Intentions for post-abortion contraceptive use among women who received abortion services in health facilities of Harar city and Dire Dawa city
Meron Degefa, Nega Assefa, Merga Deresa, Dawit Abebe, Sinetibeb Mesfin

TL;DR
This study examines the intention of women in Ethiopia to use contraception after an abortion and identifies factors influencing this decision.
Contribution
The study identifies key behavioral and demographic factors associated with post-abortion contraceptive intentions in a specific regional context.
Findings
74.7% of women expressed intention to use post-abortion contraception.
Positive attitude and perceived behavioral control were strongly associated with contraceptive intention.
Divorced women and those with wanted pregnancy abortions were less likely to intend contraceptive use.
Abstract
A woman's specific beliefs about contraceptives influence her engagement and adherence to these methods. The intention to use post-abortion contraceptive methods is a critical aspect of reproductive health, particularly for women who have undergone abortion procedures. The use of less effective contraceptive methods, inconsistent usage, and discontinuation significantly contribute to unintended pregnancies, which are a primary cause of abortion. Studies indicate low contraceptive utilization and a high prevalence of abortion in the study area. Therefore, this study aimed to assess the intention to use post-abortion contraceptives and the associated factors among women visiting health facilities for abortion services, utilizing a behavioral model. To assess intention to use post abortion contraceptive use and associated factors among women visiting health facilities for abortion…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
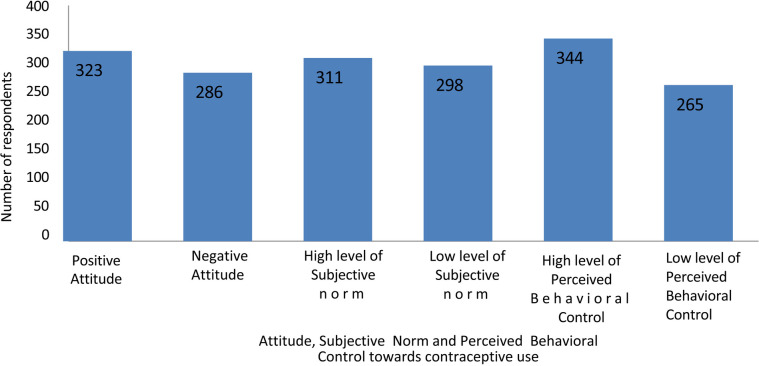 Figure 1
Figure 1| Variables | Categories | Number | Percentage (%) |
|---|---|---|---|
| Age( | 15–19 | 92 | 15.1 |
| 20–24 | 203 | 33.3 | |
| 25–29 | 183 | 30.0 | |
| 30–34 | 94 | 15.4 | |
| ≥35 | 37 | 6.1 | |
| Marital status ( | Single | 253 | 41.5 |
| Married | 321 | 52.7 | |
| Divorced | 35 | 5.7 | |
| Duration of marriage ( | <5year | 162 | 50.5 |
| 6–10 years | 100 | 31.2 | |
| >10 years | 59 | 18.4 | |
| Religion ( | Muslim | 277 | 45.5 |
| Orthodox | 222 | 36.5 | |
| Other* | 110 | 18 | |
| Level of education ( | No formal education | 89 | 14.6 |
| Primary(1–8) | 123 | 20.2 | |
| Secondary(9–10) | 181 | 29.7 | |
| Preparatory & above | 216 | 35.5 | |
| Ethnic group ( | Oromo | 263 | 43.2 |
| Amhara | 187 | 30.7 | |
| Somali | 46 | 7.6 | |
| Harari | 34 | 5.6 | |
| Tigray | 38 | 6.2 | |
| Other** | 41 | 6.7 | |
| Residence ( | Rural | 130 | 21.3 |
| Urban | 479 | 78.7 | |
| Occupation ( | Housewife | 194 | 31.9 |
| Gov'tal employer | 91 | 14.9 | |
| Some job/private | 117 | 19.2 | |
| Student | 184 | 30.2 | |
| Other*** | 23 | 3.8 |
| Variable | Categories | Number | Percentage (%) |
|---|---|---|---|
| Previous obstetrics related variables | |||
| Number of children ( | No child | 309 | 50.7 |
| 1–2 | 163 | 26.8 | |
| ≥3 | 137 | 22.5 | |
| Previous abortion history ( | Yes | 103 | 16.9 |
| No | 506 | 83.1 | |
| Previous contraceptive history related factors | |||
| Information about contraceptive ( | Yes | 526 | 86.4 |
| No | 83 | 13.6 | |
| Source of information ( | TV | 246 | 46.8 |
| Public health institution | 317 | 60.3 | |
| Private health institution | 61 | 11.6 | |
| Peer | 213 | 40.5 | |
| Other* | 18 | 3.4 | |
| Type of contraceptive that have information about ( | Oral contraceptive | 397 | 75.5 |
| Injectable | 392 | 74.5 | |
| Implanon | 308 | 58.6 | |
| Traditional | 22 | 4.2 | |
