Factors associated with cigarette smoking among learners at a high school in KwaZulu-Natal
Gcinile V. Ngwenya, Refiloe M. Malaka, Lindiwe P. Cele, Modikwe Rammopo

TL;DR
This study found that 21% of high school students in KwaZulu-Natal smoke, with factors like having a smoking family member increasing the likelihood.
Contribution
The study identifies key factors associated with cigarette smoking among high school learners in South Africa.
Findings
21% of 400 participants reported smoking cigarettes.
Having a smoking family member significantly increased the odds of smoking (AOR = 5.82).
Most smokers accessed cigarettes from shops and smoked on school premises.
Abstract
Young smokers are said to have increased risk of nicotine addiction, even at lower levels of consumption compared to adults, making smoking cessation among this group much more difficult. A survey previously conducted in South Africa indicated an early smoking debut age of below 18 years. This study investigated the prevalence of cigarette smoking and associated factors among high school learners. The study was conducted at a high school located in Madadeni township of KwaZulu-Natal. This cross-sectional study collected data through interviews using self-administered questionnaires. Data analysis was conducted on Epi Info 7 and STATA 17. Eighty-four (21%) of the 400 participants reported smoking cigarettes. Of these, forty-nine (58.3%) had a smoking friend. Sixty out of 81 (74.1%) accessed cigarettes from the shops, whilst 69.2% (n = 54/78) smoked inside the school premises.…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
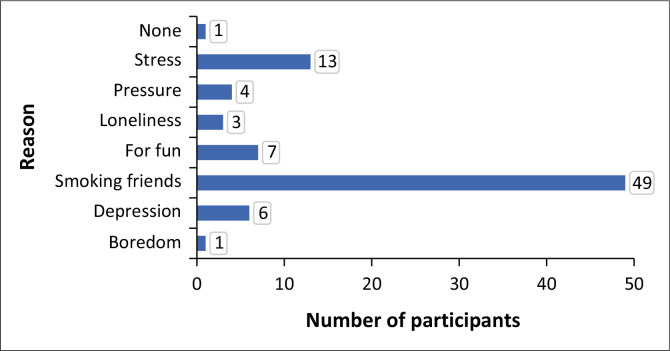 FIGURE 1
FIGURE 1| Variables | Frequency | Percentage | Mean | s.d. |
|---|---|---|---|---|
|
| ||||
| Female | 216 | 54.0 | - | - |
| Male | 184 | 46.0 | - | - |
| Age | - | - | 16 | 2.1 |
|
| ||||
| 12–15 | 175 | 43.8 | - | - |
| 16–18 | 196 | 49.0 | - | - |
| ≥ 19 | 29 | 7.2 | - | - |
|
| ||||
| 8 | 74 | 18.5 | - | - |
| 9 | 84 | 21.0 | - | - |
| 10 | 107 | 26.8 | - | - |
| 11 | 92 | 23.0 | - | - |
| 12 | 43 | 10.8 | - | - |
|
| ||||
| Other | 169 | 42.7 | - | - |
| Christian | 227 | 57.3 | - | - |
|
| ||||
| Rural | 96 | 24.2 | - | - |
| Semi-urban | 301 | 75.8 | - | - |
|
| ||||
| Yes | 84 | 21 | - | - |
| No | 316 | 79 | - | - |
| Age at smoking debut, |
| - | 14.8 | 1.79 |
| Variable | Total | Female, | Male, |
| |||
|---|---|---|---|---|---|---|---|
|
| % |
| % |
| % | ||
|
| |||||||
| 10–12 | 6 | 7.0 | 3 | 50 | 3 | 50 | 0.83 |
| 12–15 | 50 | 60.0 | 19 | 38 | 31 | 62.0 | - |
| 16–19 | 27 | 33.0 | 10 | 37 | 17 | 63 | - |
