Early Supera stent fracture after treatment of popliteal artery occlusion caused by artificial knee joint: a case report
Yuki Shima, Narumi Taninobu, Kazunori Mushiake, Hiroyuki Tanaka, Kazushige Kadota

TL;DR
A case report describes an 86-year-old woman who experienced early Supera stent fracture in the popliteal artery, possibly due to proximity to an artificial knee joint and vascular abnormalities.
Contribution
This case highlights a rare early fracture of the Supera stent in the popliteal artery, potentially linked to artificial joint proximity and vascular anatomy.
Findings
Supera stent fracture occurred 6 months post-implantation in the popliteal artery.
Fracture site was near an artificial knee joint and a medially deviated artery, suggesting entrapment syndrome.
Endovascular treatment with balloon angioplasty was performed due to risks of additional stenting.
Abstract
The Supera stent, a self-expanding interwoven nitinol stent, has greater radial force than conventional stents, resulting in high patency and reduced stent fracture. There have been few reports of early stent fracture, and it is considered an effective device in the popliteal artery. We present a case of popliteal artery occlusion due to Supera stent fracture. An 86-year-old woman presented to our department with intermittent claudication after 6 months of Supera stent implantation. Ultrasonography demonstrated popliteal artery occlusion secondary to Supera stent fracture. Fluoroscopy revealed that the stent had fractured at the site closest to the artificial knee joint and might have been in contact with a vessel. In addition, the popliteal artery was slightly deviated medially in the P2 segment, suggesting popliteal artery entrapment syndrome. Because additional stenting was…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
