Left Ventricular Noncompaction in Advanced Heart Failure With an Anomalous Coronary Artery: A Case Report
Khaleel Quasem, Michelle Carrasquel, Jordan Felice, Britni Smith, Dania Baraka, Karam Khasawneh, Adam Quasem, Majid Mughal

TL;DR
This case report describes an older adult with late-onset left ventricular noncompaction and an unusual coronary artery anomaly, emphasizing the need for thorough imaging and tailored treatment in heart failure.
Contribution
The case expands understanding of LVNC by showing its late-onset potential and coexistence with an anomalous coronary artery in an older adult without familial history.
Findings
LVNC was diagnosed in a 77-year-old with nonischemic cardiomyopathy using echocardiography and MRI.
Anomalous left circumflex artery was identified, highlighting the need for comprehensive imaging in complex heart failure cases.
Multimodal treatment improved functional status and symptoms, with continued monitoring for device and disease progression.
Abstract
Left ventricular noncompaction (LVNC) involves abnormal development of the heart muscle, where the inner layer remains excessively trabeculated instead of compacting properly. Traditionally considered congenital, increasing reports of nonfamilial or sporadic LVNC suggest that adverse myocardial remodeling, such as from volume overload or preexisting cardiomyopathy, may contribute to its development. We present the case of a 77-year-old male with chronic atrial fibrillation and nonischemic cardiomyopathy who was found to have severe LVNC, identified on echocardiography and cardiac MRI using a noncompacted-to-compacted myocardial thickness ratio >2.3 at end-systole. Severe left ventricular dysfunction (ejection fraction (EF) <20%) was confirmed, and angiography revealed nonobstructive coronary disease with an anomalous left circumflex artery - an uncommon co-occurrence that underscores…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
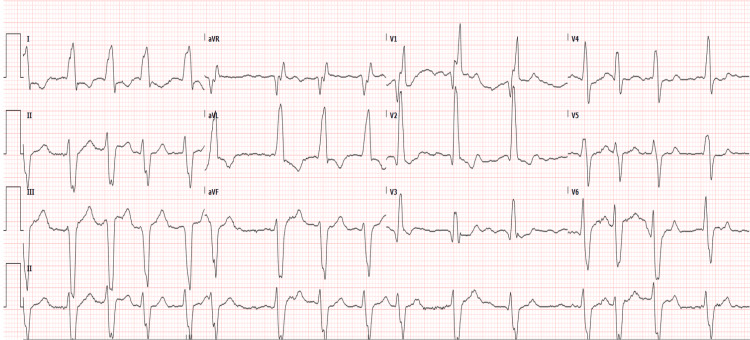 Figure 1
Figure 1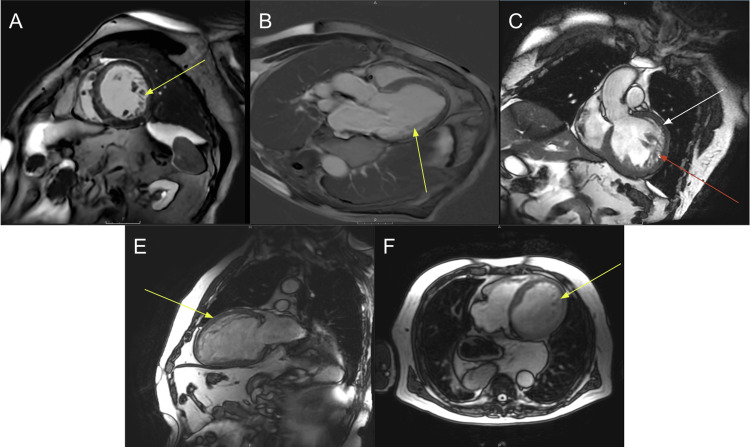 Figure 2
Figure 2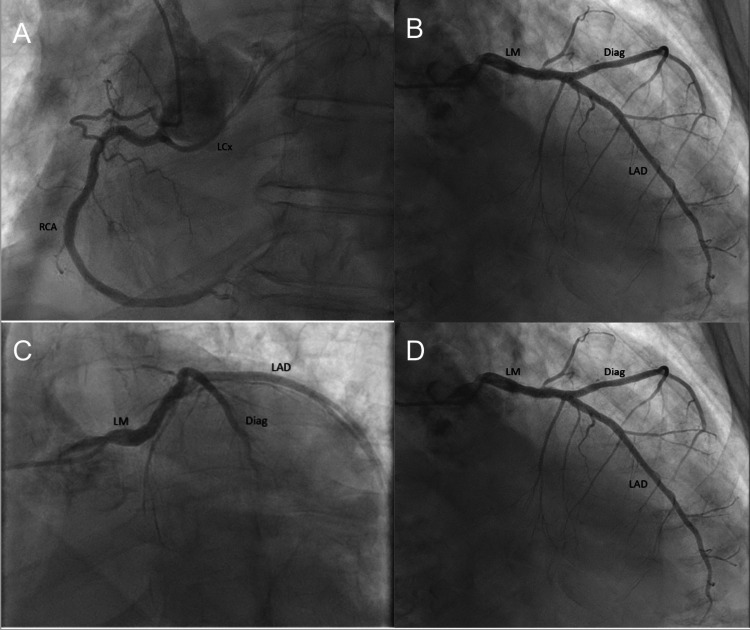 Figure 3
Figure 3| Vital sign | Value | Reference range |
