Intersecting Pathologies: Polycythemia Vera and Recurrent Infections in an Elderly Patient
Prince Saha, Emre Sahin, Nirupam Nadella, Adil M Siddiqui, Lokesh Edara

TL;DR
This case report describes the complex management of a 95-year-old woman with polycythemia vera and recurring infections, highlighting the need for coordinated care.
Contribution
The paper presents a unique case illustrating the challenges of managing overlapping hematological and infectious conditions in elderly patients.
Findings
The patient exhibited persistent leukocytosis and thrombocytosis alongside recurrent infections.
Initial antibiotic resistance required treatment adjustments, emphasizing the complexity of managing PV with infections.
The case highlights the importance of multidisciplinary care and preventive strategies for high-risk patients.
Abstract
This case report highlights the diagnostic and therapeutic challenges encountered in the management of a 95-year-old female patient with polycythemia vera (PV) complicated by recurrent infections. The patient presented with significant leukocytosis, thrombocytosis, and concurrent infections, including a urinary tract infection and influenza B. PV, a myeloproliferative neoplasm, is characterized by increased production of red blood cells and often involves heightened activation of myeloid and megakaryocytic lineages, resulting in leukocytosis and thrombocytosis. These hematological abnormalities, coupled with underlying immune dysregulation, predispose patients to recurrent and severe infections. The patient's condition was further complicated by resistance to initial antibiotic therapy, necessitating adjustments in treatment. Despite resolving the infections, persistent leukocytosis…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
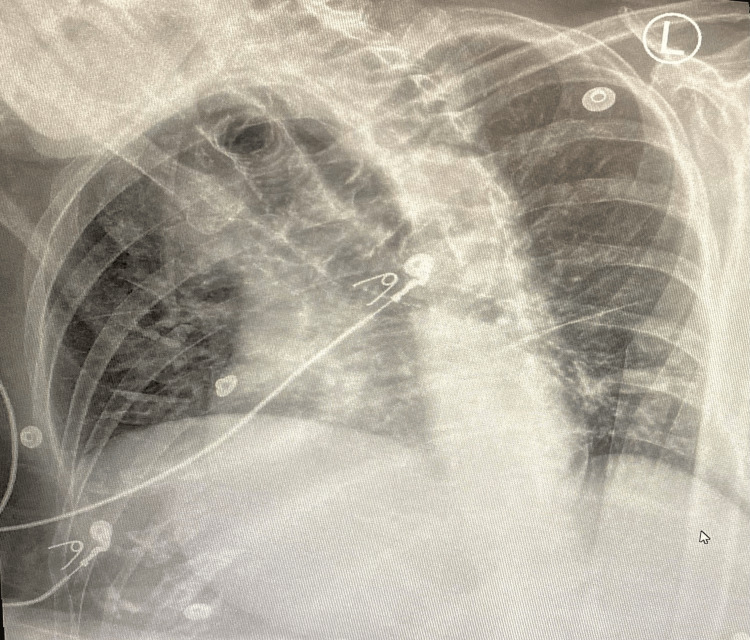 Figure 1
Figure 1| cTest | Results | Units | Normal Range |
| White Blood Cells (WBCs) | 30.5 | 103/mcL | 5.2-10 |
| Neutrophils% (Manual) | 98 | % | 52-73 |
| Lymphocytes% (Manual) | 2 | % | 20-45 |
| Neutrophils# (Manual) | 29.89 | 103/mcL | 1.47-6.20 |
| Lymphocytes# (Manual) | 0.6 | 103/mcL | 1.3-4.2 |
| Toxic Granulations | Slight | ||
| Prothrombin Time (PT) | 13.8 | seconds | 9.3-12.1 |
| International Normalized Ratio (INR) | 1.3 | 0.9-1.2 | |
| Activated Partial Thromboplastin Time (aPTT) | 37.0 | seconds | 23.9-32.8 |
| Hemoglobin | 9.3 | gm/dL | 12.3-15.3 |
| Hematocrit | 32.7 | % | 36.0-45.0 |
| Mean Corpuscular Volume (MCV) | 80.0 | fL | 81.0-99.0 |
| Mean Corpuscular Hemoglobin (MCH) | 22.7 | pg | 26.0-32.0 |
| Mean Corpuscular Hemoglobin Concentration (MCHC) | 28.4 | gm/dL | 31.0-35.4 |
| Red cell Distribution Width (RDW) | 22.1 | % | 11.5-14.5 |
| Platelet Count | 571 | 103/mcL | 130-433 |
| Blood Urea Nitrogen (BUN) | 26 | mg/dL | 7.0-17.0 |
| Creatinine | 1.10 | mg/dL | 0.52-1.04 |
| Estimated Creatinine Clearance | 28 | mL/min | 88–128 |
| Estimated GFR | 46 | mL/min/1.73m2 | >=90 |
| BUN/Creatinine Ratio | 23.6 | 10:1-20:1 |
| Test | Results | Units | Normal Range |
| Urine Color | Amber | Yellow | |
| Urine Clarity | Cloudy | Clear | |
| Urine pH | 5.0 | 5.0-8.0 | |
| Urine Specific Gravity | 1.018 | 1.000-1.035 | |
| Urine Protein | 100 | mg/dL | Negative |
| Urine Ketones | 5 | mg/dL | Negative |
| Urine Blood | Large | Negative | |
| Urine Leukocyte Esterase | Moderate | Negative | |
| Urine RBC | >182 | /hpf | 0-2 |
| Urine WBC | 90 | /hpf | 0-5 |