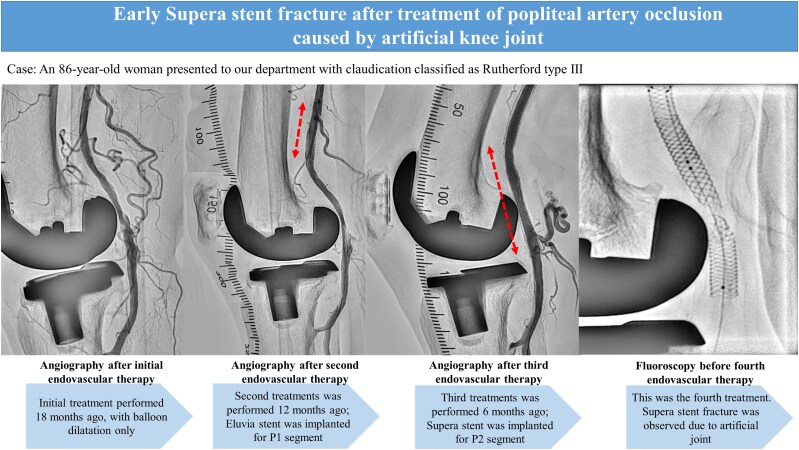 Figure 1
Figure 1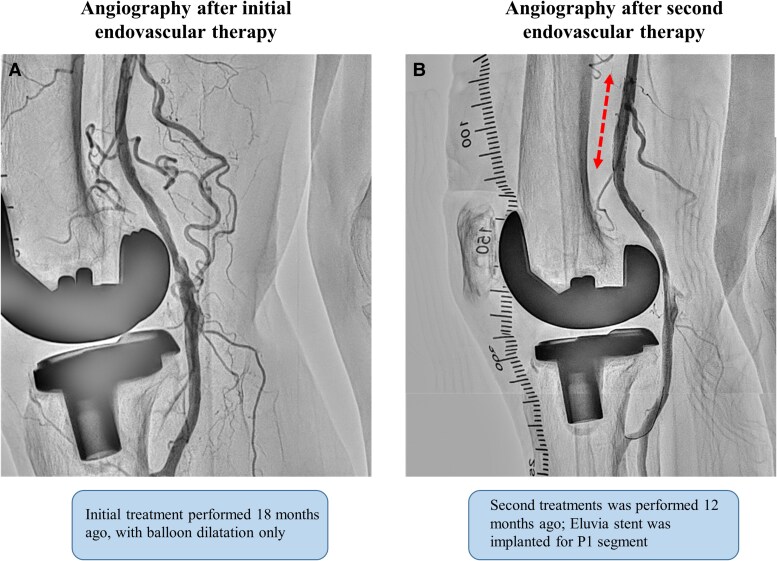 Figure 1
Figure 1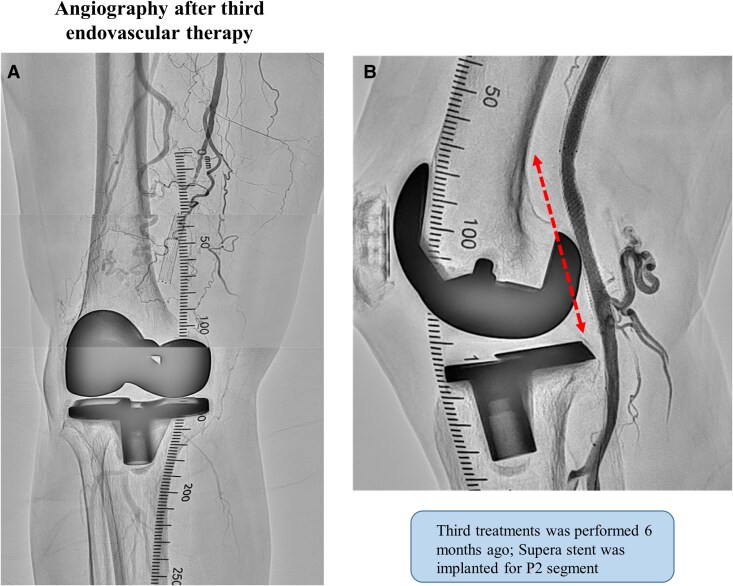 Figure 2
Figure 2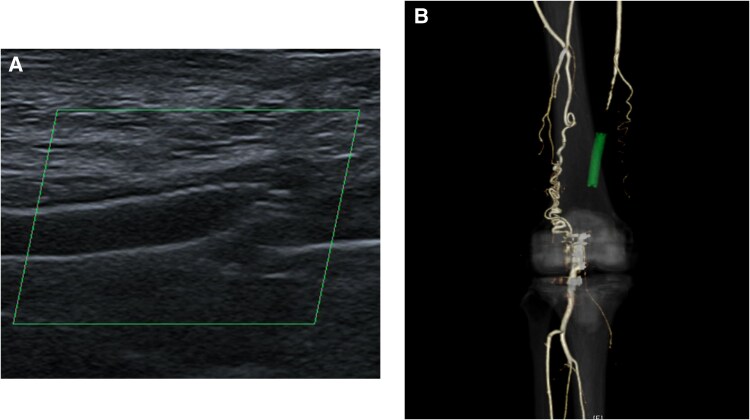 Figure 3
Figure 3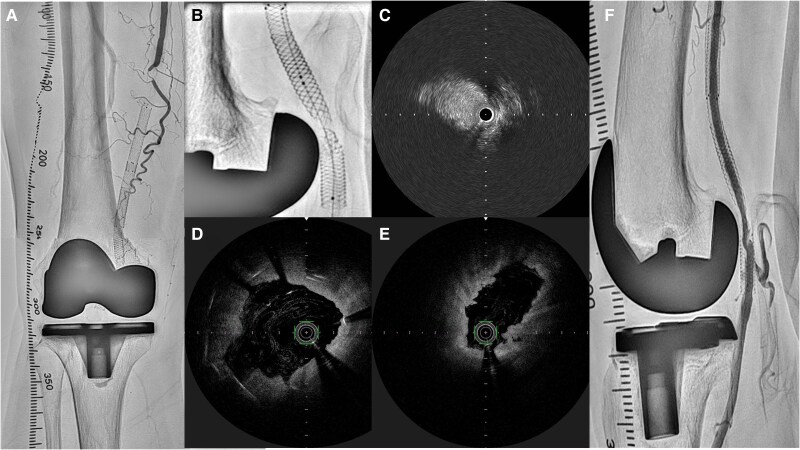 Figure 4
Figure 4Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPeripheral Artery Disease Management · Vascular Procedures and Complications · Muscle and Compartmental Disorders
Introduction
Owing to its repetitive flexion, the popliteal artery is a challenging anatomic site for the endovascular treatment of peripheral artery disease. The popliteal artery is considered a non-stenting zone because the mobility of the knee joint introduces additional dynamic forces into the vessel, resulting in accelerated restenosis and higher rates of stent fracture and occlusion. Therefore, the use of self-expanding nitinol stents in the popliteal artery has been avoided.^1^ The Supera stent (Abbott Vascular, Santa Clara, CA, USA) is a self-expanding interwoven nitinol stent that offers greater resistance to fracture and kinking, radial force, and flexibility than other self-expanding nitinol stents.^2^ As the Supera stent has been shown to have excellent primary patency and a low stent fracture rate at mid- and long-term follow-ups, popliteal artery stenting is becoming more common.^3,4^ As early Supera stent fracture is rare and has been scarcely reported, we present a case of popliteal artery occlusion due to Supera stent fracture at six months postoperatively.