| IUCD | 81 | 15.4 | |
| Condom & other barrier meth | 21 | 4 | |
| History of contraceptive use ( | Yes | 398 | 65.4 |
| No | 211 | 34.6 | |
| Type of Contraceptive used ( | Pills | 160 | 40.1 |
| Injectable | 181 | 45.5 | |
| Implanon | 92 | 23.1 | |
| Other** | 21 | 5.2 | |
| Reasons for not using contraceptives ( | Insufficient knowledge | 33 | 15.6 |
| Fear of side effects | 13 | 6.2 | |
| Cultural or religious | 29 | 13.7 | |
| Being student | 11 | 5.2 | |
| Being not married | 33 | 15.6 | |
| Desire to have a child (recently married) | 39 | 18.5 | |
| Start sex near time | 25 | 11.8 | |
| Not anticipating pregnancy | 12 | 5.7 | |
| Other*** | 16 | 7.6 | |
| Variable | Categories | Number | Percentage (%) |
|---|---|---|---|
| Type of institution ( | Public | 367 | 60.3 |
| NGO | 242 | 39.7 | |
| Types of uterine evacuation performed ( | Medical Abortion | 393 | 64.5 |
| MVA/EMA(surgical) | 195 | 32.0 | |
| Both | 21 | 3.4 | |
| Profession of service providers ( | Doctor | 113 | 18.6 |
| Health officer | 53 | 8.7 | |
| Midwifery | 262 | 43.0 | |
| Nurse | 181 | 29.7 | |
| Planning for pregnancy within the next two years ( | Yes | 196 | 32.2 |
| No | 413 | 67.8 |
| Attitude related items | Strongly disagree | Disagree | Neutral | Agree | Strongly agree |
|---|---|---|---|---|---|
| I don't believe that birth control will have negative side effects. | 36 | 186 | 131 | 218 | 38 |
| I believe that birth control will be more beneficial than harmful for me. | 14 | 78 | 89 | 342 | 86 |
| I believe I might get pregnant if I don't use birth control correctly. | 17 | 27 | 94 | 346 | 125 |
| I would feel upset if I became pregnant in the next year. | 74 | 91 | 58 | 192 | 194 |
| It is important is to use birth control when there is no often sex. | 55 | 144 | 166 | 189 | 55 |
| Items of subjective (perceived) norm | Possible answers | ||||
|---|---|---|---|---|---|
| Strongly disagree | Disagree | Neutral | Agree | Strongly agree | |
| My husband or boyfriend support me in using birth control | 40 | 124 | 105 | 287 | 53 |
| Health professionals support me in using birth control | 14 | 21 | 91 | 378 | 105 |
| My family support me in using birth Control | 66 | 178 | 139 | 189 | 37 |
| My friends support me in using birth Control | 32 | 112 | 172 | 247 | 46 |
| I do not want to do as all what my boyfriend husband thinks I should do | 29 | 160 | 92 | 295 | 33 |
| I do not want to do as all what Health professionals thinks I should do | 19 | 150 | 105 | 295 | 40 |
| I do not want to do as all what my family thinks I should do | 30 | 195 | 108 | 249 | 27 |
| I do not want to do as all what my friends thinks I should do | 29 | 141 | 145 | 258 | 36 |
| Health professionals use Contraceptives | 11 | 19 | 199 | 280 | 100 |
| My friends use contraceptives | 19 | 67 | 150 | 303 | 70 |
| My family use contraceptives | 57 | 94 | 129 | 286 | 43 |
| Items of perceived behavioral control | Strongly disagree | Disagree | Neutral | Agree | Strongly agree |
|---|---|---|---|---|---|
| I'm certain I'll use birth control for the next year. | 73 | 77 | 67 | 283 | 109 |
| I'm confident that I'll be proactive about using birth control. | 50 | 88 | 99 | 267 | 105 |
| I'll find it easy to use birth control correctly. | 24 | 90 | 117 | 297 | 81 |
| I'm sure I could stand firm with my husband or boyfriend if he doesn't want me to use contraception. | 34 | 103 | 135 | 264 | 73 |
| It's really important for me to prevent pregnancy at this time. | 71 | 89 | 53 | 237 | 159 |
| I want to accomplish things like finishing school, getting a job, and earning more money before having a child or my next child. | 75 | 86 | 70 | 219 | 159 |