| Urine WBC clumps | 7 | /hpf | 0-1 |
| Urine Squamous Epithelial Cells | 2 | /hpf | 0-5 |
| Urine Bacteria | Moderate | /hpf | None Seen |
| Urine Mucus | Occassional | /lpf | None Seen |
| Test | Results | Units | Normal Range |
| Influenza Type A Antigen | Negative | Negative | |
| Influenza Type B Antigen | Positive | Negative | |
| SARS-CoV-2 Ag (Rapid) | Negative | Negative |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsMyeloproliferative Neoplasms: Diagnosis and Treatment · Eosinophilic Disorders and Syndromes · Hemoglobinopathies and Related Disorders
Introduction
Polycythemia vera (PV) is a pathological condition characterized by the excessive production of red blood cells (RBCs), leading to an increase in the overall mass of RBCs in the body [1]. Frequently, the myeloid and megakaryocytic lineages are simultaneously activated, resulting in the heightened production of white blood cells and platelets [1]. The present knowledge of pathophysiology concerns heightened responsiveness to growth factors due to an anomalous hematopoietic cell clone. Signs and symptoms such as headache, dizziness, claudication, and thrombosis can be attributed to elevated blood viscosity [1].
Leukocytosis, usually referred to as an increased white blood cell count, is a frequently observed laboratory abnormality in both inpatient acute care settings and outpatient practices [2]. It has multiple causes, such as infection, inflammation, and malignancy, that practitioners from all disciplines should be knowledgeable about [2].
Thrombocytosis is a condition characterized by excessive platelet production in the body. Reactive thrombocytosis, also known as secondary thrombocytosis, occurs when an underlying ailment, such as an infection, causes it [3]. Occasionally, when there is no apparent underlying cause for a high platelet count, the illness is referred to as primary thrombocythemia, essential thrombocythemia, or PV [3]. This condition is characterized by abnormalities in the blood and bone marrow [3].
This report provides a unique case during the approach to leukocytosis and thrombocytosis, including their differential diagnosis. It also discusses the challenges faced by the interprofessional team involved in patient care when considering treatment options and their effectiveness in cases where multiple factors contribute to elevated counts.
Case presentation
A 95-year-old Hispanic woman was transferred from an Adult Living Facility (ALF) to the emergency room on March 11, 2024, at a (secondary health care center) in Miami-Dade County, Florida. She has a past medical history of (Janus Kinase) JAK-2 positive PV treated with hydroxyurea, hyperlipidemia, hypothyroidism, dementia, hypertension, pneumonia, total hip replacement, and coronary artery disease. She came with complaints of right facial swelling, redness, and progressive generalized weakness. She was later found to have significant leukocytosis at around 30,000 WBCs per microliter and significant hematuria and pyuria suggestive of a urinary tract infection (UTI).
During the physical examination, the patient appeared frail and lethargic but not distressed, with a T-max of 97.6F. Her neurological examination revealed AAOx1, meaning she was oriented only to people. The remainder of the examination was within normal limits. Significant laboratory and radiological findings at the time of presentation are presented in Tables 1-3 and Figure 1.
