons instead of partial contours. All plans were normalized so that 100% of the prescribed dose covered 98% of the PTV.
The MIM AI_Part_Un plan was subsequently compared to the RP_Part_Un plan for the select dosimetric indices mentioned previously. Geometric evaluations, dice similarity coefficient (DSC), and overlay index (OI) between the OAR contours from partial‐contoured manual structure sets and partial‐contoured AI structure sets were analyzed. Also, geometric evaluations for fully contoured manual structure sets and fully contoured AI structure sets were performed. Calculations for descriptive statistics included the determination of mean values and standard deviations. Student's t‐tests were done for quantitative comparisons, and two‐sided p‐values ≤ 0.05 were considered statistically significant.
RESULTS
3
As we studied the use of AI for contouring across both patient groups, we observed an increase in the similarity and accuracy of AI to the manual contours for the partial contours versus the full manual OAR contours (see Table 1). When comparing the DSC and OI for full contours to the partial contours, in patients with SpaceOAR, all comparisons showed significantly improved agreement for both organs. The same results were observed for patients without SpaceOAR. This indicates that there was a higher degree of concordance between the contours when only partial contours were considered.
Comparison between RP and RP_Part_Un
3.1
For patient groups with SpaceOAR, the D max and D mean of the bladder for RP_Part_Un plans, statistically, were significantly smaller than those for the RP plan (p ≤ 0.05), and no statistically different results were observed for D max and D mean for the rectum. For patient groups without SpaceOAR, there was a significant improvement on rectum D mean, and no differences were observed for rectum D max as well as bladder D max and D mean. All values are shown in Table 2.
TABLE 2: Average doses for rectum D max, rectum D mean, bladder D max, and bladder D mean for RP, RP_Part_Un, and MIM AI_Part_Un.
For the patient sample used in this study, the doses to both left and right femoral heads were less of a concern in the treatment planning process. As an example, the average volumes receiving 40 Gy (V40 Gy) are listed in Table 3 for both left and right femoral head. No significant differences (within 1%) were observed among all three plans for both SpaceOAR and non‐SpaceOAR patient groups.
TABLE 3: Comparisons of V 40 Gy for left and right femur heads.
As shown in Figure 2, for two representative patients over the percent volume range (V 10 Gy–V 70 Gy) compared to RP plans, the RP_Part_Un showed improved bladder dosimetry for the patient group with SpaceOAR, and improved rectum dosimetry for the patient group without SpaceOAR.
Comparison of RP and RP_Part_Un plans. Two representative patient DVHs with (top left) and without (top right) SpaceOAR and dosimetric comparisons (V 10–V 70) for space (bottom left) and no space (bottom right) OAR. DVH, dose‐volume histogram; OAR, organ‐at‐risk; RP, Rapid Plan; RP_Part_Un, Rapid Plan partial uninvolved.
Comparison between RP_Part_Un and MIM_Part_Un
3.2
For patient groups with SpaceOAR, the D max of the rectum was significantly lower for MIM AI_Part_Un plan. The D mean of the bladder was also significantly different; however, the RP_Part_Un plan was smaller. No statistically significant results were observed for bladder D max and rectum D mean. For patient groups without SpaceOAR, the D max of rectum was observed to be significantly lower for MIM AI_Part_Un. No statistically significant results were observed for rectum D mean as well as bladder D max and D mean. All values are shown in Table 2.
As shown in Figure 3, for two representative patients over the percent volume range (V 10–V 70) starting around V 30 Gy, compared to RP_Part_Un plans the MIM AI_Part_Un gave improved rectum dosimetry for both patient groups.
Comparison of RP_Part_Un and MIM AI_Part_Un plans. Two representative patient DVHs with (top left) and without (top right) SpaceOAR and dosimetric comparisons (V 10–V 70) for space (bottom left) and no space (bottom right) OAR. DVH, dose‐volume histogram; OAR, organ‐at‐risk; RP_Part_Un, Rapid Plan partial uninvolved.
The ratios of RP_Part_Un and RP, MIM AI_Part_Un and RP_Part_Un, for D max, D mean, V 70 Gy, and V 65 Gy are shown in Table 4 for the OARs (bladder and rectum).