|
| |||||||
| Daily | 56 | 67.4 | 22 | 39.3 | 34 | 60.7 | 0.63 |
| Weekends only | 13 | 15.7 | 6 | 46.2 | 7 | 53.8 | - |
| Weekly | 14 | 16.9 | 4 | 28.6 | 10 | 71.4 | - |
|
| |||||||
| School | 21 | 25.9 | 7 | 33.3 | 14 | 66.7 | 0.59 |
| Shops | 60 | 74.1 | 24 | 40 | 36 | 60 | - |
|
| |||||||
| No | 24 | 30.8 | 8 | 33.3 | 16 | 33.3 | 0.54 |
| Yes | 54 | 69.2 | 22 | 40.7 | 32 | 59.3 | - |
|
| |||||||
| No | 8 | 9.6 | 3 | 37.5 | 5 | 62.5 | 1.00 |
| Yes | 75 | 90.4 | 29 | 38.7 | 46 | 61.3 | - |
|
| |||||||
| No | 18 | 21.4 | 6 | 33.3 | 12 | 66.7 | 0.64 |
| Yes | 66 | 78.6 | 26 | 39.4 | 40 | 60.6 | - |
|
| |||||||
| No | 63 | 75.0 | 28 | 44.4 | 35 | 55.6 | 0.04 |
| Yes | 21 | 25.0 | 4 | 19 | 17 | 81 | - |
|
| |||||||
| No | 6 | 7.0 | 2 | 33.3 | 4 | 66.7 | 1.00 |
| Yes | 77 | 93.0 | 30 | 39 | 47 | 61 | - |
| Characteristic | Unadjusted |
| Adjusted |
| ||
|---|---|---|---|---|---|---|
| OR | 95% CI | OR | 95% CI | |||
|
| ||||||
| Male | 2.26 | 1.38–3.71 | 0.001 | 2.33 | 1.29–4.17 | 0.004 |
| Female | - | 1 | - | - | - | - |
|
| ||||||
| 12–15 | 0.08 | 0.03–0.21 | < 0.001 | 0.04 | 0.01–0.15 | < 0.001 |
| 16–19 | 0.54 | 0.25–1.19 | 0.13 | 0.36 | 0.13–0.18 | 0.05 |
| ≥ 19 | - | 1 | - | - | 1 | - |
|
| ||||||
| ≤ 10 | 0.47 | 0.29–0.77 | 0.002 | 1.64 | 0.85–3.18 | 0.14 |
| > 10 | - | 1 | - | - | 1 | - |
|
| ||||||
| Christian | 0.05 | 0.00–0.48 | 0.01 | 0.01 | 0.00–0.18 | 0.002 |
| Other | - | 1 | - | - | - | - |
|
| ||||||
| Semi-urban | 0.15 | 0.01–1.63 | 0.05 | - | - | - |
| Rural | - | 1 | - | - | - | - |
|
| ||||||
| Yes | 5.68 | 3.21–10.01 | < 0.001 | 5.82 | 3.08–11.0 | < 0.001 |
| No | - | 1 | - | - | 1 | - |
|
| ||||||
| Yes | 1.15 | 0.00–0.56 | 0.92 | - | - | - |
| No | - | 1 | - | - | - | - |
|
| ||||||
| Yes | 0.85 | 0.49–1.48 | 0.56 | - | - | - |
| No | - | 1 | - | - | - | - |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsSchool Health and Nursing Education
Introduction
Smoking remains one of the major public health problems worldwide, with tobacco smoking responsible for more than 8 million global deaths each year (Arrazola et al. 2017). The bulk of tobacco users are reported to live in low-and middle-income countries (LMICs), contributing 80% to the 1.3 billion global tobacco users (World Health Organization [WHO] 2023). The Southeast and European regions of the WHO currently have the highest proportions of tobacco users in the population, at 26.5% and 25.3%, respectively. Women in the European region are reported to have high rates of smoking than males, which are more than double the global average (Jafari et al. 2021).