Summary figure
**
Case presentation
An 86-year-old woman presented to our department with intermittent claudication classified as Rutherford type Ⅲ. She was diagnosed with peripheral artery disease because the right popliteal artery pulse was not palpable. She had hypertension, hyperlipidaemia, and a history of total knee arthroplasty years before the initial medical examination. Lower extremity ultrasonography revealed an occlusion of the P1 and P2 segments of the popliteal artery. The patient was an older adult and requested to be treated by endovascular therapy (EVT), which was performed using balloon dilation alone. (Figure 1A). However, at 6 months postoperatively, the patient redeveloped intermittent claudication symptoms. The distal part from the superficial femoral artery (SFA) to the P2 segment of the popliteal artery was re-occluded, and the patient requested another EVT to improve symptoms. During the second treatment, balloon dilation was performed, however, a large amount of thrombosis was noted at the distal part of SFA, and blood flow could not be obtained. Therefore, Eluvia 6.0 × 40 mm (Boston Scientific, Marlborough, MA, USA) stenting was performed in the distal SFA, and P1–P2 segments were dilated using Ranger 5.0 × 60 mm (Boston Scientific, Marlborough, MA, USA), as a drug-coated balloon (Figure 1B). The P2 segment was slightly poorly dilated, however, as the lesion was in a non-stenting zone, treatment was considered complete. However, at 6 months after the second endovascular treatment, the popliteal artery re-occluded and the patient redeveloped intermittent claudication symptoms. Therefore, a third endovascular treatment was performed. At this time, the lesion was also thrombotic, and the P2 segment was poorly dilated. Because of the possibility of another re-occlusion if the lesion remained poorly dilated, Supera stenting was performed with the patient’s consent to achieve long-term patency (Figure 2). Postprocedural intravascular ultrasound showed no evidence of stent compression.
First and second endovascular treatment (EVT) angiograms. (A) The first EVT was completed with balloon angioplasty only. (B) The second EVT was Eluvia stenting in the P1 segment and balloon angioplasty alone in the P2 segment.
Third endovascular treatment angiograms. (A) Occluded lesions over superficial femoral artery to popliteal artery. (B) Supera stent was deployed, and blood flow was good.
At six months following the third endovascular treatment, the patient returned to our department with intermittent claudication and loss of distal and popliteal pulses in the right lower limb. The patient’s intermittent claudication symptoms became progressively worse with each recurrence, and this time the symptoms appeared after ∼100 m of walking. Her ankle-brachial index was 0.66. Ultrasonography demonstrated popliteal artery occlusion secondary to Supera stent fracture (Figure 3A). The lesion repeatedly re-occluded, so a contrast-enhanced computed tomography scan was performed to evaluate the possibility of popliteal artery entrapment syndrome, which showed occlusion from the SFA to the popliteal artery despite the development of collateral blood channels (Figure 3B). Furthermore, angiography showed occlusion from the superficial artery to the popliteal artery (Figure 4A).