Chest X-ray of the patientThe chest X-ray failed to reveal any consolidation
The blood analysis showed evidence of microcytic anemia, indicating a possible iron deficit. Additionally, there was an increase in platelet count (thrombocytosis) and white blood cells (WBCs) with minor toxicity with toxic granulations (granulocytic leukocytosis). The kidney function test indicated the presence of acute kidney injury in the patient, as evidenced by elevated creatinine levels and abnormal values of BUN and BUN/creatinine ratio, as shown in Table 1. The urine routine testing revealed the presence of hematuria and pyuria, along with elevated leukocyte esterase and urine bacteria, confirming the diagnosis of a UTI, as shown in Table 2. Cultures were obtained, and based on empirical evidence, the patient was initiated on cefepime and vancomycin.
The rapid antigen testing results for influenza B came out to be positive, as shown in Table 3. A chest X-ray was subsequently ordered, but it failed to reveal any consolidation, as shown in Figure 1. The patient was appropriately started on oseltamivir therapy. The SARS-CoV-2 rapid antigen testing came out negative. Due to the patient's repeated history of UTIs, cefepime was replaced with meropenem. The vancomycin and oseltamivir treatment was appropriately modified to avoid any difficulties due to toxicity, considering the patient's advanced age and impaired renal function.
The culture ultimately cultivated Enterococcus species, specifically Enterococcus faecium. Additional bacterial susceptibility pattern testing revealed that the bacterium exhibited resistance to vancomycin. Subsequently, treatment with linezolid was initiated, and the patient's clinical condition improved significantly.
Nevertheless, despite completing the treatment, the WBC count remained high, causing uncertainty regarding whether the increased number of leukocytes resulted from an inflammatory, infectious, or malignant process occurring in the background. It is challenging to accurately diagnose the condition, as in this patient with an ongoing infection (UTI & Influenza B) and underlying myeloproliferative disorder (PV) and determine the appropriate treatment choice and duration.
Discussion
PV leads to excessive RBC production, often accompanied by concurrent activation of myeloid and megakaryocytic lineages, boosting WBC (leukocytosis) and platelet counts (thrombocytosis) [1]. Leukocytosis and thrombocytosis can each have their respective etiologies, complications, and further implications in a patient, and in the background of a myeloproliferative disorder, it can be challenging to pinpoint the exact pathological condition contributing to these signs, thereby putting forward a challenge to the interdisciplinary team involved in patient care [1].
A study conducted by Luque et al. discovered that individuals with myeloproliferative neoplasms (MPNs) have chronic inflammation and an imbalance in their immune system, resulting in elevated levels of pro-inflammatory cytokines [4]. MPNs are associated with alterations in immune cell populations, particularly B lymphocytes. Studies indicate that patients with MPNs often exhibit reduced numbers of B lymphocytes, which inversely correlates with the burden of the JAK2-V617F allele [5]. The implications of this observation suggest a potential compromise in immune function, which may contribute to an increased vulnerability to infections among these individuals [5]. Understanding these relationships is crucial for developing targeted therapies and improving patient management strategies in MPNs.
Romano et al., in their study, found that abnormalities in the immune system vary among patients with different driver mutations [6]. Specifically, JAK2-mutated cases showed more alterations in T-regulatory cell populations, while CALR-mutated cases exhibited dysregulations in the interferon-γ-axis [6]. Furthermore, individuals with MPNs are also more susceptible to other medical conditions, including cardiovascular and thromboembolic disease, autoimmune disease, and solid malignancies [7-9]. As a result, they may have a higher likelihood of developing infections due to the treatment of these comorbidities, hospitalization for unrelated reasons, or overall increased vulnerability. The higher risk of diseases found in MPNs may be attributed to the simultaneous presence of multiple underlying causes [7-9].
There is widespread support for immunization against pneumococci and influenza in Sweden for adults aged 65 and over and for specific risk categories (MPNs not included) [10].
However, the provision and subsidization of these vaccinations for residents may vary across different counties [10]. Since 2009, health authorities have included pneumococci immunization in the recommended routine for babies [10]. In 2014, reports indicated that 50% of the elderly received the influenza vaccine [10].