| Heart rate | 111 bpm | 60-100 bpm |
| Respiratory rate | 20 breaths/min | 12-20 breaths/min |
| Blood pressure | 92/82 mmHg | 90/60-120/80 mmHg |
| Oxygen saturation | 93% | 96-100% |
| Category | Test | Value | Reference range |
| Hematology | WBC | 11.78 × 10⁹/uL | 4.0-11.0 × 10⁹/uL |
| Hgb | 16.3 g/dL | 13.5-17.5 g/dL | |
| Hct | 51.20% | 41-53% | |
| Platelets | 202 × 10³/µL | 150-450 × 10³/µL | |
| Electrolytes | Sodium | 142 mmol/L | 135-145 mmol/L |
| Potassium | 4.4 mmol/L | 3.5-5.0 mmol/L | |
| Chloride | 107 mmol/L | 96-106 mmol/L | |
| Calcium | 9.7 mg/dL | 8.5-10.5 mg/dL | |
| Magnesium | 2.3 mg/dL | 1.8-2.5 mg/dL | |
| CO₂ | 22.4 mmol/L | 22-29 mmol/L | |
| Anion gap | 12.6 mmol/L | 7-16 mmol/L | |
| Renal function | BUN | 30.7 mg/dL | 6-20 mg/dL |
| Creatinine | 1.9 mg/dL | 0.7-1.3 mg/dL | |
| eGFR | 36 mL/min/1.73 m² | >90 mL/min/1.73 m² | |
| Liver function | ALT | 79 U/L | 7-56 U/L |
| AST | 41 U/L | 10–40 U/L | |
| ALP | 109 U/L | 44-147 U/L | |
| Bilirubin total | 0.7 mg/dL | 0.1–1.2 mg/dL | |
| Cardiac function | NT-proBNP | 4,362 pg/mL | <125 pg/mL |
| hs-cTN | 59 ng/L | <20 ng/L |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCardiomyopathy and Myosin Studies · Cardiac Structural Anomalies and Repair · Cardiovascular Function and Risk Factors
Introduction
Left ventricular noncompaction (LVNC) is a rare cardiomyopathy characterized by excessive trabeculation of the myocardium, resulting from incomplete compaction of normal myocardial fibers [1]. This process creates a thick, noncompacted endocardial layer over a thinner compacted epicardium. While LVNC was traditionally considered a congenital disorder, emerging evidence suggests it can also be acquired, indicating a multifactorial etiology [2,3]. Myocardial remodeling due to volume overload or progressive changes in other cardiomyopathies has been proposed as a potential mechanism for acquired LVNC. This abnormal myocardial structure can lead to significant ventricular dysfunction, increasing the risk of heart failure, arrhythmias, and thromboembolic events - underscoring the importance of early detection and appropriate management [4].
