Risk Factors for Acute Hemorrhagic Rectal Ulcers after Bypass Surgery for Chronic Limb-Threatening Ischemia
Yohei Kawai, Masayuki Sugimoto, Takuya Osawa, Changi Lee, Shuta Ikeda, Kiyoaki Niimi, Hiroshi Banno

TL;DR
This study finds that using steroids and being unable to walk after surgery increase the risk of rectal ulcers in patients with severe leg blood flow issues.
Contribution
Identifies steroid use and postoperative nonambulatory status as novel risk factors for acute hemorrhagic rectal ulcers after bypass surgery in CLTI patients.
Findings
6 out of 80 CLTI patients developed AHRU after bypass surgery.
Steroid use and postoperative nonambulatory status were significant risk factors for AHRU.
AHRU patients had longer hospital stays and higher steroid use compared to non-AHRU patients.
Abstract
Objectives: Acute hemorrhagic rectal ulcer (AHRU) occurs with a sudden onset of painless bloody stools and is caused by impaired blood flow in the rectal mucosa due to arteriosclerosis or prolonged bedridden status. Little information is available about AHRU in patients with chronic limb-threatening ischemia (CLTI). This study aimed to identify factors related to AHRU among CLTI patients after bypass surgery. Methods: Between 2019 and 2023, we enrolled 80 CLTI patients at our institution who underwent bypass surgery using autogenous veins. Data were collected prospectively and supplemented with retrospective medical record reviews. Information regarding demographic and clinical characteristics was collected. The outcomes of patients without AHRU (non-AHRU group) and those with AHRU (AHRU group) were compared. Logistic regression analysis was used to assess factors associated with AHRU…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
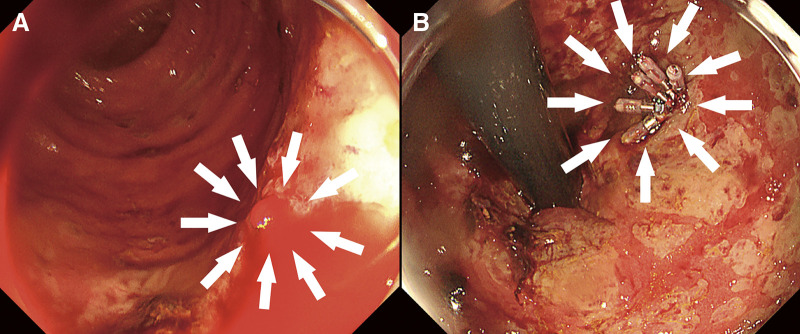 Figure 1
Figure 1| Case | 1 | 2 | 3 | 4 | 5 | 6 |
|---|---|---|---|---|---|---|
| Days to the onset of AHRU after surgery | 7 | 10 | 15 | 26 | 65 | 7 |
| Age | 79 | 66 | 64 | 87 | 73 | 67 |
| Gender | F | M | F | F | F | M |
| DAPT | – | + | – | – | – | – |
| Anticoagulant drugs | – | – | – | + | – | – |
| Steroid (mg/day) | – | – | Prednisolone (10) | Prednisolone (12.5) | – | Hydrocortisone (20) |
| Transfusion (units) | 0 | 4 | 16 | 0 | 8 | 4 |
| Inferior mesenteric artery | Patent | Patent | Patent | Patent | Patent | Patent |
| Internal iliac arteries | Bilateral patent with calcification | Bilateral patent with calcification | Bilateral patent | Bilateral patent with calcification | Bilateral patent with calcification | One-sided patent |
| Endoscopic treatment (clipping) | – | + | + | – | + | + |
| Recurrence | – | + | + | + | – | – |
| Variables | Non-AHRU group (n = 74) | AHRU group (n = 6) | P value |
|---|---|---|---|
| Age (years) | 72.5 [69,77] | 70.0 [66.3,77.5] | 0.763 |
| Female sex | 25 (34) | 4 (67) | 0.182 |
| Nonambulatory status before the onset of CLTI | 2 (3) | 0 (0) | 1.000 |
| Nonambulatory status before surgery | 28 (38) | 4 (67) | 0.211 |
| Body mass index (kg/m2) | 21.2 [19.1,23.5] | 22.2 [19.8,23.3] | 0.695 |
| Hypertension | 58 (78) | 5 (83) | 1.000 |
| CAD | 52 (70) | 3 (50) | 0.370 |
| Dyslipidemia | 37 (50) | 4 (67) | 0.676 |
| CVD | 11 (15) | 1 (17) | 1.000 |
