Impact of Antimicrobial Stewardship on Antimicrobial Utilization and Resistance Patterns in a Tertiary Care Hospital in Western Maharashtra
Neelam R Attar, Sara S Dhanawade, Divya Yadav, Jalandhar Nikam

TL;DR
This study shows that an antimicrobial stewardship program significantly reduced antibiotic use and resistance in a hospital in western Maharashtra.
Contribution
The study demonstrates the effectiveness of an AMS program in reducing antibiotic consumption and resistance in a private tertiary care hospital in India.
Findings
Antibiotic consumption decreased significantly after the AMS program was implemented.
Resistance to gentamicin, amikacin, and teicoplanin decreased following the intervention.
Culture-based therapy and surgical prophylaxis compliance improved substantially.
Abstract
Background: Non-judicious use of antibiotics by health professionals has been identified as an area for interventions and improvement by the World Health Organization for controlling antimicrobial resistance. Following the Indian Council for Medical Research (ICMR) guidelines, we established an antimicrobial stewardship (AMS) program at the 950-bedded multispecialty private sector hospital located in western Maharashtra by the end of the year 2021. Aim and objective: The purpose of this study was to evaluate the impact of an AMS program intervention on the utilization of antibiotics and resistance patterns of organisms isolated from the patients. Result: A significant reduction in the utilization of ceftriaxone (23.3 to 6.75), piperacillin-tazobactam (7.7 to 6.0), amikacin (9.03 to 5.15), clindamycin (6.25 to 5.75), linezolid (5.8 to 4.8), and ceftazidime (0.9 to 0.2) in defined daily…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
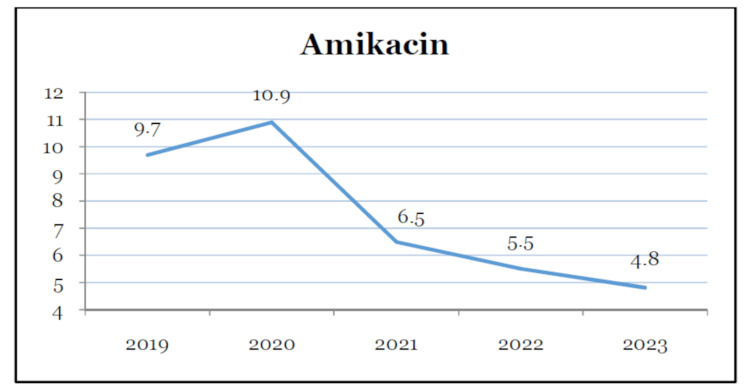 Figure 1
Figure 1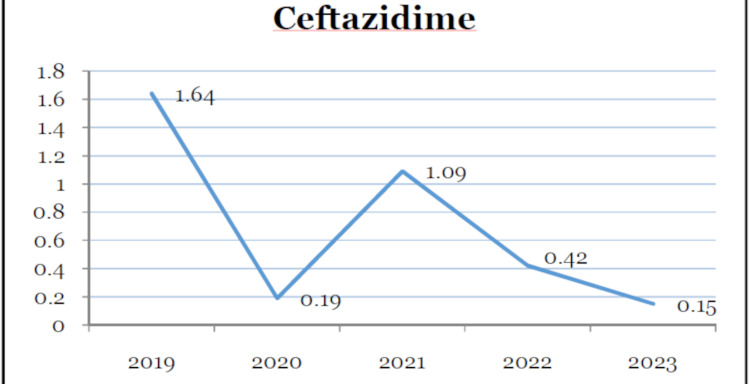 Figure 2
Figure 2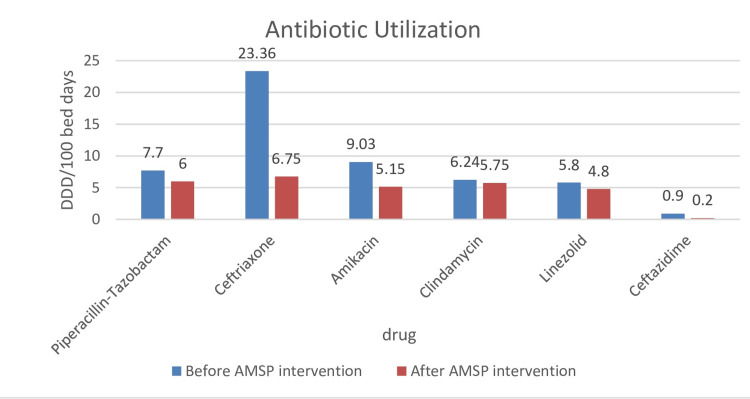 Figure 3
Figure 3| Drugs | 2019 | 2020 | 2021 | 2022 | 2023 |
| Piperacillin-tazobactam | 5.1 | 13.2 | 4.8 | 5.6 | 6.53 |
| Ceftriaxone | 13.4 | 27.7 | 29 | 3.4 | 10.1 |
| Ciprofloxacin | 0.45 | 0.41 | 0.31 | 0.32 | 0.39 |
| Imipenem | 0.1 | 0.09 | 0.01 | 0.08 | 0.08 |
| Gentamicin | 2.19 | 1.5 | 1.3 | 2.5 | 2.8 |
| Teicoplanin | 0.15 | 0.08 | 0.24 | 0.7 | 0.9 |
| Amikacin | 9.7 | 10.9 | 6.5 | 5.5 | 4.8 |
| Clindamycin | 3.94 | 6.74 | 8.05 | 5.4 | 6.1 |
| Linezolid | 4.9 | 6.4 | 6.3 | 4.3 | 5.3 |
| Meropenem | 3.2 | 4.4 | 3.8 | 3.4 | 5.5 |
| Vancomycin | 0.93 | 0.26 | 0.87 | 1.2 | 0.95 |
| Ceftazidime | 1.64 | 0.19 | 1.09 | 0.42 | 0.15 |
| Drugs | 2019 | 2020 | 2021 | 2022 | 2023 | |
| Escherichia coli | Piperacillin-tazobactam | 30 | 57 | 52 | 51 | 52 |