LVNC presents along a broad clinical spectrum. Some individuals remain asymptomatic and receive a diagnosis incidentally, while others develop severe cardiac complications [1,2]. In some cases, arrhythmias serve as the initial clinical manifestation, preceding the onset of symptomatic heart failure or thromboembolic complications. These arrhythmias, ranging from atrial fibrillation to potentially life-threatening ventricular tachyarrhythmias, are thought to arise from structural irregularities that disrupt normal electrical conduction. Diagnosis relies on echocardiography and cardiac MRI [3,5]; however, distinguishing LVNC from other cardiomyopathies, such as dilated or hypertrophic cardiomyopathy with deep trabeculations, remains challenging due to overlapping structural and functional characteristics. Careful imaging interpretation, combined with clinical context, is essential for an accurate diagnosis.
Several factors influence the progression of LVNC to overt heart failure or significant arrhythmias, including the extent of noncompaction, left ventricular systolic dysfunction, underlying comorbidities (e.g., hypertension and coronary artery disease), and early manifestations of arrhythmias. Management primarily focuses on symptom relief, arrhythmia prevention, and thromboembolic risk reduction through anticoagulation. In advanced cases, implantable cardioverter-defibrillators (ICDs) or even heart transplantation may be necessary. Despite medical advancements, LVNC remains underrecognized and poorly understood, limiting the availability of robust data to refine management strategies.
Here, we present a unique case of LVNC that highlights the role of advanced diagnostic imaging, outlines the clinical course, and details the therapeutic approach, while also illustrating the rarity of LVNC coinciding with an anomalous coronary artery. This co-occurrence is clinically significant, as it underscores the potential for coexisting structural cardiac anomalies that may alter the presentation and management of LVNC. Comprehensive imaging was pivotal in detecting both the noncompacted myocardial segments and the anomalous coronary origin, guiding the subsequent treatment plan.
Case presentation
A 77-year-old male with a history of hypertension, paroxysmal atrial fibrillation, nonischemic cardiomyopathy (diagnosed approximately one year earlier but not extensively evaluated), and hyperlipidemia presented to the ED after several weeks of progressively worsening dyspnea. On arrival, he was tachycardic (heart rate: 111 bpm) and hypotensive (blood pressure: 92/82 mmHg), with a respiratory rate at the upper limit of normal (20 breaths/min) and an oxygen saturation of 93% on room air (Table 1).
An outpatient echocardiogram performed the previous year had shown a significantly dilated left ventricle with global hypokinesis, an estimated ejection fraction (EF) of 20-25%, and notably prominent trabeculations in the mid-lateral and apical walls. However, at that time, the possibility of LVNC had not been definitively investigated.
Upon presentation to the ED, a 12-lead EKG showed atrial fibrillation with a widened QRS complex (165 ms), consistent with right bundle branch block (Figure 1). Laboratory studies revealed mild leukocytosis (WBC 11.78 × 10⁹/uL), an elevated NT-proBNP level (4,362 pg/mL), and an increased high-sensitivity troponin (59 ng/L), suggestive of decompensated heart failure and ongoing myocardial stress (Table 2). Hemoglobin was 16.3 g/dL, and hematocrit was 51.2%, effectively ruling out true anemia. These findings, along with his hemodynamic instability, indicated an acute exacerbation of his chronic cardiac condition.
12-lead EKGA 12-lead EKG demonstrates atrial fibrillation with a ventricular rate of 95 bpm. The QRS complex is widened (165 ms), indicative of a likely right bundle branch block. QTc is within normal limits, with left axis deviation. No evidence of ST elevation or depression is observed.
A follow-up cardiac MRI performed during the admission confirmed extensive left ventricular trabeculations and quantified a noncompacted-to-compacted myocardial thickness ratio exceeding 2.3 in diastole (Figure 2), meeting the accepted diagnostic criteria for LVNC. Subsequent right and left heart catheterization revealed nonobstructive epicardial coronary artery disease, an anomalous left circumflex artery originating from the proximal right coronary artery (Figure 3), and elevated filling pressures, including a pulmonary artery systolic pressure of 50 mmHg. Given his severely reduced EF (<20%), low cardiac output (1.6 L/min), and index (0.8 L/min/m²), along with markedly elevated right-sided pressures, his presentation was consistent with an advanced stage of heart failure.