| Hemodialysis | 35 (47) | 3 (50) | 1.000 |
| Diabetes mellitus | 44 (60) | 5 (83) | 0.399 |
| Smoking | 42 (57) | 2 (33) | 0.401 |
| EF (%) | 63 [55,67] | 58 [47,63] | 0.202 |
| Creatinine (mg/dL) | 2.42 [0.73,6.80] | 3.48 [1.32,7.29] | 0.289 |
| Albumin (g/dL) | 3.1 [2.7,3.6] | 2.9 [2.6,3.1] | 0.210 |
| Hemoglobin (g/dL) | 11.0 [9.7,12.6] | 10.3 [10.0,11.2] | 0.499 |
| GNRI | 87.6 [78.1,97.8] | 84.0 [77.5,87.9] | 0.391 |
| Barthel index | 80 [65,90] | 90 [83,98] | 0.214 |
| Medication | |||
| Aspirin | 42 (57) | 4 (67) | 1.000 |
| Clopidogrel | 37 (50) | 1 (17) | 0.676 |
| Cilostazol | 11 (15) | 1 (17) | 1.000 |
| DAPT | 24 (32) | 1 (17) | 0.731 |
| Anticoagulant drugs | 14 (19) | 1 (17) | 1.000 |
| Statin | 35 (47) | 3 (50) | 1.000 |
| Steroid | 5 (7) | 3 (50) | <0.001 |
| Variables | Non-AHRU group (n = 74) | AHRU group (n = 6) | P value |
|---|---|---|---|
| Rutherford classification | 0.283 | ||
| 4 | 8 (11) | 0 (0) | |
| 5 | 40 (54) | 2 (33) | |
| 6 | 26 (35) | 4 (67) | |
| WIfI stage | 0.401 | ||
| 1 | 2 (3) | 0 (0) | |
| 2 | 12 (16) | 0 (0) | |
| 3 | 16 (22) | 0 (0) | |
| 4 | 44 (59) | 6 (100) | |
| Wound grade | 0.184 | ||
| 0 | 11 (15) | 0 (0) | |
| 1 | 26 (35) | 1 (17) | |
| 2 | 20 (27) | 3 (50) | |
| 3 | 17 (23) | 2 (33) | |
| GLASS stage | 0.646 | ||
| I | 15 (20) | 2 (33) | |
| II | 22 (30) | 2 (33) | |
| III | 37 (50) | 2 (33) |
| Variable | Non-AHRU | AHRU group (n = 6) | P value |
|---|---|---|---|
| Distal anastomosis | 0.872 | ||
| Popliteal artery | 22 (30) | 1 (17) | |
| Crural artery | 22 (30) | 3 (50) | |
| Infra-malleolar artery | 30 (40) | 2 (33) | |
| Operation time ≥406 min (median) | 48 (65) | 6 (100) | 0.077 |
| Blood loss (mL) ≥225 mL (median) | 43 (58) | 5 (83) | 0.225 |
| Postoperative nonambulatory status | 1 (1) | 3 (50) | 0.041 |
| Length of hospital stay (days) | 48 [30,83] | 106 [91,133] | 0.004 |
| 30-day mortality | 0 (0) | 0 (0) | N/A |
| In-hospital mortality | 2 (3) | 3 (50) | 0.002 |
| Cause of death | NOMI, AS | NOMI, acute hemorrhagic |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPeripheral Artery Disease Management · Anatomy and Medical Technology · Diagnosis and Treatment of Venous Diseases
Introduction
Acute hemorrhagic rectal ulcer (AHRU) is a condition that presents with painless bleeding from the rectum and often results in a critical outcome. It is more common in elderly people with underlying medical conditions and is considered to be associated with impaired activities of daily living (ADL). Although there have been several reports about AHRU, its risk factors have not been sufficiently investigated due to the small number of cases.^1–19)^
Chronic limb-threatening ischemia (CLTI) is associated with amputation, death, and deterioration in quality of life, and it is a condition requiring revascularization. Bypass surgery using an autologous vein is the standard treatment for CLTI, but it is more invasive than endovascular therapy.^20)^ Some patients who undergo bypass surgery may experience postoperative deterioration in ADL and suffer from AHRU during their hospital stay. However, few reports have shown an association between CLTI and AHRU. The aim of this study is to assess the risk factors for AHRU after bypass surgery for CLTI.
