A ‘COMMON SENSE’ approach to geriatric patients in clinical practice
Lara S. Greenstein

TL;DR
This paper introduces a practical approach for primary care providers to manage older patients effectively without specialized geriatric training.
Contribution
The novel contribution is the 'COMMON SENSE' mnemonic, which simplifies geriatric assessments for primary care practitioners.
Findings
The 'COMMON SENSE' approach ensures key geriatric assessment components are not overlooked.
Simple screening tools can be used effectively in busy primary care settings to identify geriatric syndromes.
Abstract
South Africa has a critical shortage of geriatricians and a growing ageing population. Most geriatric patients are cared for by their primary care practitioner who may not have been trained in the care of the older adult. The comprehensive geriatric assessment (CGA) is the cornerstone of the geriatric consultation but can be time-consuming. By using a common sense approach to the geriatric patient, none of the important components of the CGA will be missed. The mnemonic ‘COMMON SENSE’ can be used as a tool to assist in identifying the common conditions that older adults experience, as well as highlight specific considerations that become increasingly important in this population. Many simple and time-effective screening tools are available to assist in diagnosing the geriatric syndromes which can be easily implemented in a busy primary care practice.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
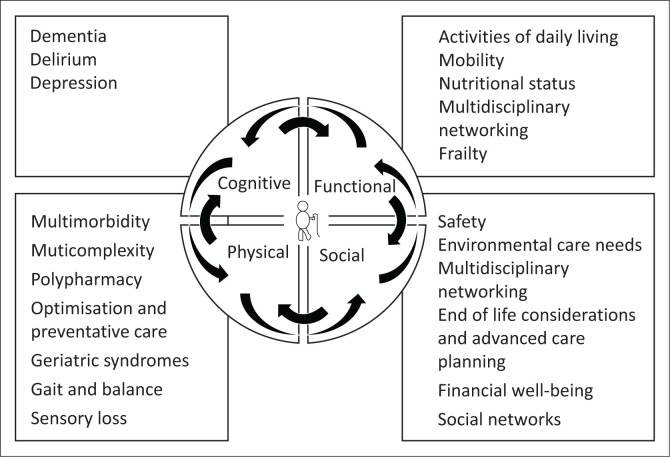 FIGURE 1
FIGURE 1| Geriatric syndrome | Assessment tool | Interpretation | Sensitivity and specificity | References |
|---|---|---|---|---|
| Cognitive impairment (dementia) | Mini-cog | Give the patient three words to remember. Ask the patient to draw a clock and make the time ten past nine. Ask the patient to recall all three words. | Sensitivity: 99% |
|
| Depression | 2-item Geriatric Depression Scale test | An answer of yes to either of: Being down, depressed or hopeless Having little interest or pleasure in doing things? | Sensitivity: 91.8% |
|
| Polypharmacy | Use a drug-interaction checker, the Beers criteria or STOPP/START criteria | The Beers criteria is a guideline used to identify potentially inappropriate medicines that should be avoided in older adults. | - |
|
| Frailty | The Clinical Frail Scale | 1 point each for the following: | Sensitivity: 88.0% |
|
| Malnutrition | Nestle Mini Nutritional Assessment | Questions asking about food intake, weight loss, mobility, psychological stress and neuropsychological problems. | Sensitivity: 96% |
|
| The Simplified Nutritional Appetite Questionnaire (SNAQ) | Four questions asking about appetite, satiation, food taste and number of meals per day. | Sensitivity: 69.2% |
| |
| Gait/balance abnormalities | Timed-Up-and-Go (TUG) | The patient must be timed while rising from a chair, walking three metres, turning around, walking back and sitting down. | - |
|
| Falls | Timed-Up-and-Go with or without a fall risk assessment | Ask each patient every year if they have fallen. | Sensitivity: 0.31 (95% CI: 0.13–0.57) |
|
| Incontinence | 3IQ test | Have you leaked urine in the past 3 months? with activity – stress incontinence with urgency – urge incontinence both – mixed incontinence neither – another cause | Sensitivity: 75% |
|
| Sarcopenia | Sarc-F Questionnaire | A number of questions each scoring a maximum of 2 points for strength, assistance in walking, rising from a chair, climbing stairs and falling. | Sensitivity: 28.9% – 55.3% |
|
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsFrailty in Older Adults · Aging and Gerontology Research · Chronic Disease Management Strategies
Introduction
The number of people aged 65 years and above in South Africa is increasing and general practitioners are treating a growing number of older patients.^1,2^ Geriatric patients often have multiple underlying conditions, and because of this complexity, consulting with older adults may be daunting.^3^ There is a critical shortage of geriatricians in South Africa and the general practitioner often has to take on the role of overseer. By applying the mnemonic ‘COMMON SENSE’, which is being coined in this article (see Box 1), important considerations and common conditions affecting older adults are less likely to be missed. Awareness of these geriatric syndromes enables clinicians to utilise simple targeted screening tools to identify conditions that may not be immediately apparent, thereby optimising the quality of care provided to older patients. As only 15–20 min is allocate to a general practice consultation, not every condition can be assessed in this short time, and individualised care is necessary to decide which components to tackle in each appointment. An hour-long booking for a comprehensive geriatric assessment (CGA) would be ideal.