TABLE 4: Parity comparison of dosimetric values obtained from plans. D max, D mean, V 70 Gy, and V 65 Gy were compared.
DISCUSSION
4
In our retrospective study, patients were separated into two groups, individuals with and without a SpaceOAR. The purpose of a SpaceOAR insertion into a patient is to create a physical separation of the rectum to the prostate, allowing for dose reduction to the rectum. Since the rectum in the SpaceOAR patients is typically displaced from the PTV compared to non‐SpaceOAR patients, these patients will have less overlap between the PTV and rectum, and so the use of partial contours should have less impact on plan quality. We observed for the SpaceOAR patients, no significant difference in D mean and D max for the rectum when between the RP and RP_Part_Un plans. Which is why little to no additional benefits were observed.
For patient groups with SpaceOAR, RP_Part_Un plans gave the D max and D mean values significantly smaller compared to RP plan for the bladder, and no significant dose difference observed for the rectum. For patient groups without SpaceOAR, compared to RP plans, we observed a significant improvement on rectum D mean, and no differences noticed for bladder D max and D mean for RP_Part_Un plans. For non‐SpaceOAR patient groups, the rectum is the closest OAR to the target and typically requires optimizer effort most in the planning process. Our study showed the partial uninvolved OAR volumes may give us superior dosimetry to the rectum in our patient sample. Similarly for patient group with SpaceOAR, less optimization effort will be spent on the rectum compared to the bladder, this is why we observed an improved bladder dosimetry from the partial uninvolved contours.
Previous works have been focused on using different geometric indices to quantify AI contour accuracy with varied results. However, the important matrix has been overlooked is the plan quality generated based on those AI contours. This work shows that MIM AI contours can be used to create high quality treatment plan. When the MIM AI_Part_Un plan was used for further comparison to the RP_Part_Un plan, the max dose for rectum was significantly lowered for both patient groups. A possible rationale for why a difference was seen in rectum D mean and D max but not bladder could be assumed from the geometric indices of the rectum. Rectum typically has a lower DSC and OI.6, 20, 21 Although we obtained higher indices when considering only the partially uninvolved volumes, the values for the rectum are lower and therefore have more of a possibility for variation in dose calculations. Due to its simplicity, this automated model could potentially be used in various other clinics.
We investigated reproducibility and the auto‐segmentation success via measuring DSC and OI. We observed that as we incorporated partial contours instead of the full contours the DSC and OI values increased (Table 1). The higher DSC and OI values that were observed can be attributed to the reduced range and limited CT images utilized for the delineation of the OAR contours. Inter‐observer variability has been shown in previous studies by organ volume measurement.22 Using the partial contour technique, the variation in volume for the OARs can be decreased. In theory, the more volume an expert observer has to contour, the more possibility for error and variation. So, a reduction of the volume to be contoured would reduce the likelihood of error and variation. When AI was introduced, it was shown to produce a more similar contour set with the manual plan when using the partially uninvolved model. This agrees with our theory that consistency can be improved by using partial contours. The degree of variation is reduced as the DSC and OI values increase as shown in Table 1. This is important in treatment planning because poor delineation can lead to toxicity to these normal tissues.
To compare how similar the dosimetric values for the OARs were between the plans, a ratio was done. In Table 4, in general, D max, D mean, V 70 Gy, and V 65 Gy were near the value of 1. This indicates that MIM AI_Part_Un and RP_Part_Un plans resulted in similar dosimetric values. The lowest values (0.55, 0.62) were observed when comparing the ratio of MIM AI_Part_Un to RP_Part_Un for average V 70 Gy and V 65 Gy, respectively, for rectum with no SpaceOAR patients. As we see in Figure 3, for the no SpaceOAR patients, at V 70 Gy and V 65 Gy we see a significant dose difference for MIM AI_Part_Un compared to RP_Part_Un. MIM AI_Part_Un calculated dose is nearly at zero while RP_Part_Un is nearly double that. This explains why the ratio was nearly half for V 70 Gy and V 65 Gy.