| Variables | Intended (%) | Not intended (%) | COR | 95% CI for COR | AOR | 95% CI for AOR | |
|---|---|---|---|---|---|---|---|
| Marital status | Single | 228 (90.1) | 25 (9.9) | 1.00 | 1 | ||
| Married | 200 (62.3) | 121 (37.7) | 0.181 | (0.113–0.290) | 0.318 | (0.100–1.017) | |
| Divorced | 27 (77.1) | 8 (22.9) | 0.370 | (0.152–0.902) |
|
| |
| Level of education | No formal | 49 (55.1) | 40 (44.1) | 1.00 | 1 | ||
| Primary (1–8) | 77 (62.6) | 46 (37.4) | 1.366 | (0.785–2.380) | 0.959 | (0.400–2.301) | |
| Secondary(9–10) | 152 (84) | 29 (16) | 4.279 | (2.404–7.614) | 0.915 | (0.340–2.464) | |
| Collage | 177 (81.9) | 39 (18.1) | 3.705 | (2.153–6.375) | 0.688 | (0.232–2.047) | |
| Residence | Rural | 69 (53.1) | 61 (46.9) | 1.00 | 1 | ||
| Urban | 386 (80.6) | 93 (19.4) | 3.669 | (2.430–5.541) | 1.255 | (0.596–2.641) | |
| Occupation | Housewife | 116 (59.8) | 78 (40.2) | 1.00 | 1 | ||
| Governmental | 68 (74.7) | 23 (25.3) | 1.988 | (1.143–3.456) | 1.456 | (0.538–3.937) | |
| Private | 91 (77.8) | 26 (22.2) | 2.353 | (1.397–3.966) | 0.642 | (0.278–1.485) | |
| Student | 162 (88) | 22 (12) | 4.951 | (2.915–8.410) | 0.696 | (0.213–2.268) | |
| Other | 18 (78.3) | 5 (21.7) | 2.421 | (0.863–6.791) | 0.437 | (0.069–2.753) | |
| Number of children | No child | 246 (79.6) | 63 (20.4) | 1.00 | 1 | ||
| 1–2 | 113 (69.3) | 50 (70.7) | 0.579 | (0.375–0.892) | 1.729 | (0.698–4.316) | |
| ≥3 | 96 (70.1) | 41 (29.9) | 0.6 | (0.379–0.949) | 1.971 | (0.742–5.236) | |
| Information about contraception | Yes | 416 (79.1) | 110 (20.9) | 4.267 | (2.641–6.892) | 0.890 | (0.365–2.170) |
| No | 39 (47.0) | 44 (53.0) | 1.00 | 1 | |||
| Contraceptives use history | Yes | 335 (84.2) | 63 (15.8) | 4.032 | (2.749–5.914) |
|
|
| No | 120 (56.9) | 91 (43.1) | 1.00 | 1 | |||
| Type of institution | Public | 249 (67.8) | 118 (32.2) | 1.00 | 1 | ||
| NGO | 206 (85.1) | 36 (14.9) | 2.712 | (1.788–4.112) | 1.3,334 | (0.587–3.029) | |
| Desire for pregnancy | Unwanted | 318 (89.1) | 39 (10.1) | 1.00 | 1 | ||
| Wanted | 93 (47) | 105 (53) | 0.109 | (0.70–0.168) |
|
| |
| Mistimed | 44 (81.5) | 10 (18.5) | 0.540 | (0.252–1.157) | 0.728 | (0.264–2.006) | |
| Profession | Doctor | 57 (50.4) | 56 (49.6) | 1.00 | 1 | ||
| Health officer | 46 (86.8) | 7 (13.2) | 6.456 | (2.687–15.51) | 0.575 | (0.163–2.026) | |
| Midwife | 208 (79.4) | 54 (20.6) | 3.784 | (2.353–6.085) | 1.163 | (0.575–2.355) | |
| Nurse | 144 (79.6) | 37 (20.4) | 3.824 | (2.282–6.407) | 0.882 | (0.328–2.372) | |
| Plan for pregnancy For the next 2 years | Yes | 89 (45.4) | 107 (54.6) | 1.00 | 1 | ||
| No | 366 (88.4) | 47 (11.4) | 9.362 | (6.189–14.16) |
|
| |
| Attitude | Positive | 294 (91) | 29 (9) | 7.871 | (5.032–12.31) |
|
|
| Negative | 161 (56.3) | 125 (43.7) | 1.00 | 1 | |||
| Subjective norm | High level | 280 (90) | 31 (10) | 6.348 | (4.102–9.826) |
|
|
| Low level | 175 (58.7) | 123 (41.3) | 1.00 | 1 | |||
| Perceived behavioral control | High level | 324 (94.2) | 20 (5.8) | 16.57 | (9.933–27.65) |
|
|
| Low level | 131(49.4) | 134(50.8) | 1.00 | 1 | |||
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsReproductive Health and Contraception · Global Maternal and Child Health · Adolescent Sexual and Reproductive Health
Introduction
Every year, approximately 121 million women worldwide experience unintended pregnancies, and around 73.3 million of them undergo abortions (1). The use of less effective contraceptive methods, inconsistent or infrequent usage, and discontinuation of contraceptives significantly contribute to unintended pregnancies, which are a primary cause of abortion (2). The World Health Organization (WHO) guidelines recommend that a woman should wait at least six months after an abortion before attempting to conceive again (3). Shorter intervals of less than six months between a miscarriage or induced abortion and a subsequent pregnancy are associated with an increased risk of adverse maternal and perinatal outcomes (4, 5).