Since 2013, Sweden has offered vaccination against the reactivation of zoster to individuals who specifically request it, although this vaccination is not commonly advised [11]. The determination of appropriate preventive or prophylactic actions for individuals with MPNs cannot solely rely on observational findings [11]. However, it may be prudent to consider some vaccines, such as the varicella zoster vaccine, for specific high-risk individuals [11].
According to Landtblom et al., individuals with MPNs had a considerably greater susceptibility to severe infections when compared to a control group from the general population [11]. The absence of disparities in infection risk between untreated and treated patients in their study indicated that the heightened risk of infections is an inherent characteristic of MPNs [11]. Therefore, the risk of infection should not be a decisive factor when contemplating cytoreductive treatments like hydroxyurea or interferon-α if they are otherwise indicated [11]. It is essential to acknowledge the heightened vulnerability to infections while treating patients with MPNs and when assessing the impact of drugs, especially JAK inhibitors, on their susceptibility to infections.
Conclusions
In conclusion, the case demonstrates the complex difficulties faced when diagnosing and treating patients with PV who also have high WBC count, high platelet count, and illnesses such as UTIs and influenza. The interaction between the underlying myeloproliferative illness and the infectious processes adds complexity to the diagnosis and therapy considerations. The discussion elucidates the immunological dysregulation exhibited in people with MPNs, which makes them more prone to chronic inflammation and infections. Moreover, the diverse irregularities in the immune system among individuals with distinct driver mutations highlight the intricacy of handling issues connected to MPNs. Emphasis is placed on the significance of preventative interventions, such as immunization against pneumococci and influenza, for high-risk persons. Nevertheless, the choice regarding preventive measures should be approached with care, considering specific patient characteristics and the existing data. Furthermore, the increased susceptibility to infections highlights the importance of thorough assessment and control of infectious consequences, particularly while undergoing cytoreductive therapies like hydroxyurea or interferon-α. The results indicate that the potential for infection should not discourage the proper utilization of these treatments when necessary. To summarize, this study highlights the significance of a multidisciplinary strategy that includes hematologists, infectious disease specialists, and other healthcare providers in effectively managing patients with PV and its related consequences. Additional studies are necessary to gain a deeper understanding of the immunological pathways that contribute to infections connected to MPNs and enhance preventive and treatment approaches for these individuals.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Polycythemia vera Stat Pearls [Internet] Lu X Chang R Treasure Island (FL)Stat Pearls Publishing 2025 https://www.ncbi.nlm.nih.gov/books/NBK 557660/
- 2Leukocytosis Stat Pearls [Internet] Mank V Azhar W Brown K Treasure Island (FL)Stat Pearls Publishing 2025 https://www.ncbi.nlm.nih.gov/books/NBK 560882/
- 3Mayo Clinic. Thrombocytosis 3 2024 2024 https://www.mayoclinic.org/diseases-conditions/thrombocytosis/symptoms-causes/syc-20378315
- 4Key role of inflammation in myeloproliferative neoplasms: instigator of disease initiation, progression and symptoms Curr Hematol Malig Rep Luque LF Blackmon AL Ramanathan G Fleischman AG 1451531420193111947510.1007/s 11899-019-00508-w PMC 7746200 · doi ↗ · pubmed ↗
- 5B-cell frequencies and immunoregulatory phenotypes in myeloproliferative neoplasms: influence of ruxolitinib, interferon-α2, or combination treatment Eur J Haematol Sørensen AL Bjørn ME Riley CH 35136110320193129788310.1111/ejh.13292 · doi ↗ · pubmed ↗
- 6Mutations in JAK 2 and Calreticulin genes are associated with specific alterations of the immune system in myelofibrosis Oncoimmunology Romano M Sollazzo D Trabanelli S 06201710.1080/2162402 X.2017.1345402 PMC 566508129123956 · doi ↗ · pubmed ↗
- 7Risk for arterial and venous thrombosis in patients with myeloproliferative neoplasms: a population-based cohort study Ann Intern Med Hultcrantz M Björkholm M Dickman PW Landgren O DerolfÅR Kristinsson SY Andersson TM 31732516820182933571310.7326/M 17-0028 PMC 7533681 · doi ↗ · pubmed ↗
- 8Autoimmunity and the risk of myeloproliferative neoplasms Haematologica Kristinsson SY Landgren O Samuelsson J Björkholm M Goldin LR 121612209520102005387010.3324/haematol.2009.020412 PMC 2895049 · doi ↗ · pubmed ↗