Cigarettes are the most widely used tobacco products in the world. Cigarette smoking is not harmful only to smokers, but it is also detrimental to nearby people through exposure to toxic second-hand smoke (American Lung Association [ALA] 2024b). Harmful effects include, among others, increased risk of latent tuberculosis (TB) progressing to active TB and poor prognosis, increased risk of chronic obstructive pulmonary disease (COPD), lung cancer, diabetes, premature babies, reproductive health in women, low birth weight babies and stroke among others (National Health Services 2022). Adolescent cigarette smoking has been linked with severe respiratory illness, lung growth and function, and reduced physical fitness (ALA 2024a).
Available evidence suggests an increased risk of nicotine addiction among young smokers, even at lower levels of consumption compared to adult smokers, making smoking cessation among this group much more difficult (Mahajan, Homish & Quisenberry 2021). Nicotine is known to elicit serious changes in parts of the developing teenage brain, some of which are involved with emotion regulation (Castro, Lotfipour & Leslie 2023). Studies have reported an association of nicotine dependence with smoking debut age of younger than 20 years. Surveys conducted among school learners in South Africa reported smoking at the debut age of 13 years old. This corroborates reports of tobacco and nicotine use by children aged between 13 and 16 years old (WHO 2024).
Among the studies that have investigated the factors associated with cigarette smoking, having a smoking friend or family member has been found to stimulate the initiation of smoking (Asif et al. 2017). The influence of advertisements of tobacco products on television, movies and magazines and the lack of awareness and knowledge among the learners have also been cited (CDC 2023; Sun et al. 2022). Others have also cited depression, anxiety and stress as predictors of cigarettes among school children (Fluharty et al. 2016). This study aimed to determine the prevalence of cigarette smoking and investigate associated factors among high school learners.
Research methods and design
Study design
This study used a quantitative, descriptive, cross-sectional design and conducted interviews using self-administered questionnaires among the learners in one of the high schools in Amajuba District in KwaZulu-Natal (KZN). The collected data were used to determine the prevalence of cigarette smoking and the associated factors.
Study setting
This study was conducted in one of 12 high schools situated at 1014 Madadeni, Newcastle, 2957 of Amajuba district in KZN province, South Africa. Amajuba borders the Free State and Mpumalanga provinces. It is a public secondary school classified as Quintile 3 that caters to a community with moderate socio-economic status. The school has a total of 1816 learners and 56 educators, resulting in a student-teacher ratio of 32:1. The school operates from 07:20 a.m. to 14:30 a.m. (SchoolsDigest 2024).
Data sources and target population
The study used a self-administered questionnaire written in English and translated into isiZulu, the most spoken language in the area. The data collection tool comprised of three sections. Section A collected the sociodemographic data, including the learner’s age, sex and grade. Section B collected question items to capture smoking behaviour and influences of smoking. Section C collected the reasons for smoking among the participants who had indicated that they smoked cigarettes.
The study population were all learners attending one of the high schools of Madadeni in the Amajuba district. The learners were eligible for the study if they were 12 years old and above. Potential study participants were excluded from participating if they did not offer signed assent or parental informed consent forms and if they were writing examinations during data collection. The data collection occurred between August 2022 and October 2022
Sample size and sampling technique
The authors used the Raosoft sample size calculator (Raosoft 2004) to determine the recommended sample size. The total headcount of 1800 learners was used for the population size, and the authors selected a confidence level of 95%, which corresponds to a 5% margin of error, and chose a 50% response rate to obtain a minimum recommended sample size of 317 participants. However, because the study used self-administered questionnaires, a 25% buffer was added to maximise the response rate to obtain a final sample size of 396, which was increased to 400.
A line list of learners was arranged according to learner grade, and proportionate sample sizes of each grade were determined. For the selection of participants, the list of learners was arranged alphabetically by name before using the systematic random sampling technique, where every nth learner was selected. The n value was obtainable by dividing the total number of learners in each stratum by the required number of participants from each stratum.
Recruitment
The recruitment of participants started immediately after permission was granted by the KZN Department of Education. The researcher made an appointment with the principal to discuss the study and the logistics regarding access to the learners. The study was explained to the selected learners, and they were given informed consent to give to their parents to sign and return them to the school. Those who returned signed forms were recruited during breaks and in the afternoon. One classroom was allocated to the researcher, where a group of students assembled to answer the self-administered questionnaires.