| Imipenem | 22 | 51 | 56 | 36 | 33 | |
| Meropenem | 2 | 42 | 55 | 35 | 34 | |
| Gentamicin | 48 | 44 | 58 | 38 | 40 | |
| Amikacin | 18 | 49 | 45 | 21 | 20 | |
| Ceftriaxone | 79 | 81 | 85 | 92 | 89 | |
|
| Piperacillin-tazobactam | 64 | 70 | 68 | 67 | 72 |
| Imipenem | 41 | 41 | 61 | 64 | 64 | |
| Meropenem | 55 | 55 | 59 | 61 | 68 | |
| Gentamicin | 38 | 38 | 58 | 57 | 57 | |
| Amikacin | 56 | 56 | 6 | 3 | 24 | |
| Ceftriaxone | 79 | 79 | 85 | 85 | 86 | |
|
| Piperacillin-tazobactam | 76 | 85 | 92 | 89 | 92 |
| Imipenem | 63 | 79 | 56 | 80 | 85 | |
| Meropenem | 38 | 87 | 55 | 79 | 88 | |
| Gentamicin | 81 | 92 | 72 | 76 | 82 | |
| Amikacin | 66 | 84 | 65 | 74 | 84 | |
| Ceftriaxone | 89 | 96 | 91 | 79 | 86 | |
|
| Piperacillin-tazobactam | 47 | 67 | 50 | 11 | 28 |
| Imipenem | 54 | 67 | 54 | 60 | 55 | |
| Meropenem | 53 | 68 | 50 | 64 | 56 | |
| Gentamicin | 42 | 43 | 50 | 59 | 50 | |
| Amikacin | 55 | 71 | 67 | 65 | 51 | |
| Ceftazidime | 36 | 64 | 32 | 14 | 30 | |
|
| Gentamicin | 45 | 63 | 51 | 40 | 31 |
| Clindamycin | 20 | 27 | 40 | 70 | 26 | |
| Teicoplanin | 10 | 9 | 6 | 5 | 4 | |
| Vancomycin | 2 | 18 | 11 | 9 | 8 | |
| Ciprofloxacin | 69 | 83 | 79 | 87 | 86 | |
| Linezolid | 30 | 28 | 48 | 55 | 28 | |
|
| Teicoplanin | 10 | 17 | |||
| Vancomycin | 3 | 35 | 30 | 42 | 23 | |
| Ciprofloxacin | 70 | 89 | 74 | 81 | 87 | |
| Linezolid | 8 | 13 |
| Organism | Drug | Spearman's correlation R | Significance | Result |
| Escherichia coli | Piperacillin-tazobactam | 0.5642 | 0.32172 | NS |
| Imipenem | -0.6668 | 0.2188 | NS | |
| Gentamicin | -0.8 | 0.10409 | NS | |
| Amikacin | 0.4 | 0.50463 | NS | |
| Meropenem | 0.3 | 0.62384 | NS | |
| Ceftriaxone | -0.6 | 0.2847 | NS | |
| Klebsiella | Piperacillin-tazobactam | 0.6 | 0.2847 | NS |
| Imipenem | -0.64889 | 0.23615 | NS | |
| Meropenem | 0.4616 | 0.4377 | NS | |
| Gentamicin | -0.1054 | 0.866 | NS | |
| Amikacin | 0.6668 | 0.2188 | NS | |
| Ceftriaxone | 0.9 | 0.0373 | S | |
| Acinetobacter | Piperacillin-tazobactam | -0.1539 | 0.8048 | NS |
| Imipenem | 0.0513 | 0.9347 | NS | |
| Meropenem | 0.9 | 0.03739 | S | |
| Gentamicin | 0.3 | 0.62384 | NS | |
| Amikacin | -0.1026 | 0.8696 | NS | |
| Ceftriaxone | 0.9 | 0.03739 | S | |
| Pseudomonas | Piperacillin-tazobactam | -0.1 | 0.87289 | NS |
| Imipenem | -0.1539 | 0.7998 | NS | |
| Meropenem | -0.3 | 0.6284 | NS | |
| Gentamicin | -0.3077 | 0.6143 | NS | |
| Amikacin | -0.7 | 0.18812 | NS | |
| Ceftazidime | -0.2 | 0.74706 | NS |
| Drugs | Before AMSP intervention | After AMSP intervention |
| Piperacillin-tazobactam | 7.7 | 6 |
| Ceftriaxone | 23.36 | 6.75 |
| Ciprofloxacin | 0.39 | 0.35 |
| Imipenem | 0.06 | 0.08 |
| Gentamicin | 1.66 | 2.65 |