Imaging studies six months after the third endovascular treatment. (A) Ultrasonography demonstrated popliteal artery occlusion secondary to Supera stent fracture. (B) Contrast-enhanced computed tomography scan showed occlusion from the superficial femoral artery to the popliteal artery despite the development of collateral blood channels.
Imaging studies of the fourth endovascular treatment. (A) Angiography showed occlusion from the superficial artery to the popliteal artery. (B) Fluoroscopy showed Supera stent fracture at the site closest to the artificial knee joint. (C) Optical frequency domain imaging demonstrated Supera stent fracture with partial protrusion into the lumen and (D) areas not covered by the stent. (E) Intravascular ultrasound showed a lesion with low stent coverage and vessel dilation. (F) Final angiography confirmed blood flow, but vessel dilation was inadequate.
The fourth endovascular treatment was performed for popliteal artery occlusion. A 45-cm 6 F Destination guide catheter (Terumo, Tokyo, Japan) was inserted into the right common femoral artery via an antegrade approach. Fluoroscopy showed stent fracture at the site closest to the artificial knee joint, which appeared to be in contact with the vessel (Figure 4B). A 0.014-inch Gladius guidewire (Asahi Intecc, Seto, Japan) was supported by a Prominent Advance Neo 90-cm microcatheter (Tokai Medical Products, Kasugai, Japan) and successfully crossed the occluded lesion. Optical frequency domain imaging demonstrated Supera stent fracture with partial protrusion into the lumen and areas not covered by the stent, but no evidence of stent compression by the artificial knee joint (Figure 4C and D). Intravascular ultrasound showed a lesion with low stent coverage and vessel dilatation (Figure 4E). The lesion was dilated with a 3.0 × 40 mm JADE PTA balloon catheter (OrbusNeich Medical Tokyo, Japan) and a 5.0 × 40 mm Aperta PTA balloon catheter (Nipro, Osaka, Japan). Final angiography confirmed blood flow was re-established, but vessel dilation remained inadequate (Figure 4F). First and final angiography videos showed in Supplementary material. However, re-stenting could result in another stent fracture, therefore bypass surgery was considered. She was started on aspirin 100 mg/day and clopidogrel 75 mg/day as dual anti-platelet therapy. Other medications were pitavastatin 2 mg/day o.d. and azilsartan 10 mg/day o.d. These medications were taken regularly from the first to the last treatment. Because of repeated re-occlusion, the anti-platelet therapy plan was to continue dual anti-platelet therapy for at least one year. The patient’s symptoms did not improve and she requested surgical treatment, so bypass surgery was performed three months after the last EVT. The lesion showed good patency for the six months after bypass surgery.
Discussion
To our knowledge, this is the first case of early Supera stent fracture and there are two possible causes exist. First, the Supera stent may have fractured due to physical irritation caused by contact with the artificial knee joint. Optical frequency domain imaging and intravascular ultrasound showed no evidence of stent compression, but the stent fracture occurred in close proximity to the artificial knee joint; it is highly likely that the stent was physically affected by joint flexion or other stresses. Second, Supera stent fracture may have occurred due to popliteal artery entrapment syndrome. This is because the popliteal artery is repeatedly compressed by abnormal attachments of the gastrocnemius muscle or by abnormal muscles and fibre bundles in the popliteal fossa, resulting in impaired blood flow. It is more common in men under the age of 30 and may be especially common in athletes with high muscle mass.^5^ In this case, there were no abnormal attachments or abnormal muscle bundles in the popliteal fossa on the computed tomography scan, although they could not be fully evaluated due to artefacts from the artificial knee joint. The popliteal artery appeared to be slightly deviated medially in the P2 segment, and suggesting abnormal vascular running. The patient has atherosclerotic factors such as hypertension and hyperlipidaemia, but very mild atherosclerosis in the left lower extremity, aorta, and coronary arteries. Thus, the combination of abnormal vascular running and the artificial knee joint may have caused early Supera stent fracture. There are case reports of Supera stenting in an occluded popliteal artery with stent fracture.^6,7^ In this case, the risk of stent fracture was considered high even with additional Supera stenting, and no additional stenting was performed.