Patients and Methods
Study population
This clinical investigation analyzed the preoperative medical risk factors, surgical characteristics, and outcomes of 80 CLTI patients who underwent bypass surgery at our institution between 2019 and 2023.
Data were collected from a prospectively maintained database. Patient records were carefully reviewed retrospectively. This study was conducted in accordance with the Declaration of Helsinki. The Nagoya University School of Medicine Institutional Review Board approved the study (approval number: 2023-0265). All patients provided written informed consent prior to the intervention and data collection.
Revascularization procedures and postoperative management
In our hospital, arterial revascularization is considered for all CLTI patients. Blood sampling data, cardiac status (electrocardiography, coronary angiography, and echocardiography), respiratory function, and other parameters were routinely assessed. The treatment strategy for each patient was discussed by the vascular surgical team, and the most appropriate treatment was selected on the basis of the patient's comorbidities, ambulatory status, venous status, wound condition, and anatomical features. Surgical bypass tends to be preferred as the first choice, particularly in patients with large tissue loss and lower leg lesions. The technical details of the vein graft bypass procedure have been published previously.^21,22)^ The distal anastomotic site was chosen based on the optimal runoff vessel to the ischemic wounds. Proximal anastomoses were performed with 6-0 polypropylene sutures, and distal anastomoses were performed with 7-0 polypropylene sutures. For distal anastomoses, we used the non-dissection method with pneumatic tourniquets to control blood flow. The greater saphenous vein (GSV) was the preferred conduit if it had a diameter greater than 2 mm, as determined by preoperative duplex scan imaging. If the GSV was unavailable, the lesser saphenous or an arm vein was used. When a single vein was too short, a spliced vein graft was created using 7-0 sutures. The policy is not to perform bypass surgery in patients with infections beyond the ankle joint, severe dementia, or gait failure prior to the onset of CLTI.^21,22)^
Patients taking oral steroids have preoperative steroid coverage, depending on the anesthesiologist's judgment, because their adrenal cortical function is suppressed.
Heparin was intravenously administered for 24 hours, and prostaglandin E1 was also infused for several days postoperatively. All patients subsequently received antiplatelet drugs. Recently, low-dose rivaroxaban has been administered in addition to aspirin in patients with acceptable renal function.
With respect to actual physiotherapy after bypass surgery, early mobilization from the day after surgery is encouraged, with close attention paid to vital signs. In patients with ischemic wounds, gait training is also given as early as possible, with thorough unloading.
