Comparison of Intra-articular Haematoma Block and Procedural Sedation for the Manipulation of Closed Ankle Fracture Dislocations: A Cross-Sectional Study
Mahmoud Elmesalmi, Zeid Morcos, John Mcfall, Fadi Hindi, Khaled F Al-Kharouf, Togay Koç

TL;DR
This study compares two methods for reducing ankle fractures and finds that a local injection is as effective and cheaper than sedation.
Contribution
Demonstrates that intra-articular haematoma block is a viable, cost-effective alternative to procedural sedation for ankle fracture reduction.
Findings
No significant differences in pain scores between the two methods.
IAHB had lower costs and faster treatment times compared to procedural sedation.
Abstract
Background Ankle fracture dislocations are commonly reduced in the emergency setting under procedural sedation (PS), which requires trained clinicians and monitoring. This study aimed to evaluate the patient-reported efficacy of intra-articular haematoma block (IAHB) as an analgesic alternative to PS for the closed reduction of ankle fracture dislocations. Methods Data from patients with displaced ankle fractures requiring manipulation between October 2020 and April 2021 were analysed. Patients who received IAHB were compared to those who received PS. IAHB involved the injection of 10 mL of 1% lignocaine into the joint space. Results Twenty-eight patients received PS, and 25 received IAHB. There were no statistically significant differences in visual analogue scale (VAS) scores before, during, or after treatment (p > 0.05). First-attempt reductions were successful in 76% of IAHB…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
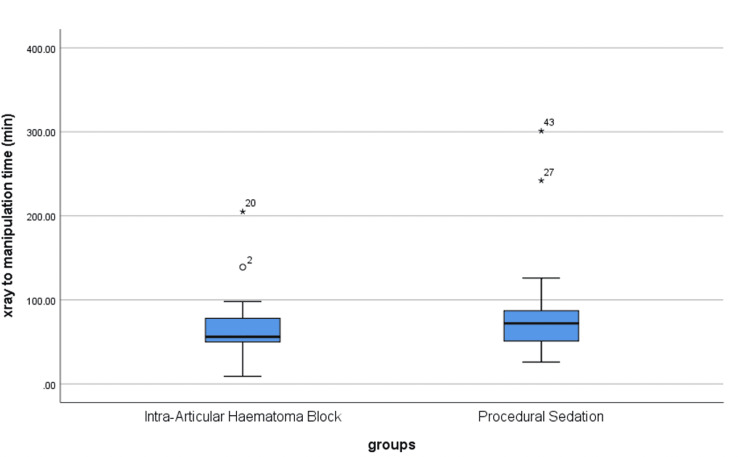 Figure 1
Figure 1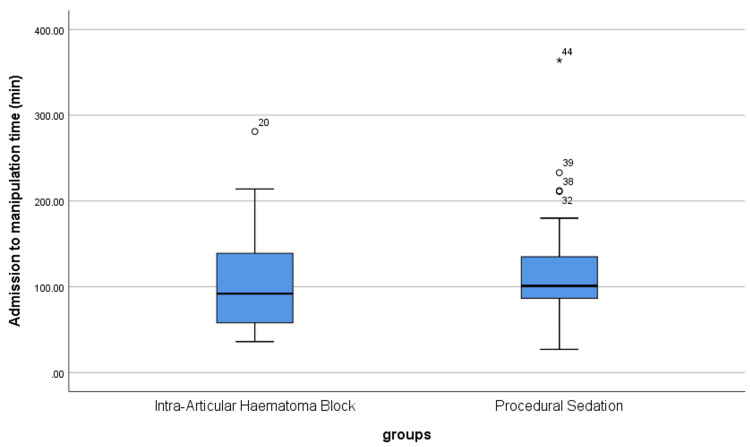 Figure 2
Figure 2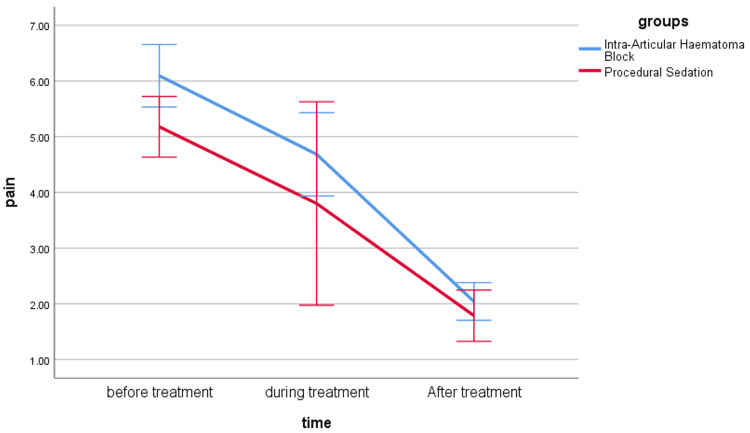 Figure 3
Figure 3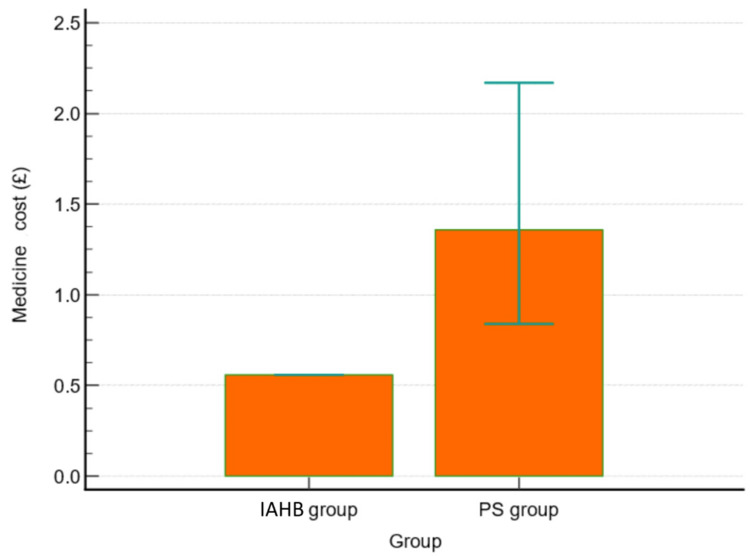 Figure 4
Figure 4| Intra-articular haematoma block (N = 25) | Procedural sedation (N = 28) | p-value | |
| Age in years | 57.8 ± 19.16 | 55.14 ± 17.21 | 0.590 |
| Number of clinicians involved | 0.002 | ||
| Two | 1 (4.0%) | 0 (0.0%) | |
| Three | 22 (88.0%) | 14 (50.0%) | |
| Four | 2 (8.0%) | 9 (32.1%) | |
| Five | 0 (0.0%) | 5 (17.9%) | |