Variables
The outcome variable was defined based on whether the participants had reported that they smoked cigarettes or not (smoking ‘yes’ and smoking ‘no’). The prevalence of smoking was calculated as the proportion of participants who were smoking out of the total number of the study participants. To investigate the factors associated with cigarette smoking, the smoking status variable was dichotomised into ‘yes’ and ‘no’ categories and used as the outcome or dependent variable in the regression analyses. Sociodemographic characteristics and the data related to smoking behaviours and influences of smoking were used as the explanatory (independent) variables.
Data analysis
The study used STATA version 17 software for the analysis of data. The authors described the sample using means and the standard deviations (s.d.) for continuous data and presented the categorical data as proportions and percentages. The Chi-square test was used in the cross-tabulation of the outcome variable, cigarette smoking status and the other independent variables, including the sociodemographic characteristics and information on smoking behaviours and influences of smoking. P values were used to indicate the statistical significance of the differences, p < 0.05. Univariable and multivariable logistic regression analyses were conducted to investigate the factors associated with smoking cigarettes. All variables yielding p values ≤ 0.20 from the binary regression analysis were included in multivariable regression analysis. The results were reported as adjusted odds ratios (AOR), with the corresponding 95% CIs. Associations yielding p values < 0.05 were considered statistically significant.
Validity and reliability
The question items of the data collection tool were adapted from previous studies. The tool was piloted on 5% of the required sample size from the same school before data collection. However, the pilot results were not included in the results of the main study. Minor modifications were made where necessary based on the participant responses.
Ethical considerations
This study obtained ethical approval from the research ethics committee of Sefako Makgatho University Health Sciences University (SMUREC/H/42/2022:PG). Permission to conduct the study was obtained from the KZN Department of Education (Ref:2/4/8/7322). All selected learners were notified about the study and were requested to give written informed consent through the signing of the informed consent form (ICF) and assent forms. The assent forms were signed by the parents or guardians of the learners who were aged below 18 years.
Results
Sociodemographic characteristics of the study participants
Table 1 shows the demographic characteristics of the 400 study participants. The majority, 54% (n = 225) were female. The mean age of the participants was 16 years and two standard deviations (± 2 [s.d.]), with 92.8% (371) participants who were between the ages of 12 and 18 years old. More than half, 51.8% (n = 207) were in Grades 9 and 11. Some, 57.3% (n = 227) were Christian. Additionally, 75.8% (n = 310) lived in semi-urban areas. Cigarette smoking was reported by 21% (n = 84) of the participants. The mean age at which participants started smoking was 14.8 years and 1.79 s.d. (14.8 ± 1.79).
Reasons for smoking cigarettes
Figure 1 reveals that 58% (49/84) of participants smoked cigarettes because they had a friend who was smoking. Other reasons for smoking include stress, 15.5% (13), 8.3% (n = 7) smoked for fun, 4.8% (n = 4) because of peer pressure, 3.6% (n = 3) had loneliness, 1.2% (n = 1) because of boredom and 1.2% (n = 1) did not state the reason for smoking cigarettes.
Reasons for smoking cigarettes, N = 84.
Smoking behaviours and influences of cigarette smoking
Table 2 shows the smoking behaviours and influences of smoking among the 84 cigarette smokers. Sixty per cent (50/83) had started smoking when they were between the ages of 12 and 15 years old, and these were mostly males, 61.0% vs. 59.4% female participants. Sixty-seven per cent (56/83) of participants were daily smokers, and there was no statistically significant difference between male and female participants, 39.3% female vs. 61% male participants, p = 0.69. A total of 74.1% (60/81) participants got the cigarettes from the shops, and these were mostly males, 60% vs. 40% female participants, p = 0.59. Of the 54/78 participants, 69.2% smoked in school, 40.7 % female vs. 59.3% male participants, p = 0.54. Ninety per cent (75/83) had a smoking friend, 38.7% female vs. 61.3% male participants, p = 1.00. Of the 66/84 smokers, 78.6% had a smoker in the family, and these were mostly male participants, 60.6% vs. 39.4% females, p = 0.64. Only 25% (21/84) belonged to a social club, and these were male participants, 81% vs. 19% females, statistically significant, p = 0.04. Ninety-three per cent (77/83) of the participants indicated an intention to quit smoking, 39% female vs. 61% male, p = 1.0.