| Teicoplanin | 0.15 | 0.8 |
| Amikacin | 9.03 | 5.15 |
| Clindamycin | 6.24 | 5.75 |
| Linezolid | 5.8 | 4.8 |
| Meropenem | 3.8 | 4.45 |
| Vancomycin | 0.68 | 1 |
| Ceftazidime | 0.9 | 0.2 |
| Drugs | Before intervention | After intervention |
| Piperacillin-tazobactam | 61.0% | 73.0% |
| Ceftriaxone | 84.8% | 86.3% |
| Ciprofloxacin IV | 77.3% | 86.0% |
| Imipenem | 49.7% | 56.0% |
| Gentamicin | 53.1% | 45.0% |
| Teicoplanin | 8.3% | 4.5% |
| Amikacin | 46.0% | 38.8% |
| Clindamycin | 29.0% | 38.0% |
| Linezolid | 35.3% | 41.5% |
| Meropenem | 48.3% | 56.0% |
| Vancomycin | 16.8% | 20.8% |
| Ceftazidime | 56.0% | 78.0% |
| Antimicrobial stewardship quality indicators | Before | After |
| Policy adherence indicators | ||
| Empirical antibiotics were as per policy | 73% | 96% |
| Surgical prophylaxis was as per policy | 58% | 96% |
| Administrative compliance indicators | ||
| Antibiotic was administered in the correct dose and duration | 83% | 93% |
| Culture-based antibiotic therapy used | 61% | 90% |
| Surgical antibiotic prophylaxis is given in the correct time frame | 79% | 98% |
| Antimicrobial usage outcome indicator | ||
| Overall antibiotic consumption | 1,681.0 DDD/100 bed days | 1,420.0 DDD/100 bed days |
| Irrational fixed-dose combination usage | 98.1 (9.3%) | 70.3 (4.8%) |
| AWaRe class | 2019 | 2020 | 2021 | 2022 | 2023 |
| Access | 519.8 (30.9%) | 275.9 (21.6%) | 475.2 (22.8%) | 213.9 (16.7%) | 437.1 (28.0%) |
| Watch | 1,078.8 (64.2%) | 938.4 (73.3%) | 1,437.7 (69.1%) | 1,007.4 (78.7%) | 1,027.8 (65.9%) |
| Reserve | 82.7 (4.9%) | 65.3 (5.1%) | 169.1 (8.1%) | 59.2 (4.6%) | 94.9 (6.1%) |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAntibiotic Use and Resistance · Patient Satisfaction in Healthcare · Pharmaceutical Practices and Patient Outcomes
Introduction
The global pandemic of antimicrobial resistance (AMR) has impacted every region of the world, jeopardizing the effectiveness of infection prevention and treatment. Almost 1.27 million deaths were attributed, and five million were associated with AMR in 2019, and now by 2050, the death toll is estimated to reach 10 million annually [1].
As per the World Health Organization (WHO) Bacterial Pathogen Priority List of 2024, carbapenem-resistant Enterobacterales, carbapenem-resistant Acinetobacter, cephalosporin-resistant Enterobacterales, and rifampicin-resistant Mycobacterium tuberculosis have been identified as the critical pathogens. The list highlights the impact of these pathogens in terms of burden, as well as issues related to transmissibility, treatability, and prevention options. It also guides stakeholders in research and development and investing in AMR [2].