| On-call orthopaedic team involved | 20 (80.0%) | 21 (75.0%) | 0.660 |
| Median (IQR) X-ray to manipulation time (minutes) | 56 (48-78) | 72 (50.5- 87) | 0.173 |
| Median (IQR) admission to manipulation time (minutes) | 92 (57.5- 139) | 101 (86.25- 135) | 0.387 |
| Time spent in the ED (minutes) | 286.65 ± 126.88 | 247.89 ± 89.49 | 0.230 |
| Intra-articular haematoma block | Procedural sedation | p-value | |
| Preoperative VAS pain | 6.10 ± 2.80 | 5.18 ± 2.88 | 0.250 |
| Pain during reduction | 4.68 ± 3.74 | 3.80 ± 4.09 | 0.640 |
| Postoperative VAS pain | 2.04 ± 1.70 | 1.79 ± 2.44 | 0.670 |
| Intra-articular haematoma block (N = 25) | Procedural sedation (N = 28) | p-value | |
| Satisfactory reduction first attempt | |||
| Yes | 19 (76.0%) | 23 (82.1%) | 0.582 |
| No | 6 (24.0%) | 5 (17.9%) | |
| Further manipulation | 5 (20%) | 1 (3.6%) | 0.062 |
| Satisfactory reduction second attempt | 3 (12%) | 0 (0.0%) | 0.061 |
| Intra-articular haematoma block | Procedural sedation | p-value | |
| 1% lignocaine (mL) (n = 25) | 10.2 ± 1.0 | -- | -- |
| Ketamine (mg) (N = 13) | -- | 72.7 ± 20.4 | -- |
| Propofol (mg) (N = 14) | -- | 77.9 ± 47.9 | -- |
| Fentanyl (mcg) (N = 13) | -- | 79.2 ± 48.6 | -- |
| Ketamine (£) (N = 13) | -- | 1.08 ± 0.53 | -- |
| Propofol (£) (N = 14) | -- | 1.23 ± 0.76 | -- |
| Fentanyl (£) (N = 13) | -- | 1.03 ± 0.8 | -- |
| Total cost of medicines (£) | 0.56 (0.56-0.84) | 1.4 (0.6-4.7) | <0.001 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsOrthopedic Surgery and Rehabilitation · Anesthesia and Pain Management · Patient Safety and Medication Errors
Introduction
Orthopaedic injuries requiring manipulation can be resource-intensive for emergency departments (EDs), especially when conscious procedural sedation (PS) is needed [1]. The Royal College of Emergency Medicine [2] mandates that conscious sedation be administered by an appropriately trained clinician with a skilled assistant, along with safe monitoring. Thus, the availability of appropriately trained clinicians and a monitored bed space in our increasingly busy EDs can impact manipulation times. Patient factors, such as fasting status and comorbidities, can also affect the suitability of PS.
