A Unique Case of Disseminated Cutaneous Coccidioidomycosis Years After Initial Infection
Mason Seely, Christina W Sun, Christopher Smith, Nicole R Bender

TL;DR
A 21-year-old woman presented with a rare case of skin coccidioidomycosis years after her initial infection, showing unusual histopathological features.
Contribution
This case highlights a rare delayed presentation and atypical histopathology of disseminated cutaneous coccidioidomycosis.
Findings
The patient showed deep dermal non-caseating granulomas, an unusual histopathological feature.
There was no pseudoepitheliomatous hyperplasia, which is typically seen in cutaneous coccidioidomycosis.
The patient had a remote history of Valley Fever, confirming a long-term progression of the disease.
Abstract
Coccidioides is a dimorphic fungus that causes coccidioidomycosis, also known as San Joaquin Valley Fever. The fungus is endemic to the southwestern United States, northern Mexico, and Central and South America. Infection is typically acquired through inhalation of dust particles that causes pulmonary disease. Direct cutaneous inoculation can occur but is rare. Histopathological examination of cutaneous lesions typically shows pseudoepitheliomatous hyperplasia with acute, suppurative granulomatous inflammation. Fungal organisms tend to be found more superficially and vary in density. Although non-caseating and sarcoidal granulomas have been described in late lesions of coccidioidomycosis, these tend to be in the upper two-thirds of the dermis. In this report, we describe a case of disseminated cutaneous coccidioidomycosis in a 21-year-old female seen as a dermatology outpatient for…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
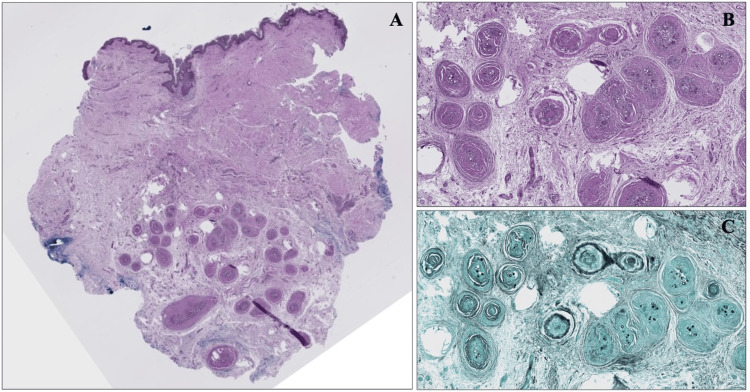 Figure 1
Figure 1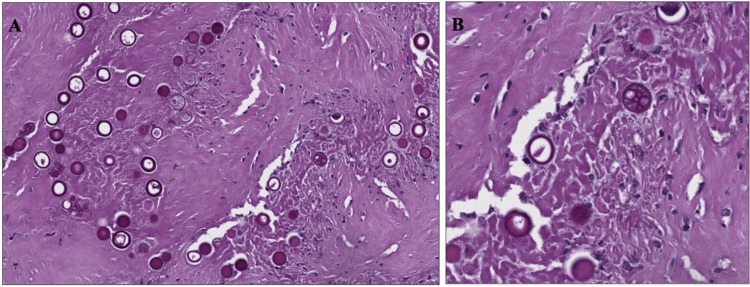 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsFungal Infections and Studies · Nail Diseases and Treatments · Antifungal resistance and susceptibility
Introduction
Coccidioides is a dimorphic fungus that causes coccidioidomycosis, also known as San Joaquin Valley Fever. It is caused by dimorphic species of Coccidioides immitis and Coccidioides posadasii endemic to the southwestern United States, northern Mexico, and Central and South America [1]. Infection is typically acquired through inhalation of dust particles that causes pulmonary disease. Occasionally, patients with pulmonary disease can have hematogenous or lymphatic spread to the bone, brain, and/or skin with systemic disease occurring in 1% of immunocompromised hosts [1-3]. Primary cutaneous disease, caused by direct inoculation or exposure at sites of trauma, is rare with less than 100 cases reported in the literature [4-6]. Clinical presentation of primary cutaneous coccidioidomycosis is variable with most cases reported describing non-ulcerated nodules that appear after a 2-3-week inoculation period [4,5].
On histological examination, cutaneous lesions of coccidioidomycosis typically show pseudoepitheliomatous hyperplasia, a reactive epidermal thickening seen in many infections, with acute, suppurative granulomatous inflammation [4,7]. Fungal organisms tend to be found more superficially and vary in density [4-6]. Hematoxylin and eosin (H&E), periodic acid-Schiff (PAS), and Gomori methenamine silver (GMS) stains are all useful in the examination of granulomas and help reveal spherules [1]. We report a case of cutaneous coccidioidomycosis with unusual histologic findings.
Case presentation
A healthy 21-year-old female from southern California presented to an outpatient dermatology clinic for a scar revision at the site of a previously excised draining lymph node secondary to systemic Valley Fever over 10 years ago. At her prior visit, she did not receive treatment aside from node excision and her symptoms self-resolved. She did not have a history of immunocompromise or other past medical history. At her presentation to dermatology, the scar was excised from the right inferolateral neck and sent for histopathological testing. H&E stains revealed non-caseating granulomas with spherules in the deep dermis and subcutis beneath a dermal scar (Figure 1). GMS stains and PAS stains were then applied highlighting these thick-walled spherules, predominantly 20-40 micrometers in diameter, some of which were filled with PAS-positive endospores, within the granulomas and multinucleated giant cells (see Figure 1 and Figure 2). Fite-Faraco and Ziehl-Neelson stains were negative for acid-fast bacilli. Uniquely, this patient had deep dermal granulomas, an absence of pseudoepitheliomatous hyperplasia, and a remote nature of prior infection. The pathology results were reviewed with the patient at a follow-up appointment. After discussing the findings and potential implications including indolent inoculation versus latent systemic infection, further medical therapy was deferred given the remote nature of her prior infection and lack of systemic symptoms.