India carries the largest burden of antibiotic-resistant organisms and is, hence, referred to as the AMR capital of the world [3]. Rising population, malnutrition, poverty, lack of access to healthcare, and lack of access to diagnostic facilities have all added to the ever-increasing problems of infectious diseases in the country. Drug resistance has been exacerbated by self-medication with broad-range antibiotics, easy access to over-the-counter medications, and medical professionals' careless use of antibiotics.
In 2015, WHO adopted the Global Action Plan for Antimicrobial Resistance (GAP-AMR) in collaboration with the Food and Agriculture Organization and the World Organisation for Animal Health. The plan provided five objectives for the member states to tackle the development of AMR. Phase 1 and Phase 2 of the National Action Plan were introduced by the Indian government in 2017 and 2022, respectively. In 2018, the Indian Council of Medical Research (ICMR) formulated the antimicrobial stewardship (AMS) program (AMSP) guidelines consisting of the main components of the application, which will reduce the effects of AMR [4]. Accreditation bodies collaborated by establishing an AMSP as a crucial component of the fundamental purpose. Following the guidelines, we established an AMSP at the 950-bedded multispecialty private sector hospital located in western Maharashtra by the end of the year 2021. An AMSP has been advocated as the most essential tool to combat AMR. It involves sensitizing healthcare staff, providing treatment guidelines, monitoring antibiotic prescription practices, and discouraging irrational antibiotic use through feedback. The purpose of this study was to evaluate the impact of AMSP intervention on the utilization of antibiotics and the resistance pattern of organisms isolated from the patients.
Materials and methods
A prospective analytical study was conducted on antimicrobial utilization and AMR from the year 2019 to 2023. The study included all patient care areas of a 950-bed tertiary care hospital. Our hospital consists of six intensive care units, seven surgical wards, four medicine and pediatrics wards, and four high-dependency units. As the interventions and recommendations were evidence-based and regarded as the standard of care, the Institutional Ethics Committee of Bharati Vidyapeeth (Deemed to be University) Medical College and Hospital, Sangli, approved this study (553/24) and waived the requirement for informed consent. Data was gathered both prior to and following the intervention (2019-2021).
CDC recommends seven core components in the implementation of AMSP [5]. They consist of hospital leadership commitment, where the hospital provides necessary human, financial, and information technology resources. Physicians and pharmacists will be accountable for program management and outcomes. The clinical pharmacist will lead implementation efforts to improve antibiotic use and apply infection-based, provider-based, pharmacy-based, microbiology-based, and nursing-based interventions. The impact of interventions will be tracked by monitoring antibiotic prescribing practices, the prevalence of Clostridioides difficile infection, and resistance patterns among hospital pathogens. Antibiotic prescribers and nurses will be provided with regular updates on antibiotic use and resistance. They will be educated on appropriate antibiotic-prescribing practices.
Based on these elements, our process of AMSP implementation began with the formation of an AMS committee by the end of the year 2021. It consisted of consultants from various departments, an infection control officer, a microbiologist, a pharmacologist, and five clinical pharmacists. The goals of the program were to promote the safe, effective, and rational use of antibiotics, slow down AMR by optimizing antibiotic use, and reduce overall healthcare costs.
In addition to the national recommendations, the AMS team and experts used the most recent antibiogram pattern to update the antibiotic policy. The clinical pharmacist, along with the microbiologist, conducted daily rounds in patient care areas. The first step was to look for what antibiotics were used for empirical therapy and whether it was in compliance with the antibiotic policy of the hospital. As preauthorization was not feasible with our setup, an antibiotic justification form was attached to the patient's file, and residents were asked to fill out forms within 24 hours of starting antibiotics. Forms were checked daily by microbiologists and clinical pharmacists during rounds. Consultants and residents were sensitized to using culture-based therapy. Antibiotic modifications (escalation or de-escalation) based on the culture report were monitored. Reminders for reviewing antibiotic continuation were given to consultants on day seven or 10. Consultants and residents were invited for a weekly meeting to discuss cases where antibiotic use was not justified. Additional details, including demographics, diagnosis, history of prior hospitalization and treatment, whether the infection was community- or hospital-acquired, and whether a gram-positive or gram-negative infection was suspected, were provided by the antibiotic justification form. Every quarter, AMSP meetings were held to discuss data pertaining to several AMS metrics. We began with readily attainable quality metrics like policy adherence indicators (adherence to policy, culture-based therapy, antibiotic choice, and timing for surgical prophylaxis), administrative compliance indicators (correct dose and duration of antibiotics), and antibiotic utilization indicators (defined daily doses (DDD)).