The intention to use post-abortion contraceptive methods is a critical aspect of reproductive health, particularly for women who have undergone abortion procedures (6). A woman's specific beliefs about contraceptives influence her engagement and adherence to these methods (7). The Theory of Planned Behavior (TPB) is an effective predictor of intention and behavior. It helps us understand why people make certain decisions, particularly in health-related contexts. According to TPB, our intentions are shaped by how we feel, what others think, and how much control we perceive over the situation (8). The theory comprises attitude, subjective norm, and perceived behavioral control. It suggests that that if a person has a strong intention to engage in a behavior, they are more likely to perform it (9).
The Ethiopian Ministry of Health has made significant progress in expanding comprehensive abortion care. This effort includes the development and dissemination of national guidelines for the provision of legal and safe abortion services, established in 2006 in accordance with World Health Organization standards (10). Furthermore, the ministry has supported the expansion of services provided by the private sector and has integrated safe abortion and post-abortion contraception into existing reproductive health services.
Despite these efforts, the annual abortion rate in Ethiopia increased from 22 per 1,000 women in 2008 to 24 per 1,000 women in 2019 among those aged 15–49. The rate is notably higher in certain areas, with Addis Ababa reporting 49 per 1,000 and the towns of Harar and Dire Dawa reporting 184 per 1,000 women, significantly surpassing other regions (8). A systematic review by Kumsa H et al. found that the pooled prevalence of pregnancy termination in Ethiopia was 21.52% (95% CI: 15.01%–28.03%).
As far as the investigator is aware, some studies in Ethiopia have been conducted from the perspective of intention regarding contraceptive use (11, 12). However, these studies did not incorporate the Theory of Planned Behavior, thus leaving out important factors that are necessary for measuring intention-driven behavior, which plays a vital role in understanding planned actions. In addition, research indicates that there is low contraceptive utilization and a high prevalence of abortion in the study area. Therefore, this study aims to identify various factors that encourage women to consider contraceptive methods, as well as those that may hinder their intentions.
Methodology
Study design, setting and period
A facility-based cross-sectional study was conducted from March 1 to April 6, 2022, in the Harar region and the Dire Dawa city administration health facilities. Harar is one of the cities in eastern Ethiopia, situated approximately 500 kilometers from the national capital, Addis Ababa, at an elevation of 1,885 meters. According to 2013 population projection Harari region has an estimated total population of 226,000 consisting of 114,000 male and 112,000 females. 44.7% of the population is estimated to be rural inhabitants, while 55.3% are urban dwellers.The city is has two public hospitals, eight health centers, and 27 health posts. Additionally, there are two private hospitals and a non-profit family guidance health institution.