With the devolution of musculoskeletal practice in our EDs over the years, advanced and emergency nurse practitioners (ANPs/ENPs) [3] now possess the skills to perform manipulations, but the bottleneck remains the anaesthesia. Haematoma blocks for distal radius fractures are routinely performed nationwide with good results [4,5].
In 2002, Miller et al. prospectively randomized 30 patients with isolated glenohumeral joint dislocations to undergo closed reduction with the use of either intra-articular lidocaine or intravenous sedation [6]. There were no significant differences in pain scores (p = 0.37) or the ability to reduce the shoulders. However, patients receiving PS spent significantly longer in the ED (185 vs 75 minutes), with an average cost of 0.52 for the lidocaine group [6].
White et al. conducted what is believed to be the first prospective randomized trial comparing intra-articular haematoma blocks (IAHBs) with conscious sedation for 42 closed reductions of ankle fracture dislocations [4]. Using a visual analogue scale (VAS) score, both groups achieved a statistically significant reduction in pain (IAHB, 9.2 to 3.6; PS, 9.3 to 4.1) with no significant difference between the two methods. They also stated that both methods provided similar levels of analgesia during the manipulation, but offered no supporting data. They did not find a significant difference in the time taken to deliver patient care. The IAHB group required six further manipulations, while the PS group required two (p = 0.15). White et al. demonstrated that intra-articular injection of local anaesthetics delivers a similar degree of analgesia to conscious sedation [4].
Furia et al. and Alioto et al. together report using IAHB on 23 patients without any episodes of associated infection [5,7]. Additionally, local anaesthetic chondrotoxicity has been well documented in vitro, with local anaesthetics exhibiting dose- and time-dependent cytotoxic effects [5,7].
The primary outcome of this study was to assess the patient-reported efficacy of IAHB as analgesia for the closed reduction of ankle fracture dislocations in a large, busy British NHS Hospital, compared to PS. Secondary outcomes included time to manipulation, efficiency of patient flow through the ED, economic evaluation, and manipulation success.