All consultants were given access to the quarterly AMS indicator data for improvement and feedback. Consultants, resident doctors, and nursing staff were sensitized frequently throughout the year through guest lectures, quizzes, and poster competitions. Antibiotic policy was provided in booklet form to each resident and consultant for easy access. A WhatsApp (Meta Platforms, Inc., Menlo Park, CA, US) group was created where the AMS team communicated several criteria for optimal antibiotic usage in order to improve communication between the team and consultants and residents. Infection control practices were simultaneously implemented. Through active surveillance and healthcare personnel training, appropriate steps were made to prevent hospital-acquired infections.
An antibiogram of six groups of organisms frequently isolated from the patient sample was included in the study. Escherichia coli, Klebsiella spp., Acinetobacter spp., Pseudomonas spp., Staphylococcus spp., and Enterococcus spp. were monitored for five years for resistance patterns. The following isolates were excluded from the study: (a) isolate from surveillance and (b) repeat isolate from the same sample.
Conventional methods were used to process the patient's sample, and VITEK 2 (bioMerieux, Marcy-l'Étoile, France) was used to identify the organism. Minimum inhibitory concentration (MIC) results were interpreted using Clinical Laboratory Standards Institute guidelines [6]. Antibiogram patterns of each of these isolates were analyzed at the end of the year. The antibiogram pattern was stratified depending on the type of isolates, source, and area and circulated as an annexure in the antibiotic policy for the consultant’s information.
To calculate antibiotic consumption, we retrospectively collected data from medical records and pharmacy software data. The Anatomical Therapeutic Chemical (ATC)/DDD is a universal parameter suggested by WHO for calculating the antibiotic utilization of every antibiotic and combination [7]. The usage of antibiotics was calculated by using the ATC/DDD per 100 bed days. The prescribed antibiotics were also classified based on the Access, Watch, and Reserve (AWaRe) classification. Additional data consisting of the use of irrational drug combinations was also extracted. The antibiotics that fall under the ATC classification but were dispensed to the outpatient and treatment after discharge were excluded from the study. Microsoft Excel 2021 edition (Microsoft Corp., Redmond, WA, US) was used to organize and clean the imported and calculated data.
After five years of monitoring the use of common antibiotics (piperacillin-tazobactam, ceftriaxone, ciprofloxacin, imipenem, gentamicin, teicoplanin, amikacin, clindamycin, linezolid, meropenem, vancomycin, and ceftazidime), the patterns of resistance were compared to the use of these antibiotics. Statistical analysis was done using Microsoft 365 (Microsoft Corp., Redmond, WA, US) and IBM SPSS - 29 (IBM Corp., Armonk, NY, US). Descriptive statistics and Spearman rank correlation were applied.
Results
Table 1 provides antibiotic utilization in DDD/100 bed days over a period of five years. The overall consumption of all antimicrobials differed throughout the study period. There was a gradual reduction in the utilization of amikacin and ceftazidime (Figures 1, 2). Ceftriaxone was the highest consumed antibiotic for three consecutive years before AMSP intervention. The utilization reduced drastically after the year 2022. Piperacillin-tazobactam was also the highest consumed drug in the year 2020. The usage reduced afterward. The utilization reduced in the years 2022 and 2023.
Decreasing trend of amikacin utilization over the five-year period
Decreasing trend of ceftazidime utilization (DDD/100 bed days) over the five-year periodDDD: defined daily dose
We analyzed the resistance pattern of E. coli, Klebsiella, Acinetobacter spp., Pseudomonas spp., Staphylococcus spp., and Enterococcus over a period of five years from 2019 to 2023 (Table 2). Among all the isolates analyzed over five years, E. coli (29%) was the most frequently isolated organism every year, followed by Klebsiella spp. (22%), Staphylococcus (16%), Acinetobacter (12%), Pseudomonas (11%), and Enterococcus spp. (8%). E. coli showed a reducing resistance for ceftriaxone from 92% to 89% in the years 2022 and 2023. Imipenem, meropenem, amikacin, and gentamicin resistance in E. coli decreased during the AMSP intervention in the years 2022 and 2023. Resistance of *Klebsiella *to ceftriaxone, piperacillin-tazobactam, and carbapenem has remained the same in all five years. Resistance to gentamicin has increased since 2021. There is a significant dip in the amikacin resistance pattern during the years 2021 and 2022 (from 56% to 24%). Acinetobacter shows an initial decrease in resistance to meropenem, imipenem, gentamicin, and amikacin for the year 2021, followed by an increase in resistance for the years 2022 and 2023. Resistance to piperacillin-tazobactam has remained almost the same for five years. There is no significant change in the resistance pattern of Pseudomonas to imipenem, meropenem, gentamicin, and amikacin. Ceftazidime and piperacillin-tazobactam showed a reduction in resistance in the years 2021 and 2022. Seventy percent of isolates were methicillin-resistant Staphylococcus aureus (MRSA) during all five years. Gentamicin and vancomycin initially showed high resistance in the year 2020, followed by dropping resistance in the following years. Staphylococcus has constantly shown high-level resistance to fluoroquinolones in all five years. Linezolid and clindamycin resistance has increased in 2021 and 2022 and dropped to 28% in 2023. Enterococcus has shown high resistance to ciprofloxacin in all years. Vancomycin resistance increased in the year 2022. Twenty-five percent of isolates of Enterococcus were vancomycin-resistant (VRE) in all five years.