Dire Dawa city administration is situated approximately 515 kilometers from the national capital, Addis Ababa, at an elevation of 1,275 meters. According to the 2013 population projection, the Dire Dawa city administration had an estimated total population of 427,000, with 214,000 males and 213,000 females. Of the total population, approximately 37.1% were rural residents, while 62.9% lived in urban areas. The city is home to two public hospitals, 15 health centers, and 34 health posts. Also, there are eight non-governmental health institutions.
Sample size determination and sampling technique
The sample size for both objectives was determined using single and double population proportion formulas, with the larger sample size selected for this study. For the first objective, the sample size was calculated using the single population proportion formula, which considered a 73.5% prevalence of the intention to use post-abortion contraceptives based on a study conducted in Gondor, Ethiopia (12). A 95% confidence level and a 5% margin of error (d) were applied, resulting in a calculated sample size of 299.
The sample size for the second specific objective was determined by considering factors significantly associated with the outcome variable, a two-sided confidence level of 95%, a margin of error of 5%, a power of 80%, and a ratio of exposed to unexposed of 1:1, using STATCALC from Epi Info Version 7. Based on these assumptions, the final sample size was 618 after accounting for a 10% non-response rate.
The study purposefully included a range of health facilities in both Harar and Dire Dawa based on patient flow. These facilities consisted of governmental hospitals, NGO health centers, and public health institutions to ensure a comprehensive representation of abortion care services. Reports from the regional health bureaus of Dire Dawa and Harar were used to estimate the number of women seeking abortion care over one month and one week, with a total of 623 women projected to visit the selected facilities during that time.
To determine these estimates, a term report was obtained from each regional health bureau and divided by three to calculate the average number of women accessing abortion care in one month. This monthly estimate was further divided by four to approximate the weekly patient flow. The estimated numbers varied across facilities, but collectively 623 women were expected to receive abortion services over the study period. All women visiting the selected health facilities for abortion care were interviewed until the target sample size was achieved.
Study population and eligibility criteria
All women who came to selected health facilities for abortion service during the study period constituted the study population. Women who visited these facilities for abortion service during the study period were included in the study, while those in critical condition were excluded.
Data collection tools and procedure
Data were collected using a structured, pre-tested, interviewer-administered questionnaire developed through a review of various literature. After receiving three days of training on the study's purpose, ethical considerations, and data collection techniques, ten BSc midwives conducted face-to-face interviews to collect the data.
Operational definitions
Abortion- defined as termination of a pregnancy before 28 weeks of gestation (13).
Positive Attitudes—when participants summed scored value equal or greater than the median value of summed score 5 attitude related questions (14).
Induced abortion—defined as an abortion that occurs with any medical or surgical intervention (13).
Intended to use contraceptive- those participants who answered yes for post abortion contraceptive intention item (14).
High level of Perceived behavioral control—When participants’ summed score values were equal to or greater than the median value of the summed scores from six perceived behavioral control-related questions (14).
High level of Subjective norm—When participants’ summed scores were equal to or greater than the median value of the summed scores from 11 subjective norm-related questions (14).
Spontaneous abortion—defined as an abortion occurring without any medical or surgical means to empty uterus (13).
Unintended pregnancy is a pregnancy that is either mistimed (occurred earlier than desired) or unwanted (occurred when no children or no more children were desired) at the time of conception (15).
Data processing and analysis
The data were coded, entered, and cleaned using Epi-Data version 3.1 software, and were subsequently exported to SPSS version 20 for analysis. First, descriptive analysis was conducted for each subgroup, followed by the calculation of summed scores for three constructs: attitude, perceived norm (subjective norm), and perceived behavioral control. The median value for each summed score was determined for the three components. The attitude variable was categorized into positive and negative attitudes. A woman who scored a median value of 18 or above was classified as having a positive attitude. The subjective (perceived) norm and perceived behavioral control variables were categorized as low level and high level. Within the subjective (perceived) norm subdivision, there were eleven questions; thus, a woman who scored a median value of 38 or above was classified as having a high level of subjective (perceived) norm. Women who scored a median value of 22 or above out of six perceived behavioral control-related items were classified as having a high level of perceived behavioral control. Finally, for the outcome variable (intention), women who answered “yes” to the intention-related question were assigned a code of “1” (indicating they intended to use it), while those who answered “no” were assigned a code of “0” (indicating they did not intend to use it). Univariate analysis, including simple frequencies, measures of central tendency, and measures of variability, was employed to describe the characteristics of the participants.