Cardiac MRI(A) Sagittal. (B) Short-axis apical. (C) Three-chamber vertical long axis. (D) Coronal. (E) Short-axis mid-diastole. (F) Axial.Cardiac MRI images reveal an increased trabeculated-to-non-compact myocardium in the left ventricle (yellow arrows). The ratio of non-compacted (white arrow) to compacted myocardium (red arrow) is 2.5.
Coronary angiography showing an anomalous left circumflex arteryThe LCX originates anomalously from the proximal RCA. It is a large-caliber but non-dominant vessel (A), giving rise to a medium-caliber first obtuse marginal branch, which further bifurcates in its proximal segment. The LM branches into the LAD and the Diag (A, B, C, D).Diag, diagonal artery; LAD, left anterior descending artery; LCX, left circumflex artery; LM, left main coronary artery; RCA, right coronary artery
Therapeutically, he received an amiodarone infusion for rate control of atrial fibrillation, along with his outpatient anticoagulation regimen (dabigatran). A transesophageal echocardiogram-guided cardioversion successfully restored normal sinus rhythm. Maintenance therapy included amiodarone (200 mg daily) and digoxin (125 mcg daily), in addition to sacubitril/valsartan (24/26 mg twice daily) and metoprolol succinate (25 mg daily) as guideline-directed medical therapy (GDMT) for heart failure with reduced EF. Given his profound left ventricular dysfunction, an ICD was planned for primary prevention of sudden cardiac death.
Although the new diagnosis of LVNC did not substantially alter the core management of systolic heart failure (i.e., GDMT), it emphasized the need for rigorous follow-up and device-based therapy. His case most likely represented a sporadic (nonfamilial) form of LVNC, given the late age at diagnosis, absence of known familial cardiomyopathy, and lack of LVNC features in first-degree relatives. If familial disease had been suspected, screening echocardiography for relatives would have been recommended. However, the patient’s advanced age and progressive structural changes - likely exacerbated by longstanding hypertension, atrial fibrillation, and a chronic cardiomyopathy of undetermined origin - support the concept of LVNC arising from adverse myocardial remodeling rather than a purely congenital or hereditary etiology.
Discussion
LVNC is increasingly recognized as a heterogeneous cardiomyopathy influenced by both genetic and acquired factors [1,2]. While embryological arrest in myocardial compaction has long been implicated, conditions such as longstanding hypertension or myocarditis may also contribute to adverse remodeling, leading to a noncompacted phenotype [2,3]. Genetic testing in LVNC frequently identifies mutations in genes such as MYH7, TTN, and LMNA, with early detection aiding in family screening and targeted interventions [1,4]. However, diagnosing LVNC remains challenging due to its overlapping features with dilated and hypertrophic cardiomyopathies, as well as evolving diagnostic criteria, including noncompacted-to-compacted ratio thresholds [2,5].
Patients exhibit varying degrees of heart failure symptoms, arrhythmias, and thromboembolic complications, posing therapeutic challenges. Arrhythmia management is particularly complex given the increased risk of ventricular tachyarrhythmias and syncope, alongside the progression of systolic dysfunction and the need for sudden cardiac death risk stratification. In this case, the patient’s severely reduced EF (<20%) and significant arrhythmic burden supported the decision to proceed with ICD placement [6,7]. Although atrial fibrillation was the primary contributor to the patient’s stroke risk, the morphological complexity of LVNC may also predispose non-atrial fibrillation patients to intracardiac thrombus, raising questions about prophylactic anticoagulation despite the absence of definitive guidelines [3]. Furthermore, the presence or absence of late gadolinium enhancement on MRI offers additional prognostic insights and may help guide advanced therapy decisions. While emerging approaches such as gene therapy, novel imaging techniques, and left ventricular assist devices hold promise, their optimal integration into LVNC management remains uncertain [5,8,9].