Materials and methods
This study included a total of 53 patients presenting with displaced ankle fractures requiring manipulation under anaesthesia (MUA). A cross-sectional design was employed, with prospective data collection for 25 patients undergoing IAHB from October 2020 to April 2021 and a retrospective analysis of 28 patients who underwent PS for ankle fracture manipulation over a six-month period from March to August 2020. All patients underwent a comprehensive medical history assessment, including injury mechanism and cause, and a clinical examination focusing on tenderness, swelling, and ankle joint movement limitations. Anteroposterior (AP) and lateral X-rays were performed prior to closed reduction. Pain was evaluated using VAS [8] before, during, and after reduction. Data included the number of clinicians involved, time from initial X-ray to reduction (or from the presentation if initially seen at a satellite minor injury unit (MIU)), success rate of reduction, and number of reduction attempts. Medications and their respective volumes were documented to calculate the total cost of medications. The cost was determined by multiplying the unit cost of each medication (per mg, mL, or mcg) by the quantity used. The following unit costs were applied: ketamine at £0.014 per mg, propofol at £0.015 per mg, fentanyl at £0.0143 per mcg, and lignocaine at £0.56 per 10 mL.
Data for the IAHB group were collected from written forms filled out by the clinician, while data for the PS group were collected from electronic ED documentation. The X-rays were compared using Picture Archiving and Communication System (PACS).
The IAHB technique involved injecting 10 mL of 1% lignocaine into the joint space via a medial approach adjacent to the tibialis anterior tendon, performed by a trauma and orthopaedic middle-grade clinician or ANP trained in the procedure, while PS was conducted in the ED by emergency physicians using agents such as propofol, ketamine, or benzodiazepines based on the clinical assessment. The study population included adult patients aged 18 years and older, with displaced ankle fractures requiring MUA, excluding those with open fractures, skin-threatening injuries, neurovascular compromise, or polytrauma.
Statistical analysis was conducted using IIBM SPSS Statistics for Windows, Version 27 (Released 2020; IBM Corp., Armonk, NY, United States). Categorical variables were presented as counts and percentages and compared between groups using Pearson’s chi-square test or Fisher’s exact test when more than 25% of cells had a count of <5. Quantitative variables, such as pain scores, were analysed using the Wilcoxon signed-rank test, while temporal variables were assessed using the Mann-Whitney U test. A p-value of <0.05 was considered statistically significant.
This study employs a combination of retrospective and prospective audit methodologies using non-identifiable data, ensuring no risk to the patients involved. Consequently, ethical approval was not required. The study was conducted in the Orthopaedics Department at Queen Alexandra Hospital, Portsmouth, Hampshire, UK, and was registered with the institutional governance team as a service evaluation.
Results
Patient characteristics, clinician involvement, and time metrics
The mean age was 57.8 ± 19.16 years in the IAHB group and 55.14 ± 17.21 years in the PS group (p = 0.59). The number of clinicians involved was significantly higher in the PS group than in the IAHB group (p = 0.002). There were no statistically significant differences between both groups regarding time from X-ray to manipulation, time from admission to manipulation, and time spent in the ED (p > 0.05) (Table 1, Figure 1, Figure 2).
Time from X-ray to manipulation in both groups
Time from admission to manipulation in both groups
Pain assessment using VAS scores
There were no statistically significant differences between both groups in VAS scores before, during, and after treatment (p > 0.05) (Table 2, Figure 3).
Line chart for repeated measurements for VAS pain score in both groups
Reduction success and further manipulations
There was no statistically significant difference in satisfactory first-attempt reduction rate between the IAHB group (19 patients, 76.0%) and PS group (23 patients, 82.1%) (p = 0.582). In the IAHB group, six patients had unsatisfactory first attempts at reduction. Five of the six went on to have further manipulation under the same block. Three of them were satisfactory at the second attempt, while one underwent MUA and plaster the following day and the other failed manipulation under PS and went for fixation the following morning. In the PS group, five patients had unsatisfactory first attempts at reduction. One had two further episodes of PS, but the reduction was still unsatisfactory, so the patient underwent fixation the same day. The remaining four patients had no more attempts at reduction under PS and all went on to have external fixation (three patients) or open reduction and internal fixation (one patient) within 24 hours. There was no significant difference in the number of unsatisfactory reductions between the groups (Table 3).