Bivariate analysis, including crude odds ratios with 95% confidence intervals, was employed to examine the association between each independent variable and the outcome variable using binary logistic regression. Multi-collinearity was assessed using the Variance Inflation Factor (VIF) and tolerance tests. All variables that yielded a p-value of less than 0.25 in the bivariate analysis were considered candidates for multivariable logistic regression analysis. Associations with p < 0.05 in the multivariable logistic regression were declared as statistically significant.
Ethical consideration
Ethical clearance was obtained from the Haramaya University College of Health and Medical Sciences Institutional Health Research Ethical Review Committee (IHRERC). The study's purpose, procedures, duration, potential risks, and benefits were clearly explained to the participants in the local language. Subsequently, individual informed, voluntary, written, and signed consent was obtained. We assured respondents that their information would remain confidential by not asking for their names during data collection. They were also informed that they could choose not to participate or stop at any time if they felt uncomfortable.
Result
Socio-demographic characteristics
In this study, a total of 609 women participated, resulting in a response rate of 98.5% from the sampled 618. Nine participants were excluded due to incomplete data. The mean age of the women was 25.09 years (±5.17 SD). One-third of the women, totaling 203 (33.3%), fell within the age group of 20–24 years. Half of the women, 321 (52.7%), were married. Among the married women, 50.5% had been married for five years or less. Nearly half of the participants, 277 (45.5%), identified as Muslim. Regarding educational attainment, 216 (35.5%) had completed preparatory education or higher. Two hundred sixty-three women (43.2%) belonged to the Oromo ethnicity, and the majority, 479 (78.7%), resided in urban areas. Approximately one-third of the participants were housewives (Table 1).
Past obstetrics and contraceptive history
Half of the participants, 309 (50.7%), had no children. The majority of the women, 506 (83.1%), reported no previous history of abortion. Most of the women, 526 (86.4%), had received some form of general information about contraceptives before the study. Among these, approximately 400 (65.7%) women had more detailed knowledge about specific contraceptive methods, with 397 (75.5%) aware of pills and 392 (74.5%) familiar with injectable methods. Regarding contraceptive use history, more than half of the respondents, 398 (65.4%), had previously used contraceptives, with injectable being the most commonly used method at 181 (45.5%). About one-third of the women had no history of contraceptive use, and the most common reason for not using contraceptives was the desire to have children, reported by 39 (18.6%) of the participants (Table 2).
Present obstetrics and service care history
More than half of the respondents, 367 (60.3%), were from public health facillities. Regarding their pregnancy desires, 357 (58.6%) reported that their pregnancies were unplanned. Three hundred ninety-three (64.5%) of uterine evacuations were performed through medical termination. Approximately half, 262 (43.0%), of pregnancy terminations were conducted by midwifery professionals. Out of the respondents, 413 (67.8%) indicated that they have no pregnancy plans within the next two years (Table 3).
Attitude, subjective (perceived) norm and perceived behavioral control towards contraceptive
Attitude, subjective norm, and perceived behavioral control were measured using the components of the Theory of Planned Behavior. The median scores for each summed score were calculated, resulting in median scores of 18 for attitude, 38 for subjective (perceived) norm, and 22 for perceived behavioral control, respectively. More than half of the women, 323 (53%), scored at or above the median, indicating a positive attitude toward contraception. Among these respondents, 311 (51.1%) exhibited a high level of subjective (perceived) norm, while 287 (47.1%) demonstrated a high level of perceived behavioral control (Tables 4–6; Figure 1).
Attitude, level of subjective (perceived) norm and level of perceived behavioural control of women came for abortion service (n = 609) in health facilities of Harari region and Dire Dawa city administration, eastern Ethiopia.
Intention towards contraceptive
More than two-thirds of the participants, 455 (74.7%), reported an intention to use post-abortion contraception (95% CI: 71.3–78.2). Among those with this intention, 255 women (41.9%) planned to use Implanon. Conversely, 154 women (25.3%) expressed no intention to use contraceptives after their abortion; of these, 89 women (57.8%) indicated that they did not intend to engage in family planning because they desired to have children.
Factors affecting intention to use post abortion contraceptive
In the bivariable model, intention to use post abortion contraceptive was significantly associated with marital status, duration of marriage, level of education, residence, occupation, number of child, information about contraceptive, contraceptive use history, type of healthcare institutions, desire for pregnancy, Clinical service provider profession, plan for pregnancy within the next two years, attitude towards contraceptive, subjective (perceived) norm and perceived behavioral control.