Definitions
In this study, we included patients who underwent bypass surgery for CLTI. Coronary artery disease was defined as abnormal coronary angiography and previous myocardial infarction, open coronary artery surgery, or percutaneous coronary revascularization. Cerebrovascular disease was defined as patients who had suffered a stroke in the past or who had carotid artery lesions that had previously undergone carotid artery stenting or carotid endarterectomy. Hypertension, dyslipidemia, and diabetes mellitus were diagnosed in patients receiving relevant active treatment or dietary therapy. A positive smoking history was defined as any prior smoking. Ambulatory status was defined as the patient's functional status immediately before the initial operation. Patients were considered nonambulatory if they were wheelchair-bound or bedridden. AHRU was defined as an ulcerative lesion in the lower rectum within 5 cm of the dentate line, identified by endoscopy, with sudden, painless, fresh bloody stools (Fig. 1).
Fig. 1 Endoscopic findings. (A) Active bleeding was observed from the lower rectum (white arrows). (B) Endoscopic treatment was performed using clips (white arrows).
Clinical endpoints
The goals of this study were to compare patients with and without AHRU after bypass surgery for CLTI and to analyze factors associated with AHRU.
Statistical analysis
Normally distributed continuous variables are expressed as the means ± standard deviations. Medians and interquartile ranges are presented for other continuous variables. Categorical variables are presented as percentages. The JAPAN Critical Limb Ischemia Database (JCLIMB) prediction model was used to calculate the estimated 30-day mortality and major amputation rate, the estimated 2-year survival rate, and the amputation-free survival (AFS) rate.^23,24)^ Statistical significance was calculated and compared between the 2 groups using the χ^2^ test or unpaired t test, as appropriate. Logistic regression analysis was used to assess the associations between each variable and AHRU after bypass surgery. P values <0.05 were considered statistically significant. All statistical analyses were performed using IBM Statistics Statistical Package for Social Science (SPSS) version 29 (IBM Corp., Armonk, NY, USA).
Results
During the study period, 80 CLTI patients underwent bypass surgery. According to the JCLIMB prediction model, the estimated 30-day death and major amputation rate, the estimated 2-year survival rate, and the AFS rate were 3.8% [2.3,6.2], 75% [62,84], and 67% [53,76], respectively. Seventy-four patients did not develop AHRU (92.5%; non-AHRU group), but 6 patients developed AHRU (7.5%; AHRU group). Table 1 summarizes 6 patients with AHRU.
**:
Patient characteristics
The characteristics of the patients in both groups are shown in Table 2. Although the 2 groups were largely similar, the AHRU group had significantly more patients taking oral steroids compared to the non-AHRU group (7% vs. 50%, respectively; P < 0.001). In the non-AHRU group, 5 patients were regularly treated with steroids, 2 for post-renal transplant, 2 for rheumatoid arthritis, and 1 for polymyalgia rheumatica. On the other hand, in the AHRU group, 3 patients were taking steroids for adrenal insufficiency, idiopathic thrombocytopenic purpura, or systemic lupus erythematosus.
**:
Preoperative limb characteristics
Table 3 shows the clinical characteristics of the limbs in both groups. There were no significant differences in the Rutherford classification, wound ischemia and foot infection (WIfI) stage, or global limb anatomic staging system (GLASS) stage between the 2 groups.
**:
Surgical details and short-term outcomes
Table 4 summarizes the details of bypass surgery and the short-term results of both groups. There were significantly more patients in the AHRU group who were unable to walk during the postoperative hospital stay (1% vs. 50%, respectively; P = 0.041). The length of hospital stay was significantly longer in the AHRU group (48 vs. 106 days, respectively; P = 0.004). No mortality within 30 days was observed in either group, but hospital death was significantly more likely to occur in the AHRU group (3% vs. 50%, respectively; P = 0.002). There were 2 deaths during hospitalization in the non-AHRU group, due to nonocclusive mesenteric ischemia (NOMI) and aortic stenosis, and 3 deaths in the AHRU group, due to NOMI, acute hemorrhagic gastric ulcer, and sepsis due to infection of the foot.