Medication volume and cost
In the IAHB group, the mean volume of 1% lignocaine used prior to manipulations was 10.2 ± 1.0 ml. In the PS group, 72.7 ± 20.4 mg of ketamine was used in 13 patients, and 79.2 ± 48.6 mcg of fentanyl was used in 13 patients. Additionally, propofol (77.9 ± 47.9 mg) was used in 14 patients. The cost of medications was significantly higher in the PS group, with a median of £1.4 (0.6-4.7), compared to £0.56 (0.56-0.84) in the IHAB group (p < 0.001) (Table 4, Figure 4).
Box plot for total cost of medicines (£) in both groupsIAHB: intra-articular haematoma block, PS: procedural sedation.
Discussion
This study found that IAHB provides comparable analgesia to PS for the closed reduction of ankle fracture dislocations. There were no statistically significant differences before, during, and after procedural pain scores between the study groups, aligning with findings from Alioto et al. and White et al. [4,7]. The first-attempt reduction success rate was also similar, with 76% for IAHB and 82.1% for PS. While six patients had a failed first attempt, three of them had satisfactory second-attempt reduction under the same block, while one patient in the IAHB group had an unsatisfactory second attempt under the same block. Notably, another patient in the IAHB group who also had an unsatisfactory second attempt failed even after sedation. In contrast, five patients in the PS group required urgent operative intervention. These results suggest that while both methods are comparable for initial reduction attempts, the IAHB group showed fewer subsequent failures requiring emergency surgery. Our study showed no statistically significant differences between the groups regarding time from X-ray to manipulation, time from admission to manipulation, and time spent in the ED.
Ankle fracture dislocations are common injuries managed in the ED [9,10]. PS carries a risky complication profile, particularly when conducted in hospitals with limited staff and resources, deep sedation in elderly patients with significant comorbidities, or during overnight hours [11]. IAHB is a regional anaesthetic technique that can be used among selected patients to minimize the anticipated complications of PS [12]. IAHB provides an equivalent amount of analgesia to conscious sedation among patients with closed ankle fracture dislocation, with lower cardiovascular risk, reduced cost, and timelier intervention [13]. The first study on the IAHB technique was conducted by Alioto et al. in 1995 [7]. They reported that the haematoma block is a safe, effective, and low-cost procedure for patients with closed ankle fractures [7]. Similar findings were reported by White et al. [4], who conducted a prospective randomized study with 42 patients with ankle fracture dislocation randomly assigned to two groups: continuous sedation and intra-articular lidocaine block. They found that there was no statistically significant difference between the study groups in terms of pain scores [4]. Conversely, our findings were inconsistent with MacCormick et al. [14], who retrospectively reviewed 221 patients who underwent IAHB and 114 patients who underwent PS. They found that first-attempt reduction was significantly lower among the IAHB group (54.8%) compared to the PS group (74%). However, there was only one case of respiratory depression in the PS group. The superiority of IAHB was mainly among patients who had ankle fractures with accompanying joint subluxation [14].