A. Scanning magnification with H&E stain demonstrating epithelioid granulomas in the deep dermis and subcutis beneath a dermal scar. B. High-power magnification of epithelioid granulomas. C. GMS stain highlighting thick-walled spherules within granulomas and multinucleated giant cells. The fungal structures appear as clustered black spherules. H&E, hematoxylin and eosin; GMS, Gomori methenamine silver.
A. Thick-walled spherules, 20-40 micrometers in diameter, with B. PAS-positive endospores. PAS, periodic acid-Schiff.
Discussion
Coccidioidomycosis infection causes symptoms in approximately 40% of patients including cough, angina, fever, and erythema nodosum. Disseminated cutaneous infection can also occur. Histopathology of early lesions is characterized by dense inflammatory infiltrates composed of neutrophils, lymphocytes, and plasma cells [7]. Later in the disease process, granulomas and epithelioid inflammation develop, which typically contain double-walled spherules 10-80 micrometers in diameter filled with endospores [6,7].
Diagnosis is often made through a combination of detailed clinical history, serology, culture, and histopathology. In this report, we document a case of cutaneous coccidioidomycosis with unique histomorphology diagnosed several years after the initial infection. It is important to recognize that both acute and chronic signs of inflammation can be found in the infected tissues. The presence of neutrophils and eosinophils clustered around ruptured spherules suggests active disease while chronic granulomatous inflammation around unruptured spherules is more commonly found in patients with controlled disease [3,5-7]. Our specimen shows sarcoidal granulomas with organisms in the deep dermis and subcutis without overlying epidermal changes such as pseudoepitheliomatous hyperplasia to suggest an underlying infection. Additionally, lymphatic invasion may be another reason that overlying epidermal changes are not seen. Therefore, clinicians should consider a deeper biopsy if the index of suspicion for cutaneous coccidioidomycosis is high. Although suppurative granulomatous dermatitis is the most common pattern seen in cutaneous infections, sarcoidal granulomas should also prompt further workup for infection in the appropriate clinical context. When coccidioidomycosis is suspected, thorough clinical history remains paramount with a history of prior residence or recent travel to an endemic area remaining critical for diagnosis.
In this patient's case, with known prior history of coccidioidomycosis infection and lymph node removal, it is also plausible that direct inoculation occurred at the time of the prior surgery with scar revision revealing a site of indolent inoculation rather than a latent product of systemic infection. At the time of prior diagnosis and lymph node excision, treatment was deferred. In patients with known risk factors like immunocompromisation or with more moderate disease, treatment with antifungal agents including fluconazole and itraconazole can be given for a duration of 3-6 months [3].
Conclusions
Cutaneous coccidioidomycosis is a rare clinical entity that typically exhibits pseudoepitheliomatous hyperplasia with acute, suppurative granulomatous inflammation surrounding clusters of spherules and endospores. In this report, we document a case of cutaneous coccidioidomycosis with unique histomorphology including deep dermal granulomas and the absence of pseudoepitheliomatous hyperplasia diagnosed several years after initial infection. When coccidioidomycosis is suspected, detailed clinical history remains paramount to diagnosis and treatment can be initiated depending on patient symptoms and risk factors. A deeper biopsy should also be considered so that pathology is not missed.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Coccidioidomycosis: A review J Investig Med Johnson RH Sharma R Kuran R Fong I Heidari A 31632369202110.1136/jim-2020-001655 PMC 784806533495302 · doi ↗ · pubmed ↗
- 2Dust devil: The life and times of the fungus that causes Valley Fever P Lo S Pathog Lewis ER Bowers JR Barker BM 011201510.1371/journal.ppat.1004762 PMC 443187725973899 · doi ↗ · pubmed ↗
- 32016 Infectious Diseases Society of America (IDSA) clinical practice guideline for the treatment of coccidioidomycosis Clin Infect Dis Galgiani JN Ampel NM Blair JE 04663201610.1093/cid/ciw 36027470238 · doi ↗ · pubmed ↗
- 4Coccidioidomycosis and the skin: A comprehensive review An Bras Dermatol Garcia Garcia SC Salas Alanis JC Flores MG Gonzalez Gonzalez SE Vera Cabrera L Ocampo Candiani J 6106199020152656020510.1590/abd 1806-4841.20153805 PMC 4631225 · doi ↗ · pubmed ↗
- 5Primary cutaneous coccidioidomycosis J Am Acad Dermatol Chang A Tung RC Mc Gillis TS Bergfeld WF Taylor JS 9449494920031457668910.1016/s 0190-9622(03)00462-6 · doi ↗ · pubmed ↗
- 6Primary cutaneous coccidioidomycosis: An update Am J Clin Dermatol Reyna-Rodríguez IL Ocampo-Candiani J Chavez-Alvarez S 6816962120203255738010.1007/s 40257-020-00525-z · doi ↗ · pubmed ↗
- 7Coccidioidomycosis granulomas informed by other diseases: Advancements, gaps, and challenges J Fungi (Basel) Miranda N Hoyer KK 650920233736758610.3390/jof 9060650 PMC 10301931 · doi ↗ · pubmed ↗