**:
Regarding the use of albumin as a nutritional index, in the AHRU group, the preoperative serum albumin level was 2.9 g/dL [2.6,3.1], but it decreased to 2.3 g/dL [2.2,2.6] at the onset of AHRU.
Overall midterm outcomes
The limb salvage rate, survival rate, and AFS rate at 2 years were 89%, 75%, and 67%, respectively.
Risk factors for AHRU after bypass surgery
According to the univariate analysis, factors associated with the development of AHRU were the use of oral steroids (odds ratio [OR], 13.8; 95% confidence interval [CI], 2.19–86.9; P = 0.005) and postoperative nonambulatory status (OR, 7.22; 95% CI, 1.26–41.4; P = 0.026).
Discussion
In this study, we analyzed factors associated with AHRU after bypass surgery for CLTI. We demonstrated that the use of oral steroids and postoperative nonambulatory status were related to the development of AHRU. This study is the first to demonstrate an association between CLTI and AHRU.
AHRU is a condition in which irregular or ring-shaped ulcers are formed in the lower rectum, resulting in sudden painless bleeding, and is considered to occur primarily in elderly patients with underlying diseases such as cerebrovascular disease, coronary artery disease, and diabetes mellitus.^5,8,10)^ In 1974, Delancy and Hitch first reported 3 cases of acute, painless, life-threatening rectal ulcers,^1)^ and in 1981, Soeno et al. described similar cases, and this was the first time that the term AHRU was used.^2)^ Moreover, Duff and Wright reported 7 cases with symptoms similar to AHRU.^3)^ The leading theory regarding the etiology of AHRU is that it is caused by impaired blood flow to the mucosa of the lower rectum due to prolonged bed rest.^25)^ Although there have been several reports on AHRU, few articles have shown an association between CLTI patients and AHRU.^1–19)^
Our analysis revealed that taking oral steroids and postoperative nonambulatory status were significant factors. Nakamura et al. reported that positional changes from the lateral to the supine position reduce blood flow in the lower rectal mucosa, which could induce ischemic ulcerative lesions.^25)^ It is reasonable to expect that CLTI patients, who are at high risk of atherosclerosis, would be susceptible to developing AHRU due to prolonged postoperative supine positioning. In the present study, of the 6 patients who developed AHRU, 3 had a postoperative nonambulatory status until discharge from the hospital. CLTI patients with multiple comorbidities often experience difficulty making progress with rehabilitation due to unstable circulation and respiratory conditions after surgery. Even in such cases, it is very important to encourage patients to change their positions frequently from the supine to the lateral position to avoid complete bedriddenness. Moreover, if patients cannot undergo rehabilitation due to lower limb pain, we should focus on pain management by using appropriate painkillers or performing continuous nerve blocks.
The lower rectum is supplied by the middle rectal artery, which branches off the internal iliac artery. These vessels may be affected by atherosclerosis in patients who develop AHRU. In this study, among the patients who developed AHRU, 1 had only one side patent, and 5 had bilateral patent. Of these 5 patients, 4 had calcification of the internal iliac artery. However, in many cases, contrast computed tomography or angiography is not used to confirm blood flow in the internal iliac artery, and the relationship between internal iliac artery lesions and AHRU remains unknown.
Furthermore, steroids interfere with the healing of ulcers, and delayed healing of rectal ulcers can lead to AHRU.^10)^ In the present study, 3 of the 6 patients who experienced rectal ulcers were regularly treated with steroids for adrenal insufficiency, idiopathic thrombocytopenic purpura, or systemic lupus erythematosus. Further studies are needed to investigate the association between steroids and the postoperative onset of rectal ulceration.
Bleeding complications can occur as a complication of antithrombotic drugs. For the patients in this study, continuous heparin injections, antiplatelet agents, and anticoagulant therapy were also used postoperatively. However, there was no difference in antithrombotic therapy between patients with and without AHRU.