A possible limitation of this study is a quantitative measurement in which the plans could affect treatment planning time. Our assumption is that we expect using partial contours would result in time saving. As for AI segmentation, from plenty of previous studies, treatment planning time is improved with implementing AI contouring.15, 16, 23, 24, 25, 26 Another limitation is the application of this model on different OARs and other disease sites.
Our study illustrates a similar concept in which planners use clipped structures for plan optimization. Overlapping regions of OARs and PTV typically receive high dose and distanced regions receive low to no dose. The results demonstrate that focusing on contouring only OARs that are partial and within a specified range from the PTV has the potential to decrease treatment planning time, enhance consistency, minimize resource utilization, and achieve comparable doses for the PTV and OARs.
CONCLUSION
5
This work shows that the plan created with uninvolved partial contours to only a specified distance (1 cm) from the PTV provides comparable dosimetry to the plan created with fully contours. To further study the benefits of using uninvolved partial contours, an auto‐segmentation model was then used. The auto‐segmented model provides an equivalent result. This would additionally decrease treatment planning time and improve consistency. These results from this study would suggest AI partial contours can be implemented for treatment planning for prostate patients.
AUTHOR CONTRIBUTIONS
Ositomiwa O. Osipitan collected the data, performed the analysis, and drafted the manuscript. David Wiant assisted with the study design and drafted the manuscript. Han Liu designed the study, assisted with the data analysis, and drafted the manuscript.
CONFLICT OF INTEREST STATEMENT
This research was supported by a grant from Varian Medical Systems, Palo Alto, CA.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Wasim S , Lee SY , Kim J . Complexities of prostate cancer. Int J Mol Sci. 2022;23(22):14257. doi:10.3390/ijms 232214257 36430730 PMC 9696501 · doi ↗ · pubmed ↗
- 2Esserman LJ , Thompson IM , Reid B . Overdiagnosis and overtreatment in cancer: an opportunity for improvement. JAMA. 2013;10(8):797‐798. doi:10.1001/jama.2013.108415 23896967 · doi ↗ · pubmed ↗
- 3Hamdy FC , Donovan JL , Lane JA , et al. 10‐Year outcomes after monitoring, surgery, or radiotherapy for localized prostate cancer. N Engl J Med. 2016;375(15):1415‐1424.27626136 10.1056/NEJ Moa 1606220 · doi ↗ · pubmed ↗
- 4Amaloo C , Hayes L , Manning M , Liu H , Wiant D . Can automated treatment plans gain traction in the clinic? J Appl Clin Med Phys. 2019;20(8):29‐35. doi:10.1002/acm 2.12674 PMC 669876331313508 · doi ↗ · pubmed ↗
- 5Carvalho IT , Baccaglini W , Claros OR , et al. Genitourinary and gastrointestinal toxicity among patients with localized prostate cancer treated with conventional versus moderately hypofractionated radiation therapy: systematic review and meta‐analysis. Acta Oncol. 2018;57(8):1003‐1010. doi:10.1080/0284186 X.2018.1478126 29882448 · doi ↗ · pubmed ↗
- 6Zabel WJ , Conway JL , Gladwish A , et al. Clinical evaluation of deep leaning and atlas‐based auto‐contouring of bladder and rectum for prostate radiation therapy. Pract Radiat Oncol. 2021;11(1):e 80‐e 89. doi:10.1016/j.prro.2020.05.013 32599279 · doi ↗ · pubmed ↗
- 7Tamura M , Monzen H , Matsumoto K , et al. Mechanical performance of a commercial knowledge‐based VMAT planning for prostate cancer. Radiat Oncol. 2018;13:163. doi:10.1186/s 13014-018-1114-y 30170614 PMC 6119260 · doi ↗ · pubmed ↗
- 8Ueda Y , Fukunaga J , Kamima T , et al. Evaluation of multiple institutions’ models for knowledge‐based planning of volumetric modulated arc therapy (VMAT) for prostate cancer. Radiat Oncol. 2018;13:46. doi:10.1186/s 13014-018-0994 29558940 PMC 5859423 · doi ↗ · pubmed ↗