Antiphospholipid antibody-associated cystic lesion of the pancreatic head with concurrent acute pancreatitis
Junxian Hong, Shikai Hu, Jiuliang Zhao, Yangzhong Zhou

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
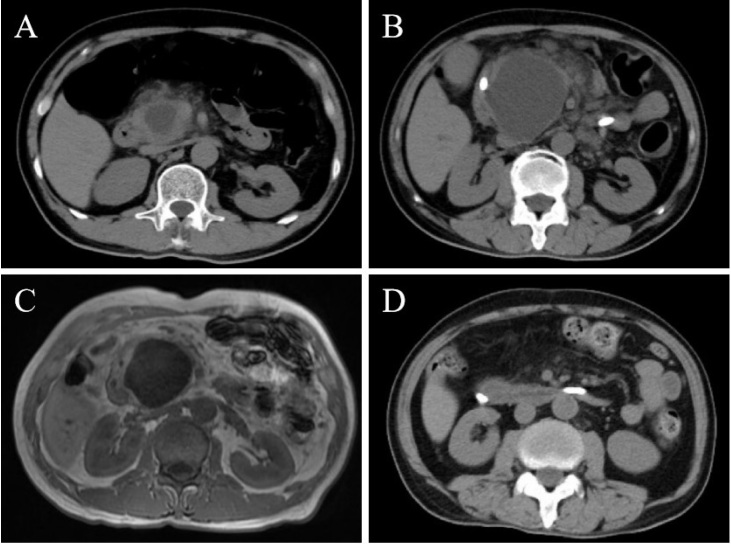 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsIgG4-Related and Inflammatory Diseases · Pancreatitis Pathology and Treatment · Systemic Lupus Erythematosus Research
A 58-year-old male presented with an 8-day history of severe upper abdominal pain and vomiting. His medical history was unremarkable, with a normal abdominal computed tomography (CT) six months prior. Laboratory tests revealed elevated serum amylase, lipase, C-reactive protein, and D-dimer levels. CT scan identified a well-circumscribed 36 mm × 26 mm cystic lesion within the pancreatic head with peripancreatic exudation (Figure 1A). Despite supportive treatment for pancreatitis, symptoms persisted. Over two weeks, the lesion progressively enlarged to 67 mm × 49 mm on CT and magnetic resonance imaging (MRI), with branch pancreatic duct dilation (Figure 1B-C). Conventional etiologies such as biliary obstruction, hypertriglyceridemia, alcohol, drugs, or infection were excluded. An autoimmune workup revealed a normal immunoglobulin G4 (IgG4) level but positive antiphospholipid antibodies (aPL: Lupus anticoagulant (LA) 1.41 [positive: > 1.20]; anticardiolipin antibody (ACL)-IgM, 12.5 IgM phospholipid units (MPLU)/mL [positive: > 12.0]; beta-2 glycoprotein 1 (β2GP1)-IgM 60.1 AU/mL [positive: > 24.0]). The cystic lesion, inconsistent with intraductal papillary mucinous neoplasm (IPMN) or pseudocyst, led to the diagnosis of aPL-associated pancreatic cystic lesion with concurrent acute pancreatitis. Thromboembolic screening was negative. Methylprednisolone (40 mg/day) and low-molecular-weight heparin (4000 U/day) were administered, along with biliary and pancreatic duct stenting. As symptoms resolved, medications were tapered. Follow-up imaging demonstrated marked cyst regression (Figure 1D). Repeated testing after three months confirmed persistent aPL positivity (LA 1.28, ACL-IgM 14.9 MPLU/mL, β2GP1-IgM 42.6 AU/mL).
This case highlights a rare manifestation of patients with aPL positivity, as pancreatic involvement occurs in ~0.5% of antiphospholipid syndrome (APS) patients.^[1]^ While pancreatitis is common, aPL-associated cystic lesions are unusual but clinically significant.^[2, 3, 4]^ The proposed mechanism involves aPL-mediated microvascular thrombosis, leading to ischemic necrosis, inflammation, and cystogenesis.^[1,5]^ Persistent aPL positivity and therapeutic responsiveness further support aPLs as the etiology. This case underscores the importance of recognizing the diverse organ involvement and micro-vascular pathology of APS. Early identification and targeted treatment addressing inflammation and thrombosis can significantly benefit patients in such scenarios.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Zhang J Li C Han X The digestive system involvement of antiphospholipid syndrome: pathophysiology, clinical characteristics, and treatment strategies Ann Med 202153132813393440989410.1080/07853890.2021.1962964 PMC 8381908 · doi ↗ · pubmed ↗
- 2Nesher G Breuer GS Temprano K Lupus-associated pancreatitis Semin Arthritis Rheum 2006352602671646107110.1016/j.semarthrit.2005.08.003 · doi ↗ · pubmed ↗
- 3Nguyen HC Dimou A Govil A Primary antiphospholipid syndrome and necrotizing pancreatitis: a diagnostic challenge J Clin Rheumatol 2013193483502396547510.1097/RHU.0b 013e 31829 cef 33 · doi ↗ · pubmed ↗
- 4Savey L Piette JC Bellanger J Catastrophic antiphospholipid syndrome (CAPS)-induced ischemic pancreatic ducts injury mimicking intraductal papillary mucinous neoplasm (IPMN)Se-min Arthritis Rheum 20184756556810.1016/j.semarthrit.2017.07.00128802775 · doi ↗ · pubmed ↗
- 5Dellamonica J Tieulie N Bernardin G Pancreatitis due to catastrophic antiphospholipid syndrome Pancreas 2007343803811741406510.1097/MPA.0b 013e 3180325 bc 1 · doi ↗ · pubmed ↗