We found that the number of clinicians involved was significantly higher in the PS group than in the IAHB group. The cost of medications was 2.5 times higher in the PS group compared to the IAHB group, with median costs of £1.40 and £0.56, respectively. These findings were comparable to those provided by MacCormick et al. [14], who reported a mean cost of 220 for PS. They also compared outcomes between orthopaedic surgeons and ED clinicians, showing that successful reduction rates at the first attempt were significantly higher among orthopaedists compared to ED clinicians [14]. We believe that IAHB may have a role in the initial management of ankle fractures in well-equipped, high-volume hospitals in central areas and large cities, as well as during pandemics such as COVID-19, where it offers the advantage of avoiding aerosol-generating procedures. Additionally, it may be useful in low-resourced healthcare facilities, including hospitals with a shortage of medical staff. For patients in whom IAHB is unsuccessful, PS can be considered, potentially reducing overall costs. Advantages of this method include limiting the requirement for designated clinical space and the need for qualified clinicians to administer sedation, as well as the ability to re-manipulate under the same block.
The limitations of this study include being a single-institution study and not categorizing patients based on gender and the severity and extent of ankle injury. Additionally, cost analysis did not include monitoring expenses, operating room utilization, and attending physicians’ fees. Future outcomes, such as whether the patient eventually required an operation or not, were not considered. Furthermore, the absence of gender data is a minor limitation. Additionally, the study design presents a limitation, as one group was assessed prospectively while the other was analysed retrospectively. A fully prospective approach would enhance comparability. Future research should consider a strictly prospective design to strengthen these findings.
Conclusions
IAHB appears to be an efficacious, safe, and inexpensive technique for providing analgesia during the manipulation of closed ankle fracture dislocations in emergency settings. It is a simple and rapid procedure that can be performed by orthopaedic and emergency care practitioners, making it particularly valuable in busy or resource-limited institutions. The choice of method should be tailored to the patient's comorbidities, as well as the availability of staff and resources. PS carries a risky complication profile particularly when conducted in hospitals with limited staff and resources. We recommend conducting a national-level study to further evaluate the role of IAHB as a timely and accessible intervention for ankle fracture dislocations.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Procedural sedation and analgesia for adults in the emergency department BMJ Atkinson P French J Nice CA 0348201410.1136/bmj.g 296524812113 · doi ↗ · pubmed ↗
- 2Haematoma block: a safe method for pre-surgical reduction of distal radius fractures J Orthop Surg Res Maleitzke T Plachel F Fleckenstein FN Wichlas F Tsitsilonis S 3511520203284304310.1186/s 13018-020-01819-y PMC 7448324 · doi ↗ · pubmed ↗
- 3Practice standards for the emergency nurse practitioner specialty Adv Emerg Nurs J Campo TM Comer A Dowling Evans D 2402454020183036543710.1097/TME.0000000000000209 · doi ↗ · pubmed ↗
- 4Intra-articular block compared with conscious sedation for closed reduction of ankle fracture-dislocations. A prospective randomized trial J Bone Joint Surg Am White BJ Walsh M Egol KA Tejwani NC 7317349020081838130810.2106/JBJS.G.00733 · doi ↗ · pubmed ↗
- 5The efficacy and safety of the hematoma block for fracture reduction in closed, isolated fractures Orthopedics Furia JP Alioto RJ Marquardt JD 42342620201310.3928/0147-7447-19970501-119172249 · doi ↗ · pubmed ↗
- 6Comparison of intra-articular lidocaine and intravenous sedation for reduction of shoulder dislocations: a randomized, prospective study J Bone Joint Surg Am Miller SL Cleeman E Auerbach J Flatow EL 213521398420021247369910.2106/00004623-200212000-00002 · doi ↗ · pubmed ↗
- 7Hematoma block for ankle fractures: a safe and efficacious technique for manipulations Journal of orthopaedic trauma Alioto RJ Furia JP Marquardt JD 11311691995 https://journals.lww.com/jorthotrauma/abstract/1995/04000/Hematoma_Block_for_Ankle_Fractures__A_Safe_and.4.aspx 777602910.1097/00005131-199504000-00004 · doi ↗ · pubmed ↗
- 8Graphic representation of pain Pain Scott J Huskisson EC 17518421976 http://I would like to formally thank my supervising consultant and peers for their advice and support with this project.1026900 · pubmed ↗