Although coronary angiography in this patient revealed an anomalous origin of the left circumflex artery, this structural anomaly - one of the more commonly encountered coronary variants - did not significantly impact ischemic risk or require specific intervention, making it largely incidental. Nonetheless, certain coronary anomalies can complicate LVNC management by introducing additional ischemic considerations or affecting surgical planning. In this case, recognizing that the patient’s preexisting cardiomyopathy and atrial fibrillation warranted further evaluation ultimately led to the correct diagnosis of LVNC via echocardiography and cardiac MRI. If the condition had been familial, formal screening of relatives would have been recommended; however, the patient’s late age at diagnosis and lack of family history suggest a sporadic presentation. These findings underscore the critical role of multimodality imaging, comprehensive arrhythmia management, and individualized heart failure therapies in optimizing outcomes for LVNC patients, while also highlighting areas of ongoing investigation, such as prophylactic anticoagulation, ICD criteria for EFs above 35%, and the role of advanced therapies.
Conclusions
In this case, an older adult with chronic atrial fibrillation and preexisting nonischemic cardiomyopathy was diagnosed with LVNC, highlighting the potential for a later-life, nonfamilial presentation likely influenced by adverse myocardial remodeling. Multimodality imaging, including echocardiography, cardiac MRI, and coronary angiography, was crucial not only for confirming the diagnosis and assessing noncompaction severity but also for identifying coexisting anomalies such as the anomalous left circumflex artery. These findings emphasize the importance of comprehensive cardiac evaluation in patients with atypical or progressive heart failure, particularly in the presence of arrhythmias, and reinforce the value of guideline-directed pharmacotherapy, rate or rhythm control, and ICD placement in reducing the risk of sudden cardiac death.
Despite the insights gained from this case, important challenges remain. LVNC’s highly variable presentation continues to blur its diagnostic boundaries, leading to underdiagnosis, particularly in older populations. Further large-scale studies are needed to refine imaging criteria, clarify indications for prophylactic anticoagulation, especially in non-atrial fibrillation patients, and explore the role of genetic testing and emerging therapies in guiding more personalized care. Addressing these gaps will help optimize treatment strategies, improve risk assessment, and enhance long-term outcomes for individuals with this rare but clinically significant cardiomyopathy.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Isolated noncompaction of left ventricular myocardium. A study of eight cases Circulation Chin TK Perloff JK Williams RG Jue K Mohrmann R 507513821990237289710.1161/01.cir.82.2.507 · doi ↗ · pubmed ↗
- 2Trabeculation in the embryonic heart Bioessays Sedmera D Thomas PS 607181996875793910.1002/bies.950180714 · doi ↗ · pubmed ↗
- 3Left ventricular non-compaction: insights from cardiovascular magnetic resonance imaging J Am Coll Cardiol Petersen SE Selvanayagam JB Wiesmann F 1011054620051599264210.1016/j.jacc.2005.03.045 · doi ↗ · pubmed ↗
- 4Isolated ventricular non-compaction of the myocardium in adults Heart Jenni R Oechslin EN van der Loo B 11159320071667009810.1136/hrt.2005.082271 PMC 1861330 · doi ↗ · pubmed ↗
- 5ACC/AHA/HRS 2008 guidelines for device-based therapy of cardiac rhythm abnormalities: a report of the American College of Cardiology/American Heart Association task force on practice guidelines (writing committee to revise the ACC/AHA/NASPE 2002 guideline update for implantation of cardiac pacemakers and antiarrhythmia devices): developed in collaboration with the American Association for Thoracic Surgery and Society of Thoracic Surgeons Circulation Epstein AE Di Marco JP Ellenbogen KA 0408117200810 · doi ↗ · pubmed ↗
- 6Left ventricular non-compaction revisited: a distinct phenotype with genetic heterogeneity?Eur Heart J Oechslin E Jenni R 144614563220112128507410.1093/eurheartj/ehq 508 · doi ↗ · pubmed ↗
- 7Isolated noncompaction of the left ventricular myocardium in adults: a systematic overview J Card Fail Bhatia NL Tajik AJ Wilansky S Steidley DE Mookadam F 7717781720112187214810.1016/j.cardfail.2011.05.002 · doi ↗ · pubmed ↗
- 8Noncompaction cardiomyopathy: a current view Arq Bras Cardiol Rosa LV Salemi VM Alexandre LM Mady C 0997201110.1590/s 0066-782x 201100090002121894393 · doi ↗ · pubmed ↗