Correction: Journal of Epidemiology and Global Health (2024) 14:1490–1503 10.1007/s44197-024-00294-6
After the article was published, the authors identified a coding error that affected the estimates of zero-dose children in the Demographic and Health Surveys (DHS) data. Specifically, children who had died by the time of the survey were erroneously included in the measure of zero-dose children. This issue did not affect estimates derived from the Multiple Indicator Cluster Surveys (MICS). We have now corrected this error and provide updated tables and figures.
Despite these minor numerical adjustments, the conclusions of the study remain unchanged:
- Zero-dose prevalence has declined globally, with Gavi-eligible countries experiencing a significantly faster reduction.
- Reductions in zero-dose prevalence are associated with declines in postneonatal and child mortality, underscoring the importance of immunization efforts.
- Efforts should prioritize countries with high prevalence and number of zero-dose children to achieve Immunization Agenda 2030 targets.
The corrections resulted in minor changes to the estimated prevalence of zero-dose children in most countries. Importantly, all key findings remain robust, including:
- The sharp decline in zero-dose prevalence over time.
- The association between Gavi-eligibility and the change in zero-dose prevalence.
- The relationship between changes in zero-dose prevalence and changes in postneonatal and child mortality.
- The sensitivity analyses, as reported in the original supplement, were unaffected and continue to show similar results as the main analysis.
The overall prevalence in the most recent surveys was 12.4% after the correction (instead of 15.9%), with an average annual decline in prevalence of 0.7 pp (instead of 0.8 pp). The association between the change in postneonatal and child deaths per 1000 births and percentage point change in zero-dose prevalence was 1.2 deaths (instead of 1.4).
While the overall impact of the error was small, a few countries had noteworthy changes in the estimated prevalence of zero-dose children (listed here for the latest surveys):
- Sierra Leone: 9 percentage point (pp) change in prevalence.
- Liberia: 7 pp change.
- Chad, Benin, Nigeria, Burundi, Lesotho, and Haiti: 6 pp change.
- Malawi, Cameroon, Zambia, Mali, Zimbabwe, Guinea, Pakistan: 5 pp change.
Conclusion
The corrected analysis confirms that substantial progress has been made in reducing the percentage of children who have not received a DPT-containing vaccine. The main conclusions of the study remain unchanged:
- The prevalence of zero-dose children has declined globally, with Gavi-eligible countries experiencing a significantly faster reduction.
- A decrease in zero-dose prevalence is associated with a decline in postneonatal and child mortality, reinforcing the importance of immunization efforts.
- Efforts to reduce the number of zero-dose children should focus on countries with high prevalence and large populations of unvaccinated children to meet the Immunization Agenda 2030 targets.
Subsequently, Figs. 1, 2 and 3 and Tables 1, 2, 3 and 4 were corrected.Fig. 1. Distribution of zero-dose prevalence across countries by survey year. Note Only includes countries with two surveys. Percentiles 5 and 95 (line) and 25, 50, and 75 (box) are shown. Dots indicate country estimates. Each country’s estimate was weighted using sampling weights. Surveys were equally weighted for the median and percentiles. See Table 2 for tabulated estimates. Percentage point (pp) average annual change (AAC) is shown on the right side y-axisFig. 2The relationship between country-level zero-dose prevalence in the earliest survey and average annual percentage point (pp) change in prevalence. Note Pearson’s correlation coefficient (r) is shown. Countries were equally weightedFig. 3Correlation of zero-dose prevalence with health expenditure and postneonatal and child mortality rate. Notes The y and x-axes vary across graphs. GDP and health expenditure were measured per capita in PPP adjusted constant 2017 international .Pearson’scorrelationcoefficients(r)areshown.Postneonatalandchildmortalityrateisdeathsper1000livebirths.AACindicatesvariablesexpressedasaverageannual(absolute)change.CountrieswereequallyweightedTable 1Zero−doseprevalenceandestimatednumberofzero−dosechildrenSurveyyearPrevalence(. Postneonatal and child mortality rate is expressed as deaths per 1000 live births. Countries were equally weighted. Robust standard errors are shown in parentheses below coefficientsTable 4Difference between previously published estimates and corrected estimates of zero-dose prevalence in the latest DHS surveys (from Table 1)PublishedCorrectedDifference%%ppPooled16123.5East Asia and Pacific13111.9 Cambodia8.27.30.94 Indonesia13112.1 Myanmar16133.1 Papua New Guinea39363.4 Philippines15132.3 Timor-Leste26232.9Eastern and Southern Africa18153.5 Angola35323.3 Burundi6.90.935.9 Ethiopia33303.4 Kenya6.93.53.4 Lesotho8.32.16.2 Madagascar27234.3 Malawi7.62.84.8 Mozambique15123.5 Rwanda3.90.483.5 South Africa14113.0 Tanzania8.55.23.3 Uganda105.94.4 Zambia7.22.34.9 Zimbabwe17125.1Europe and Central Asia8.57.21.3 Armenia3.02.60.37 Tajikistan107.42.8 Türkiye119.41.7Latin America and Caribbean7.66.80.79 Guatemala5.12.03.0 Haiti25186.3Middle East and North Africa6.14.91.2 Egypt3.10.792.3 Jordan9.67.81.8South Asia128.63.8 Afghanistan35323.4 Bangladesh5.21.53.8 India106.73.4 Maldives119.31.3 Nepal8.56.12.4 Pakistan21155.4West and Central Africa31265.3 Benin22165.8 Burkina Faso9.15.93.2 Cameroon22174.9 Chad49435.7 Cote d’Ivoire34304.3 Gabon19162.9 Gambia6.52.14.4 Ghana6.13.52.6 Guinea42375.2 Liberia179.77.3 Mali23185.0 Mauritania16133.4 Nigeria42365.9 Senegal7.44.13.3 Sierra Leone155.89.0A correction was only done for estimates from DHS surveys. The overall Pearson’s correlation between the published and corrected estimates was over 0.98. A coding error caused estimates to include children who had died by the time of the survey. The corrected estimates exclude these children. Pooled estimates and estimates for global regions used all surveys (i.e., both MICS and DHS). Estimates were weighted using sampling weights rescaled to sum up the population 12–35 months old in the country and year of survey
The Original Article has been updated.