Spearman's correlation was used to identify the correlation between antibiotic utilization and resistance among the isolates (Table 3). Spearman’s rank correlation is used to check whether the utilization of antibiotics and resistance are correlated. The correlation value R greater than or equal to 0.8 is a strong correlation. A minus sign indicates a negative correlation, and no sign is a positive correlation.
There is a high positive and significant correlation for ceftriaxone in Klebsiella and Acinetobacter (R = 0.9, p = 0.03739). It indicates that an increase in utilization increases resistance. This also stands true for meropenem in Acinetobacter.
A significant reduction in the utilization after AMSP intervention was observed in ceftriaxone, piperacillin-tazobactam, amikacin, clindamycin, linezolid, and ceftazidime (Table 4 and Figure 3). Antibiotic resistance decreased in gentamicin, amikacin, and teicoplanin following AMSP intervention (Table 5).
Utilization of antibiotics before and after intervention (defined daily doses (DDD)/100 bed days)AMSP: antimicrobial stewardship program
As an additional finding, AMS quality indicators were also monitored simultaneously during interventions. Policy compliance reached 96% after interventions. There is remarkable improvement in the administration of the correct dose and duration of antibiotics. The practice of culture-based treatment increased from 61% to 90%. Overall antibiotic consumption, which was 1,681.0 DDD/100 bed days before intervention, dropped by 15%. As irrational drug combination usage was also discouraged, a reduction of 28% was also observed (Table 6).
Antibiotic utilization as per the AWaRe classification was analyzed (Table 7). Watch group antibiotics form the major component of the antibiotic class used. Access group antibiotic utilization ranged between 30% and 28% during all five years.
Discussion
AMS has long been identified as an essential tool to ensure appropriate antibiotic usage among healthcare personnel and the general population. Rather than using restrictive measures as suggested in studies [8], we intended to bring behavioral changes through regular communication with the consultants on a case-by-case basis. Senior consultants from medicine and pediatrics provided counseling for antibiotic modifications. Feedback was also provided through structured feedback forms. These actions increased the postgraduate students' confidence in their ability to use antibiotics appropriately. Over time, postgraduate students and consultants began to rely on clinical pharmacists and microbiologists to recommend antibiotics. In several antibiotics, loading doses that were overlooked were also fixed. The majority of studies on antibiotic consumption conducted so far have been point prevalence studies. We were able to assess the long-term effects of AMSP interventions on physicians' behavior thanks to our five-year study.
India ranked first in antibiotic consumption from 2000 to 2010 [9]. Broad-spectrum antibiotics like fluoroquinolones, cephalosporins, and macrolides were frequently used for both inpatient and outpatient cases. Ceftriaxone was the most abused cephalosporin in our hospital while being the most affordable and accessible medication. Ceftriaxone was given to patients with viral diseases such as dengue, malaria, and IC bleeds due to a lack of knowledge and unidentified fear. Ceftriaxone misuse was also observed in a study by Jabeen et al. [10]. We were able to cut its usage by about 71%, from 23.36 DDD/100 bed days to 6.75 DDD/100 bed days. For surgical prophylaxis, surgeons typically used amikacin in combination with cephalosporin. Since amikacin was a tuberculosis (TB) reserve medication, we discouraged its use and saw a 42% reduction. During the two critical years of the COVID-19 epidemic, piperacillin-tazobactam was widely provided as advised by the Ministry of Health. By the end of 2021, it was a routine practice to treat each and every respiratory tract infection with piperacillin-tazobactam. Our hospital provided the physicians with different diagnostic modalities, which could help them differentiate viral cases of pneumonia (polymerase chain reaction (PCR) respiratory panels). These measures not only reassured the physicians but also contributed to a decrease in the use of piperacillin-tazobactam. Overall consumption of all antibiotics dropped by 15% after two years of AMSP intervention.