Even with the advent of the Supera stent, avoiding stenting in non-stenting zones remains common practice. However, there are situations in which stenting is unavoidable, such as thrombotic lesions and severe dissection. In addition, the strong radial force of the Supera stent is particularly useful in calcified lesions. Previous studies have reported that the Supera stent demonstrated good patency at two years without stent fracture^8^ and good patency at one year without stent fracture in popliteal artery lesions.^9^ In the BURDOCK study, the one-year and two-year patency rates of the Supera stent in calcified femoropopliteal lesions were 88.2% and 80.8%, respectively,^10^ suggesting that the Supera stent is a suitable device for femoropopliteal lesions.
Conclusion
The Supera stent is an excellent stent, however, avoiding popliteal artery stenting if a suspicion of abnormal vascular running or an artificial joint is observed may be prudent.
Supplementary Material
ytaf114_Supplementary_Data
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Laird JR, Katzen BT, Scheinert D, Lammer J, Carpenter MB, Dave R, et al Nitinol stent implantation versus balloon angioplasty for lesions in the superficial artery and proximal popliteal artery: twelve-month results from the RESILIENT randomized trial. Circ Cardiovasc Interv 2010;3:267–276.20484101 10.1161/CIRCINTERVENTIONS.109.903468 · doi ↗ · pubmed ↗
- 2Mac Taggart J, Poulson W, Seas A, Deegan P, Lomneth C, Desyatova A, et al Stent design affects femoropopliteal artery deformation. Ann Surg 2019;270:180–187.29578912 10.1097/SLA.0000000000002747 PMC 6151294 · doi ↗ · pubmed ↗
- 3Garcia L, Jaff MR, Metzger C, Sedillo G, Pershad A, Zidar F, et al Wire-interwoven nitinol stent outcome in the superficial femoral and proximal popliteal arteries: twelve month results of the SUPERB trial. Circ Cardiovasc Interv 2015;8:e 000937.25969545 10.1161/CIRCINTERVENTIONS.113.000937 · doi ↗ · pubmed ↗
- 4Garcıa LA, Rosenfield KR, Metzger CD, Zidar F, Pershad A, Popma JJ, et al SUPERB final 3-year outcomes using interwoven biomimetic Supera stent. Catheter Cardiovasc Interv 2017;89:1259–1267.28471091 10.1002/ccd.27058 · doi ↗ · pubmed ↗
- 5Sinha S, Houghton J, Holt PJ, Thompson MM, Loftus IM, Hinchliffe RJ. Popliteal entrapment syndrome. J Vasc Surg 2012;55:252–262.22116047 10.1016/j.jvs.2011.08.050 · doi ↗ · pubmed ↗
- 6Goltz JP, Ritter CO, Petritsch B, Kellersmann R, Hahn D, Kickuth R. Endovascular treatment of acute limb ischemia secondary to fracture of a popliteal artery stent. J Vasc Interv Radiol 2010;21:1739–1745.20920839 10.1016/j.jvir.2010.07.024 · doi ↗ · pubmed ↗
- 7Goltz JP, Ritter CO, Kenn W, Hahn D, Kickuth R. Immediate and complete stent collapse in the superficial femoral artery solved by implantation of a new helical nitinol stent. Cardiovasc Intervent Radiol 2011;34:S 307–S 311.20440499 10.1007/s 00270-010-9873-3 · doi ↗ · pubmed ↗
- 8Scheinert D, Grummt L, Piorkowski M, Sax J, Scheinert S, Ulrich M, et al A novel self-expanding interwoven nitinol stent for complex femoropopliteal lesions: 24-month results of the SUPERA SFA registry. J Endovasc Ther 2011;18:745–752.22149221 10.1583/11-3500.1 · doi ↗ · pubmed ↗