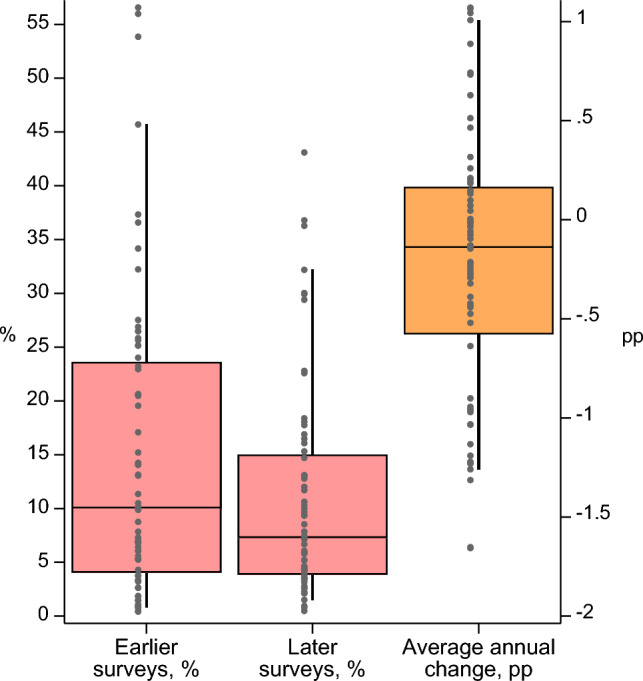 Figure 1
Figure 1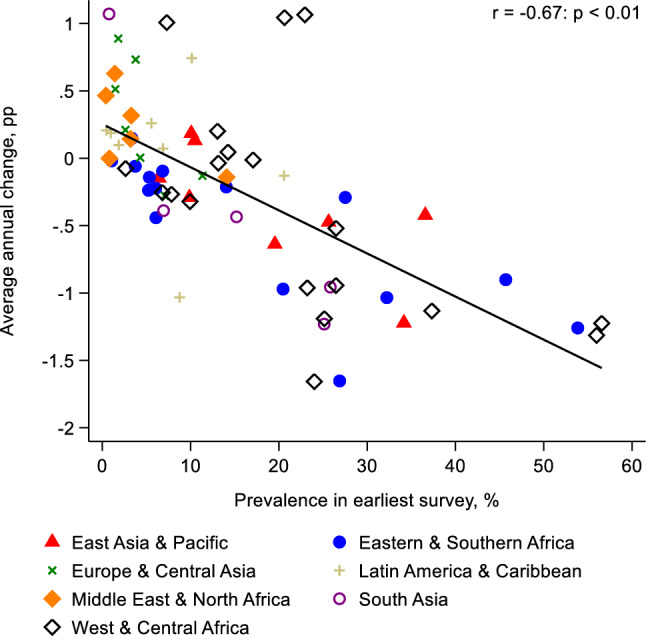 Figure 2
Figure 2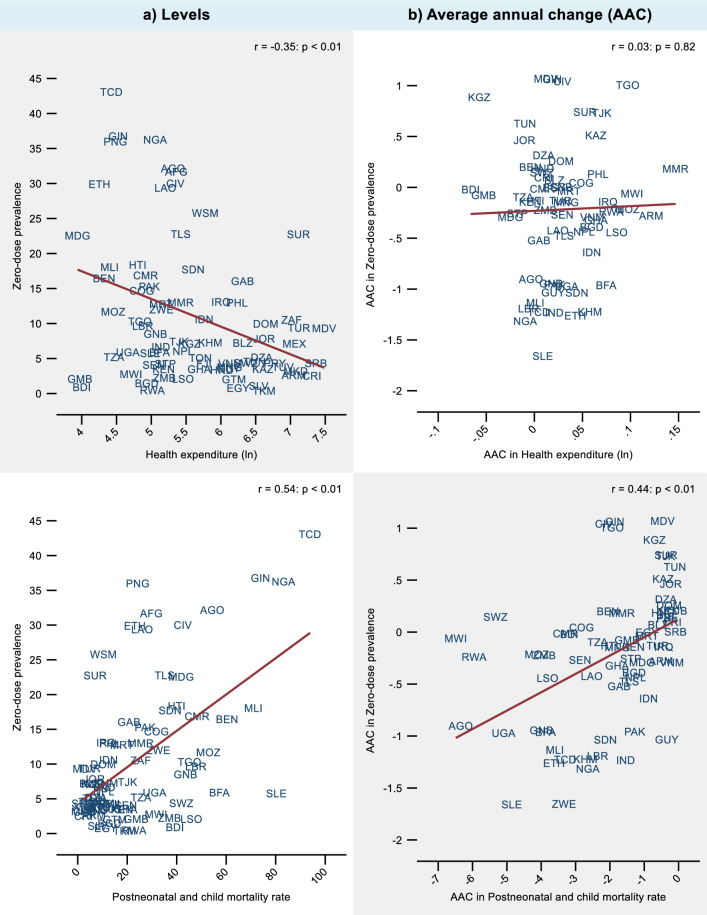 Figure 3
Figure 3