Out of those associated variables in bivariable analysis; marital status, contraceptive use history, desire for pregnancy, plan for pregnancy within the next two years, attitude, subjective (perceived) norm and perceived behavioural control were maintain their significant association with intention towards post abortion contraceptive use in multivariable analysis.
Divorced women had an 85% lower likelihood of intending to use post-abortion contraception compared to single women [Adjusted Odds Ratio (AOR) 0.149; 95% Confidence Interval (CI) (0.039–0.578)]. Women with a history of contraceptive use were 2.6 times more likely to intend to use post-abortion contraception than those without such a history [AOR 2.580; 95% CI (1.216–5.473)]. Women who had abortions for unplanned pregnancies were 66% less likely to intend to use post-abortion contraception [AOR 0.336; 95% CI (0.153–0.735)] compared to those who had abortions for unwanted pregnancies. Women who did not plan for pregnancy within the next two years had increased odds of intending to use post-abortion contraception [AOR 2.859; 95% CI (1.451–5.635)] compared to those who had a plan. Women with a positive attitude towards contraception were three times more likely to intend to use post-abortion contraception [AOR 3.335; 95% CI (1.831–6.077)], while those with a high level of subjective (perceived) norms were also three times more likely to intend to use it [AOR 3.348; 95% CI (1.805–6.210)]. Additionally, women with a high level of perceived behavioral control were six times more likely to intend to use post-abortion contraception [AOR 6.784; 95% CI (3.650–12.607)] compared to those with negative attitudes, low levels of subjective norms, and low levels of perceived behavioral control, respectively (Table 7).
Discussion
This study examined the association between various factors affecting women's intention to use post-abortion contraceptives in Eastern Ethiopia. The overall intention to use post-abortion contraceptives was found to be 74.7% (95% CI: 71.3–78.2). This finding aligns with results from studies conducted in Gambela (74.4%), and Gondar (73.5%) in Ethiopia (11, 12). However, it is slightly higher than the findings from studies in China (42.5%) (14, 16). The differences may be attributed to variations in the socio-demographic characteristics of the respondents; a majority of participants in this research had a history of contraceptive use, and this study focused on general contraceptive intention, whereas the study conducted in China specifically examined intentions toward long-acting contraceptives. Conversely, the intention rate was lower than that reported in studies from Nepal (83%), India (100%), Tanzania (89%), and Addis Ababa (90.6%) (17–19). These discrepancies may be due to variations in sample sizes and the predominance of respondents from urban regions in the in the aforementioned studies. Urban populations might have better access to healthcare services, education, and information about family planning, which could influence their intention rates.
Divorced women exhibited an 85% lower likelihood of intending to use contraceptives after an abortion compared to single women [AOR 0.149; 95% CI (0.039–0.578)]. This finding aligns with studies conducted in Gambela and Gondar, Ethiopia (11, 12). This may be attributed to the belief among many divorced women that they will not engage in sexual intercourse again, leading to a decreased concern about unwanted pregnancies (20).
Similarly to the study conducted in Nepal (14), women with a history of contraceptive use were more likely to intend to use contraceptives post-abortion compared to those without such a history [AOR 2.580; 95%CI (1.216–5.473)]. This may be attributed to the fact that individuals with prior experience are more familiar with contraceptive methods, which can increase their perceived need and likelihood of future use (21).
Women whose pregnancies were wanted but ended in abortion were less likely to use post-abortion contraceptives [AOR 0.336; 95% CI (0.153–0.735)] compared to women whose pregnancies were unwanted. Similarly, studies conducted in Gondar and Addis Ababa, Ethiopia, found that women with unwanted pregnancies were more likely to adopt contraceptives after abortion than those with wanted pregnancies (11, 13). This may be because women who desire a pregnancy typically plan to have a child. Therefore, they may seek to regain their fertility as quickly as possible in order to conceive again.
Women who did not have a pregnancy plan for the next two years were 2.9 times more likely to intend to use post-abortion contraceptives [AOR 2.859; 95% CI (1.451–5.635)]. This study aligns with research conducted in Adigrat, Ethiopia, and China (16, 22). This may be attributed to their increased awareness of the potential risks associated with unplanned pregnancies (23).