BOX 1The components of COMMON SENSE.CComprehensive geriatric assessmentO_4_Optimise
- Treatments
- Targets
- Function
- Preventative strategies
Mind (depression, delirium and dementia)Mobility (falls and instability)MedicationsMulticomplexity (multimorbidity)Matters most (goals and care)O_2_Oops
-
Incontinence
-
Iatrogenesis – medication, procedure or diagnostic testing related NNutritionSSyndromes
-
The 5 Ms
-
Incontinence
-
Iatrogenesis
-
Loneliness
-
Frailty
-
Sarcopenia
-
Malnutrition EEnvironment – care needsNNetworking and multidisciplinary teamsSSafety (The Older Persons Act)EEnd of life care and advanced care planningNote: Please see the full reference list of this article https://doi.org/10.4102/safp.v67i1.6027 for more information.
The comprehensive geriatric assessment
The CGA is the cornerstone of geriatric medicine, taking into account all the components of the COMMON SENSE mnemonic (see Figure 1). It enhances the well-established biopsychosocial model by emphasising the critical interplay of these three vital components, while integrating cognitive and functional assessments to provide a more comprehensive approach to patient care. The CGA is a multidimensional approach to care of the older person underscoring the need for a multidisciplinary team approach.^4^ The members of this team include all allied health professionals, often various medical practitioners, pharmacists and nursing staff. This framework facilitates the creation of a comprehensive problem list and the development of an individually tailored care plan. The care plans, along with the implemented interventions, should be regularly reviewed and adjusted as necessary. The CGA can be utilised in a variety of settings, both inpatient and outpatient. It is particularly valuable when a general practitioner is managing a frail older adult with multiple geriatric syndromes, during transitions in care settings and following hospital discharge.^4,5,6^ The remainder of this article will discuss the individual components of the CGA with a focus on the COMMON SENSE components and will discuss the most time and cost-effective screening tools to assess these common problems.
The comprehensive geriatric assessment with the COMMON SENSE components.
The 5 Ms and the geriatric syndromes
Geriatric syndromes are common conditions that occur in older adults as a result of multiple contributing factors.^7^ Consequences of these syndromes are the loss of independence, deteriorating health, higher healthcare costs, the need for institutionalised care, morbidity and mortality.^7^ In 2017, the 5 Ms (see Box 1) were introduced to help those practitioners who care for older patients to identify common geriatric problems.^8^ The 5Ms take into account many of the geriatric syndromes including delirium, dementia, depression, falls and instability, polypharmacy, multimorbidity and goals of care.^8^ There are a few other syndromes, however, that deserve mention, including loneliness, frailty, sarcopenia, malnutrition, incontinence and iatrogenesis. Iatrogenesis comes in many forms and may result from medications, adverse drug events, or complications from procedures, which may be diagnostic or therapeutic. These syndromes are frequently underdiagnosed because of the complexities involved in managing older adults.
Optimisation of the older adult
The main goals of successful ageing are to keep the older adult as functional as possible for as long as possible, and as this is a multidimensional concept, successful ageing incorporates all the CGA components including functional, cognitive, social and psychological well-being.^9^ One way to achieve this is to optimise medication and treatment regimes, optimise function, aim for appropriate therapeutic targets and make use of preventative strategies.
Functional status is the ability of the older adult to look after themselves and perform the activities of daily living required of them to live independently.^9^ Box 2^15,16,17^ shows both the basic and instrumental activities of daily living. If a person cannot perform instrumental activities of daily living safely by themselves, then they will require help – either at home or in a mid-care type setting. Inability to complete certain instrumental activities independently such as driving, administering medication and taking care of financial affairs can pose a physical or financial safety threat. Those who cannot perform basic activities of daily living independently, such as eating, toileting and transferring from a bed to a chair will require 24-h care either at home or in a frail-care setting.
BOX 2Activities of daily living. Basic activities of daily living ^ 15 ^ BathingDressingToiletingTransferring from a bed to a chairFeeding Instrumental activities of daily living^16,17^ ShoppingPhoningFood preparationLaundryTransportationFinancial affairsAdministering own medicationNote: Please see the full reference list of this article https://doi.org/10.4102/safp.v67i1.6027 for more information.
Targets for common conditions such as type 2 diabetes mellitus and hypertension depend on the person’s functional and frailty status. While tighter control of both blood pressure and glucose measurements are recommended for healthy older adults who are able to complete all their own instrumental activities of daily living and who are not frail, systolic blood pressures of 150 mmHg^10^ and heamoglobin A1C (HbA1C) measurements of between 7% and 8.5%^11^ are acceptable for those patients who have multiple chronic long-term conditions, who are frail and who are nearing end of life.