Factors associated with cigarette smoking
Table 3 shows the results from the multivariate logistic regression analysis. Variables of sex, having a smoking family member, age of participants and religion had statistically significant associations with cigarette smoking. The odds of cigarette smoking were higher among males compared to females (AOR = 2.33; 95% CI: 1.29–4.17), p = 0.004, and among participants who had a smoking family member compared to those who did not have a smoking family member (AOR = 5.82; 95% CI: 3.08–11.0), p < 0.001. Family in the context of this study refers to parents, siblings, aunts, uncles and cousins. Lower odds of cigarette smoking were observed among participants who were aged between 12 and 15 years old (AOR = 0.04; 95% CI: 0.01–0.15), p < 0.001 compared to those who were aged ≥ 19 years old and among participants belonging to the Christian religion compared to those of other religions (AOR = 0.01;95% CI: 0.00–0.18), p = 0.002.
Discussion
Our study results on the prevalence and frequency of cigarette smoking were found to be comparable to the results reported from previous surveys conducted among adolescents and young adults in South Africa. These include a systematic review study of the prevalence of tobacco use among adolescents and young adults in South Africa, which found a pooled prevalence of tobacco use of 22% (Londani & Oladimeji 2024) and Zwane, Mashau and Moselakgomo (2022) found a higher percentage of 64.7% of learners who smoke cigarettes in the school premises. However, much lower and higher smoking prevalence of 4% and 33% have been reported, respectively, among high school and university students (Roble et al. 2021; Tezera & Endalamaw 2019). Surveys carried out in America also show a high prevalence of smoking among high school learners. In 2019, Wang found that 53.3% of high school learners and 24.3% of middle school learners reported that they had tried cigarette smoking. In 2022, a survey conducted by Gentzke found a decline of 34% in cigarette smoking among high school students and 11.3% of middle school students.
Participants in this study smoked cigarettes mostly because they had a smoking friend and were stressed. Similarly, others have reported a high likelihood of smoking among high school and university students because of smoking friends and peer pressure (Desai et al. 2019; Leshargie et al. 2019). Stress alleviation has also been cited as a reason for smoking among students at a large midwestern university (Nichter, Nichter & Carkoglu 2007). This finding of more than half of daily smokers among the smoking participants has been observed in other studies. These include a study that reported 51.2% of daily smokers. Others have, however, reported daily smoking among only 5.9% of the participants (Sun et al. 2022; Wamamili et al. 2019). This study also found that some of the smokers accessed cigarettes from the shops, while others used the cigarettes while at school. A study that was conducted among adolescents in India found school learners who purchased cigarettes from a shop nearby the school (Kedar & Gupta 2021).
This study investigated the factors that were associated with cigarette smoking and found high odds of cigarette smoking among the male participants. Those who had a smoking family member have been reported in other studies. These include a study which was conducted among high school students in Eastern Ethiopia, which reported 4.33 times higher odds among male learners compared to females (Roble et al. 2021).Another is a study which was conducted in Saudi Arabia, which found an increased likelihood of tobacco use among students who had at least one member of their family who smoked (Al-Makadma et al. 2015; Reda et al. 2012). However, others have reported no significant association between living with people who smoke cigarettes and adolescent smoking (Reda et al. 2012). In this study, the authors found stress, peer pressure and having fun, among other reasons for smoking. The study by Araújo (2019) resonates with our findings that pleasure, relaxation and manipulation were recorded among reasons for adolescents smoking. A significant proportion of participants who smoke expressed a desire to quit smoking in this study, especially males. Whereas in other studies, a higher percentage of both males and females were found to have difficulties in quitting smoking, with almost a quarter of smokers intending to quit (Marques-Vidal et al. 2011). Low odds of smoking were observed in this study among adolescents who were Christians or who belonged to other religious groups, and this is comparable with the study by Alexander et al. (2016), which found that black adolescents who had a stronger religious belief prevented them from smoking, which means the odds of smoking were low among this group.