With the reduced use of ceftriaxone over the five-year period, a reduction in resistance among E. coli isolates was seen. There was no change in ceftriaxone resistance in Klebsiella, though Klebsiella spp. showed decreased resistance to amikacin following reduced consumption. Our hospital, being a tertiary care center, receives antibiotic-exposed and referred patients for further management. This amplified the burden of multidrug-resistant organisms (MDROs) such as Acinetobacter, Pseudomonas, and MRSA. There was no significant change in the resistance pattern of Acinetobacter, Pseudomonas, and S. aureus over the five-year period. When the average pattern of resistance to gentamicin, teicoplanin, and amikacin was compared before and after the intervention, it showed a big drop.
As evident from other studies [11-13], we could find a similar positive correlation between antibiotic utilization and resistance. The correlation was statistically significant only for ceftriaxone use in *Klebsiella *and Acinetobacter and meropenem in Acinetobacter. Studies by Laxminarayan and Chaudhury [14] have suggested multifactorial causes in the development of AMR, consumption being only one of the factors.
To evaluate the effects of our two years of interventions, we looked at a number of indicators. The parameters included loading dose, maintenance dose, frequency, duration of therapy, de-escalation and escalation, rational fixed-dose combination (FDC) usage, culture-based therapy, policy adherence for empirical therapy, treatment change based on AMS team suggestion, IV to oral switch, and medication interactions.
The areas where aggressive intervention was still needed were de-escalations of antibiotic class. The compliance for de-escalation was better with the surgical department. Patients were given IV antibiotics for two to three days and then shifted down to oral antibiotics as per policy recommendations. We could not achieve significant de-escalation in critical care units, the reason being the majority of patients were previously treated with higher antibiotics already. They were colonized or infected with MDRO strains. This led to prolonged treatment with high-end antibiotics and an inability to de-escalate.
We achieved a significant improvement in the administration of the loading dose (93% compliance) as against the results seen in the study by Singh et al. [15], where compliance was very low (38%) for meropenem and polymyxin B. Loading doses for drugs like polymyxin B, colistin, tigecycline, and vancomycin were added in the policy for reference. The use of colistin, polymyxin B, and tigecycline started in the year 2022. These drugs were utilized as last-resort measures to treat carbapenem-resistant organisms. We initiated sensitization through interactions with treating physicians during daily rounds and provided them with literature for reference. Corrections were suggested in both loading and maintenance doses wherever required.
The use of dual antibiotics with an overlapping spectrum and dual-anaerobic cover was a frequent observation before intervention. The practice was more prevalent in surgical departments. Interventions by the AMS team did result in behavioral changes among the prescribing consultants, leading to a reduction in use.
According to a study by Koya et al. [16], a huge number of antibiotics are not permitted by central drug regulators, and a considerable portion of the Indian population takes FDC from formulations outside the National List of Essential Medicines (NLEM). We have reduced the usage of illogical FDCs in our hospital by sensitizing prescribers and routinely revising the hospital drug formulary in accordance with the NLEM list.
Culture-based therapy was not a standard practice in the hospital before AMSP. Only 60% of patients were treated using culture-based antibiotics. There was excellent compliance among pediatricians to use targeted therapy and modify empirical choice based on culture reports. Compliance was extremely low among medicine, surgery, orthopedics, and ENT. This scenario was more or less the same in other hospitals around the globe, as evident from various studies [17,18]. The AMS team at our hospital trained the residents and consultants on diagnostic stewardship. Residents were encouraged to assess the need to send samples during daily rounds. Residents were provided with an MIC guiding table for antibiotic selection and VITEK AST report interpretation. We increased the practice of targeted therapy from 60% to 90% postintervention.
Swamy et al. [19] employed a patient risk stratification model to identify patients at risk of having MDRO pathogens. The majority of patients in his study belonged to risk groups 2 and 3 that were already exposed to antibiotics. This justified the use of higher antibiotics and also reduced the chances of group 1 patients receiving higher antibiotics. Instead of using the risk stratification model to identify patients with MDRO, we screened previously hospitalized patients for bloodstream infections, urinary tract infections if catheterized, and respiratory tract infections if ventilated on day one of admission. Patients who were only colonized and not infected with MDRO were isolated, closely monitored, and treated as per policy for antibiotic-naïve patients. Those with true infections received higher antibiotics as per antibiotic susceptibility reports.
WHO introduced the AWaRe classification in the year 2017 to support AMS efforts at local, national, and global levels. WHO's 13th General Program of Work 2019-2023 recommended that countries should have 60% of total antibiotic consumption from the Access group of antibiotics, and the ratio of Access to Watch should be close to 1.5 [20]. The ratio seen in our study throughout the five years was 0.4, 0.2, 0.3, 0.2, and 0.4, respectively, which was far from the recommendation. There were similar observations seen in other studies conducted in India [21,22]. With a high prevalence of extended-spectrum beta-lactamases (ESBLs), AmpC co-producers, carbapenem-resistant Enterobacterales, and Acinetobacter in our hospital, the Watch group of antibiotics remained the only option to treat patients. The issue of resistant organisms in India is evident from various studies conducted so far [23]. Both ICMR and the National Centre for Disease Control (NCDC) have reported alarming levels of resistance among E. coli and Klebsiella for third-generation cephalosporins, fluoroquinolones, carbapenems, and beta-lactam/beta-lactamase inhibitor combinations in the 2022 annual report [24,25].