The Theory of Planned Behavior (TPB) defines attitude as the degree to which someone feels positively or negatively about doing a specific behavior. In this study, women who held a positive attitude toward contraception were 3.3 times more likely to intend to use post-abortion contraceptives compared to those who exhibited a negative attitude [AOR 3.335;95% CI (1.831–6.077)]. Similar findings have been reported in research from Nepal (14). This may be because if someone has a positive attitude towards a particular behavior, they are more likely to possess strong internal motivation to engage in that behavior. Positive attitudes often lead to stronger intentions to perform a behavior, as outlined by the TPB.
Inline to the findings of a study conducted in Nepal (14), the present study demonstrated that women with high levels of subjective (perceived) norms were 3.348 times more likely to intend to use post-abortion contraceptives than those with low levels of subjective norms. This indicates that when women feel supported by their social circles or experience less fear of judgment, they are more likely to consider using contraceptives. These results align with the Theory of Planned Behavior, which emphasizes the influence of social expectations on shaping intentions and behaviors (24, 25).
This study found that women with higher perceived behavioral control had stronger intentions to use post-abortion contraceptives compared to their counterparts with lower levels of control. A strong sense of perceived behavioral control indicates that women feel more capable of managing the behavior, which in turn boosts their motivation to take action regarding contraception. This aligns with the Theory of Planned Behavior, which highlights the crucial role of feeling capable in influencing intentions (24, 25).
Conclusion
The findings indicate that there is relatively good magnitude of intention towards contraceptive after abortion as compared to other study. Marital status, contraceptive use history, desire for pregnancy, plan for pregnancy within the next two years, attitude towards contraceptive, level of subjective norm and level of perceived behavioral control were independent factors of women's intention towards post abortion contraceptive at Harari region and Dire Dawa city administration health institutions. Healthcare providers should offer comprehensive education and counseling on contraceptive options for women following an abortion. Furthermore, it is crucial to provide personalized counseling to address each woman's unique needs and concerns regarding contraceptive choices.
Strength and limitation of the study
This study aimed to explore behavioral components that serve as strong predictors of intention and behavior. Additionally, it introduced a new variable, the duration of marriage, which had not been included in previous studies conducted in Ethiopia. One limitation of the study was the presence of social desirability bias. To mitigate this bias, data collectors interviewed the women privately in a separate room.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Bearak J Popinchalk A Ganatra B Moller A-B TunçalpÖBeavin C Unintended pregnancy and abortion by income, region, and the legal status of abortion: estimates from a comprehensive model for 1990–2019. Lancet Glob Health. (2020) 8(9):e 1152–e 61. 10.1016/S 2214-109X(20)30315-632710833 · doi ↗ · pubmed ↗
- 2Bellizzi S Mannava P Nagai M Sobel HL. Reasons for discontinuation of contraception among women with a current unintended pregnancy in 36 low and middle-income countries. Contraception. (2020) 101(1):26–33. 10.1016/j.contraception.2019.09.00631655068 · doi ↗ · pubmed ↗
- 3World Health Organization. Clinical Practice Handbook for Quality Abortion Care. Geneva: World Health Organization (2023).
- 4Kangatharan C Labram S Bhattacharya S. Interpregnancy interval following miscarriage and adverse pregnancy outcomes: systematic review and meta-analysis. Hum Reprod Update. (2017) 23(2):221–31. 10.1093/humupd/dmw 04327864302 · doi ↗ · pubmed ↗
- 5Tessema GAHåberg SE Pereira G Magnus MC. The role of intervening pregnancy loss in the association between interpregnancy interval and adverse pregnancy outcomes. BJOG. (2022) 129(11):1853–61. 10.1111/1471-0528.1722335596254 PMC 9541236 · doi ↗ · pubmed ↗
- 6Baynes C Yegon E Lusiola G Achola J Kahando R. Post-abortion fertility desires, contraceptive uptake and unmet need for family planning: voices of post-abortion care clients in Tanzania. J Biosoc Sci. (2021) 53(6):908–23. 10.1017/S 002193202000060733050954 · doi ↗ · pubmed ↗
- 7Roe AH Mc Allister A Sammel MD Schreiber CA. Pregnancy intentions and contraceptive uptake after miscarriage. Contraception. (2020) 101(6):427–31. 10.1016/j.contraception.2020.03.00232199790 PMC 7430048 · doi ↗ · pubmed ↗
- 8Conner M. Theory of planned behavior. In: Tenenbaum G, Eklund RC, editors. Handbook of Sport Psychology. Hoboken NJ: John Wiley & Sons, Inc. (2020). p. 1–18.