Limitations
This study had limitations, these incudes a small sample size, which could potentially affect the statistical significance of some of the observed relationships. Since the data collected by this study was self reported, it could have introduced social desirability biases in smoking behaviours, potentially leading to an underestimation of the magnitude of the prevalence of cigarette smoking.
Conclusion and recommendations
The finding that the average smoking debut age among school learners is 14 years necessitates urgent national attention. South Africa has proposed a bill that would impose fines or sentences of up to 15 years in prison for anyone or any business that sells cigarettes to children under 18 years old. This bill aims to align with the WHO Framework Convention on Tobacco Control (FCTC) and could help reduce the sale of cigarettes to underage schoolchildren. The prevalence of cigarette smoking in schools indicates a significant gap in the enforcement of strict rules, which must be addressed. Additionally, the intent to quit smoking expressed by some of the smoking learners calls for the establishment of a school-based smoking cessation programme. This programme should be integrated into life orientation subjects, where students are taught about the dangers of smoking.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Al-Makadma, A.S., Moynihan, M., Dobson, S. & Saewyc, E., 2015, ‘Tobacco use among adolescents in Riyadh Saudi Arabia’, International Journal of Adolescent Medicine and Health 27(3), 357–360. 10.1515/ijamh-2014-002325153556 · doi ↗ · pubmed ↗
- 2Alexander, A.C., Robinson, L.A., Ward, K.D., Farrell, A.S. & Ferkin, A.C., 2016, ‘Religious beliefs against smoking among black and white urban youth’, Journal of Religion and Health 55(6), 1907–1916. 10.1007/s 10943-015-0128-026510855 PMC 4848172 · doi ↗ · pubmed ↗
- 3American Lung Association, 2024 a, Health effects of secondhand smoke, viewed 03 September 2023, from https://www.lung.org/quit-smoking/smoking-facts/health-effects/secondhand-smoke.
- 4American Lung Association, 2024 b, Tobacco use among children and teens, viewed 10 October 2024, from https://www.lung.org/quit-smoking/smoking-facts/impact-of-tobacco-use/tobacco-use-among-children#:~:text=Cigarette%20smoking%20during%20childhood%20and,6
- 5Araújo, A.J., 2019, ‘Reasons for smoking or reasons for quitting, that is the question: Can administering the modified reasons for smoking scale make a difference in clinical practice?’, Jornal Brasileiro de Pneumologia 45(4), e 20190253. 10.1590/1806-3713/e 2019025331411281 PMC 6733720 · doi ↗ · pubmed ↗
- 6Arrazola, R.A., 2017, ‘Current tobacco smoking and desire to quit smoking among students aged 13–15 years – Global youth tobacco survey, 61 countries, 2012–2015’, MMWR Morbidity and Mortality Weekly Report 66(20), 533–537. 10.15585/mmwr.mm 6620 a 328542119 PMC 5657874 · doi ↗ · pubmed ↗
- 7Asif, H.M., Akhtar, N., Sultana, S., Ahmad, K., Qureshi, T., Ateeb, M. et al., 2017, ‘Prevalence and factors related to cigarette smoking initiation and use among university students of Bahawalpur Pakistan: A cross sectional study’, RADS Journal of Pharmacy and Pharmaceutical Sciences 5(3), 11–16.
- 8Castro, E.M., Lotfipour, S. & Leslie, F.M., 2023, ‘Nicotine on the developing brain’, Pharmacological Research 190, 106716. 10.1016/j.phrs.2023.10671636868366 PMC 10392865 · doi ↗ · pubmed ↗