Optimising medications is vitally important because inappropriate polypharmacy, taking more medications than are medically necessary or using medication that is ineffective, can lead to deleterious consequences such as adverse drug reactions, morbidity and mortality.^12^ Useful tools that can be used to assist with rationalising medications include the use of drug-interaction checkers, the Beers criteria and the STOPP/START criteria (see Table 1).^13,14^
Other optimisation strategies include vaccinations and the screening for osteoporosis and common malignancies such as those arising from the prostate, breast and colon. The decision to undergo certain screening tests depends on whether the benefits outweigh the risks, personal preferences and the likelihood that the patient will live long enough to experience the benefits of treating any conditions that are diagnosed.
Social and care needs of the older adult
Choosing the most appropriate care setting is dependent on the cognitive and functional status of the older person. Other factors that need to be taken into account include the availability of social support networks and finances. Frail-care facilities can be expensive and the waiting times for admission can be long. A poor support system can result in loneliness, which itself is a risk factor for poor health.^18^ Older adults constitute a vulnerable population and are therefore safeguarded by the Older Persons Act,^19^ which mandates the reporting of any suspected abuse or neglect against an older person.^20^
Advance care planning and end of life decisions become increasingly more important to discuss as the older adult becomes frailer. Discussions around healthcare proxies, expectations at the end of life and living wills cannot be adequately addressed in the last few minutes of a consultation, and a healthcare practitioner who has an established and trusted relationship with the patient is best suited to initiate these discussions.^21^ Currently, there is no law in South Africa to validate a living will; however, there is an ethical expectation from the patient who has a living will that their wishes will be followed.^22^
Simple screening tools
A number of screening tools and toolkits are available to assist in best diagnosing the various geriatric syndromes. As a result of both time and resource constraints in the primary care setting, a simple screening of the major geriatric syndromes would be sufficient to screen for the majority of these syndromes (see Table 1). Those who are flagged can then be interrogated in more depth or referred on to the appropriate clinician or allied healthcare worker.^6^ The CGA itself can take up to 2 hours to complete and this is usually not possible during the course of a single short consultation.
For certain syndromes such as hearing impairment and poor vision, a simple yes or no question asking if there are any problems is adequate. Screening for every syndrome is sometimes not achievable in the course of a consultation, and for a busy practice, the most important syndromes to ask about would be falls, memory problems and to perform a medication review. The Timed-Up-and-Go (TUG) takes a few seconds and gives a wealth of information.^23^ Difficulty in getting up from the chair may indicate proximal muscle weakness; gait abnormalities can be seen and characterised when the patient walks the three metres, and both static and dynamic balance problems can be detected. Screening for cognition can be performed by administering the simple mini-cog, which provides information on many aspects of cognition.^24^ Both immediate and delayed recall are tested with the three words and executive function, planning and sequencing with the clock drawing test.
Conclusion
Geriatric syndromes are common and often difficult to diagnose. Assessment tools can be a simple and cost-effective means to diagnose these syndromes. In addition to the standard history and examination, using a simple mnemonic ‘COMMON SENSE’ allows the primary care physician to remember the important components of the geriatric assessment.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1World Health Organization. World report on ageing and health. Geneva: World Health Organization; 2015.
- 2Naidoo K, Van Wyk J. What the elderly experience and expect from primary care services in Kwa Zulu-Natal, South Africa. Afr J Prim Health Care Fam Med. 2019;11(1):2100. 10.4102/phcfm.v 11i 1.210031714116 PMC 6852327 · doi ↗ · pubmed ↗
- 3Bell SP, Vasilevskis EE, Saraf AA, et al. Geriatric syndromes in hospitalized older adults discharged to skilled nursing facilities. J Am Geriatr Soc. 2016;64(4):715–722. 10.1111/jgs.1403527059831 PMC 4840035 · doi ↗ · pubmed ↗
- 4Pilotto A, Cella A, Pilotto A, et al. Three decades of comprehensive geriatric assessment: Evidence coming from different healthcare settings and specific clinical conditions. J Am Med Dir Assoc. 2017;18(2):192.e 1–192.e 11. 10.1016/j.jamda.2016.11.00428049616 · doi ↗ · pubmed ↗
- 5Parker SG, Mc Cue P, Phelps K, et al. What is comprehensive geriatric assessment (CGA)? An umbrella review. Age Ageing. 2017;47(1):149–155. 10.1093/ageing/afx 16629206906 · doi ↗ · pubmed ↗
- 6Little MO. The rapid geriatric assessment: A quick screen for geriatric syndromes. Mo Med. 2017;114(2):101–104.30228554 PMC 6140035 · pubmed ↗
- 7Inouye SK, Studenski S, Tinetti ME, Kuchel GA. Geriatric syndromes: Clinical, research, and policy implications of a core geriatric concept. J Am Geriatr Soc. 2007;55(5):780–791. 10.1111/j.1532-5415.2007.01156.x 17493201 PMC 2409147 · doi ↗ · pubmed ↗
- 8Molnar F, Frank CC. Optimizing geriatric care with the GERIATRIC 5Ms. Can Fam Physician. 2019;65(1):39.30674512 PMC 6347324 · pubmed ↗