As indicated by Sahani et al.'s [26] findings in their study, there is a paucity of AMSP intervention studies that include an education component as an important measure to strengthen stewardship activities. In order to encourage students to engage, we placed a strong emphasis on regular trainings for undergraduates and offered AMSP and hospital infection control as elective postings. Hospital infection control, diagnostic stewardship, sample collection and transportation techniques, and AMS were among the specific subjects covered in the introduction training given to postgraduate students.
Limitations of the study
As we used three years of AMSP preintervention data and compared it with two years of postintervention, we had to ensure uniformity in the antibiotics studied throughout the period. Antibiotics like colistin, tigecycline, and polymyxin B were neither tested nor used till the year 2022. Hence, we could not include the consumption of these antibiotics in our study. Issues like antimicrobial cycling, dose optimization, and cost calculations were not addressed in this study. Area-wise consumption of antibiotics from the critical care unit and wards was not looked into in the present study. Clinical outcome indicators (morbidity and mortality) also were not addressed.
Conclusions
The constant perseverance of the AMS team of our hospital had a positive impact on reducing the overall consumption of antibiotics by 15%. We brought down the utilization of ceftriaxone by 71%, amikacin by 42%, piperacillin-tazobactam by 22%, clindamycin by 8%, and linezolid by 17%. There was a decrease in resistance seen in E. coli for ceftriaxone and Klebsiella for amikacin. There was a positive correlation seen between the utilization of ceftriaxone and resistance among Klebsiella and Acinetobacter. A similar correlation was also seen in Acinetobacter for meropenem. Antibiotic policy adherence improved by 31%, surgical prophylaxis compliance by 65%, and culture-based therapy by 47%. The use of irrational FDC was reduced by 22%.
Rational use of antibiotics in humans, animals, and farming plays a major role in slowing down the ever-evolving AMR. While the government takes regulatory action at all other levels, it is the ethical responsibility of the treating physicians to use antibiotics judiciously. Stringent infection prevention and control practices, timely provision of treatment guidelines, frequent interactions and discussions with treating doctors, audits by clinical pharmacists, and feedback to the doctors along with various training programs and sensitization sessions by the AMS team have brought significant behavioral changes among the treating physicians.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1World Health Organization (WHO). Antimicrobial resistance 2 2025 2023 https://www.who.int/news-room/fact-sheets/detail/antimicrobial-resistance
- 2World Health Organization. WHO bacterial priority pathogens list, 2024: bacterial pathogens of public health importance to guide research, development and strategies to prevent and control antimicrobial resistance 2 2025 2024 https://www.who.int/publications/i/item/9789240093461
- 3Antimicrobial resistance: the next BIG pandemic Int J Community Med Public Health Chaudhry D Tomar P 2632263642017
- 4Indian Council of Medical Research. Antimicrobial stewardship program guidelines 1 2025 2018 https://www.icmr.gov.in/icmrobject/custom_data/pdf/resource-guidelines/AMSP_0.pd
- 5CDC. Core Elements of Hospital Antibiotic Stewardship Programs. Atlanta, GA: US Department of Health and Human Services, CDC Core Elements of Hospital Antibiotic Stewardship Programs 1 2025 CDCCDC Atlanta, GAUS Department of Health and Human Services, CDC 2019 https://www.cdc.gov/antibiotic-use/healthcare/pdfs/hospital-core-elements-H.pdf
- 6Clinical and Laboratory Standards Institute. M 100 Performance Standards for Antimicrobial Susceptibility Testing A CLSI supplement for global application. 30th Edition [Internet].Performance Standards for Antimicrobial Susceptibility Testing 1 2023 CLSICLSI Wayne, PA Clinical and Laboratory Standards Institute 2020 https://www.nih.org.pk/wp-content/uploads/2021/02/CLSI-2020.pdf
- 7WHO Collaborating Centre for Drug Statistics Methodology. New ATC/DD Ds and alterations included in the index of 2023 ATC/DDD Index 2023 https://atcddd.fhi.no/news/new_atc_ddds_and_alterations_included_in_the_index_of_2023
- 8Factors associated with adherence to antimicrobial stewardship after-hours Int J Pharm Pract Mostaghim M Snelling T Bajorek B 1801902720193028117810.1111/ijpp.12486 · doi ↗ · pubmed ↗