Some reports suggest that hypoalbuminemia is a risk factor for AHRU.^11,13)^ In this study, there was no difference in preoperative serum albumin levels between the 2 groups, but in the 6 patients who developed AHRU, serum albumin levels just before the onset of AHRU were lower than the preoperative values. There is a possibility that a decrease in postoperative serum albumin levels compared with preoperative levels may be associated with the development of AHRU; however, the small number of cases in this study makes it impossible to test this hypothesis, and further studies are needed.
It has been reported that AHRU has a high recurrence rate. However, there is not yet a consensus on the risk factors for recurrence.^18)^ In this study, 3 out of 6 patients of AHRU experienced a recurrence. Although active bleeding and circumferential ulceration are considered to be risk factors for recurrence, the number of cases is too small to allow analysis of these risk factors.^18)^ Patients who developed AHRU needed to be managed on a fasting, and this is thought to have led to the extension of their hospital stay.
The limitations of this study should be mentioned. First, this study was performed retrospectively at a single Japanese vascular surgery center. Therefore, our results might not be free from bias. Second, the number of patients was too small. A larger sample size might be necessary to obtain sufficient statistical power to define the relationship between CLTI and AHRU. Finally, no postoperative physical function other than ambulation was measured in our study. These limitations should be considered in future studies, as they could influence the results.
Conclusions
This study revealed that taking oral steroids and postoperative nonambulatory status were associated with the onset of AHRU after bypass surgery for CLTI. These findings suggest that postoperative rehabilitation is important to prevent the development of AHRU.
Declarations
Disclosure statement
The authors have no conflict of interest to disclose.
Author contributions
Study conception: YKData collection: YKAnalysis: YKInvestigation: YK, MS, HBManuscript preparation: YK, MS, HBCritical review and revision: all authorsFinal approval of the article: all authorsAccountability for all aspects of the work: all authors.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Delancy H, Hitch WS. Solitary rectal ulcer a cause of life-threatening hemorrhage. Surgery 1974; 76: 830–2.4547619 · pubmed ↗
- 2Soeno T, Shoji S, Sakuraba K. Acute hemorrhagic rectal ulcer accompanied with the brain disease. Akita J Med 1981; 8: 207–13. (in Japanese with English abstract)
- 3Duff JH, Wright FF. Acute and chronic benign ulcers of the rectum. Surg Gynecol Obstet 1981; 153: 398–400.6973829 · pubmed ↗
- 4Tseng CA, Chen LT, Tsai KB, et al. Acute hemorrhagic rectal ulcer syndrome: a new clinical entity? Report of 19 cases and review of the literature. Dis Colon Rectum 2004; 47: 895–905.15129312 10.1007/s 10350-004-0531-1PMC 7177015 · doi ↗ · pubmed ↗
- 5Oku T, Maeda M, Ihara H, et al. Clinical and endoscopic features of acute hemorrhagic rectal ulcer. J Gastroenterol 2006; 41: 962–70.17096065 10.1007/s 00535-006-1886-y · doi ↗ · pubmed ↗
- 6Hung HY, Changchien CR, You JF, et al. Massive hematochezia from acute hemorrhagic rectal ulcer in patients with severe comorbid illness: rapid control of bleeding by per anal suturing of bleeder using anoretractor. Dis Colon Rectum 2006; 49: 238–43.16465586 10.1007/s 10350-005-0158-x · doi ↗ · pubmed ↗
- 7Hotta T, Takifuji K, Tonoda S, et al. Risk factors and management for massive bleeding of an acute hemorrhagic rectal ulcer. Am Surg 2009; 75: 66–73.19213400 · pubmed ↗
- 8Motomura Y, Akahoshi K, Matsui N, et al. Clinical and endoscopic characteristics of acute haemorrhagic rectal ulcer, and endoscopic haemostatic treatment: a retrospective study of 95 patients. Colorectal Dis 2010; 12: e 320–5.19863598 10.1111/j.1463-1318.2009.02091.x · doi ↗ · pubmed ↗