Localized Leg Erythema as the Primary Symptom of Scarlet Fever: An Atypical Presentation
Yusuke Ito

TL;DR
A child presented with leg rashes as the main symptom of scarlet fever, highlighting the need for careful diagnosis.
Contribution
Reports an atypical case of scarlet fever presenting with localized leg erythema in a child.
Findings
A seven-year-old boy presented with localized leg rashes as the primary symptom of scarlet fever.
A rapid antigen test confirmed Streptococcus pyogenes infection.
Treatment with cefditoren pivoxil resolved all symptoms.
Abstract
Scarlet fever is an acute infectious condition caused by Streptococcus pyogenes, commonly leading to dermatological complaints in children. Its classical presentation includes fever, sore throat, and diffuse erythematous macules starting on the trunk; however, rare cases may present primarily with skin manifestations. We report a case of a seven-year-old boy who presented with pruritic, localized leg rashes as the primary symptom of scarlet fever. A thorough physical examination revealed painless erythema of the soft palate. Due to a local outbreak of Streptococcus pyogenes infections, a rapid antigen test was performed, yielding a positive result and leading to the diagnosis of scarlet fever. The patient was treated with cefditoren pivoxil, resulting in the complete resolution of symptoms. This case highlights the importance of a thorough patient history, physical examination, and…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
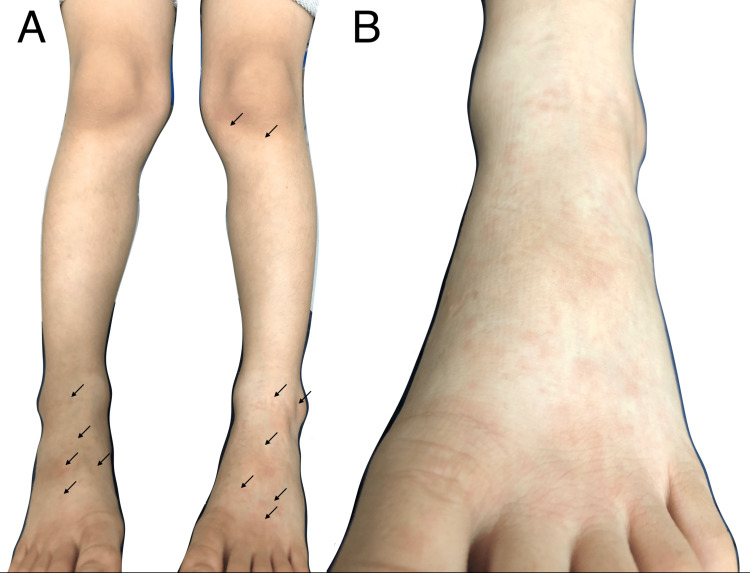 Figure 1
Figure 1| Causes | Differentiating features |
| Measles | During the prodromal phase, fever, the three Cs (cough, coryza, and conjunctivitis), and Koplik spots, followed by a maculopapular erythematous rash starting on the head and neck [ |
| Rubella | Generalized maculopapular erythema, resolving within 72 hours, accompanied by retroauricular, posterior cervical, and posterior occipital lymphadenopathy [ |
| Roseola infantum | Erythematous maculopapular rash appearing after 3-5 days of high fever, starting on the trunk and spreading peripherally [ |
| Pityriasis rosea | A single herald patch (oval-shaped, rose-colored patches with slight scale) on the trunk, followed by smaller similar lesions [ |
| Gianotti-Crosti syndrome | Lichenoid, flesh-colored to red papules on the face, buttocks, and extremities, coalescing to form plaques [ |
| Erythema infectiosum | "Slapped cheek" rash, followed by pink papules and macules in a lacy, reticular pattern on the extremities [ |
| Rocky Mountain spotted fever | Pale red or rose-colored maculopapular rash starting on the wrists and ankles and progressing to petechia [ |
| Scarlet fever | Erythema with sandpaper-like papules after the fever and sore throat, starting on the upper trunk [ |
| Staphylococcal scalded skin syndrome | Generalized macular erythema without mucosal involvement, with perioral and intertriginous erythema becoming vesicular and bullous, rapidly exfoliating within 2 to 3 days [ |
| Tinea corporis | Erythematous annular patch or plaque with a raised, scaly border and central clearing [ |
| Kawasaki disease | Generalized erythema with fever, conjunctivitis, changes in the oropharyngeal mucosa and peripheral extremities, and cervical lymphadenopathy [ |
| Drug-induced exanthema | Maculopapular exanthem after 7-12 days post exposure (common culprits: beta-lactams and non-steroidal anti-inflammatory drugs) [ |
| Erythema multiforme | Target lesions [ |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsStreptococcal Infections and Treatments · Herpesvirus Infections and Treatments · Dermatological and COVID-19 studies
Introduction
Skin complaints are among the most common concerns in pediatric care, accounting for nearly 10% of all visits in primary care ambulatory practice [1]. Scarlet fever, an acute infectious disease caused by exotoxin-producing Streptococcus pyogenes, is one of the most common dermatologic conditions in children, predominantly affecting those between the ages of three and eight years [1,2]. Population rates of scarlet fever were reported as 24-33 cases per 100,000 in regions such as East Asia and England [3]. Its incidence declined during the COVID-19 pandemic but resurged after mitigation measures [4]. The classical presentation includes diffuse erythematous macules starting on the trunk after the onset of fever and sore throat [5,6]. However, in rare cases, patients may present with atypical rash distributions and report only skin symptoms as the primary complaint. We present an atypical case of scarlet fever with erythema limited to the lower extremities as the primary symptom.
Case presentation
A seven-year-old boy presented to our department with leg rashes. On the day of the visit, he complained of mild pruritic rashes on both legs. He reported no prodrome symptoms, including fever and sore throat. Upon presentation, he appeared well and medically stable, with no other symptoms such as sore throat, fever, malaise, or respiratory symptoms. Physical examination revealed no fever on palpation and revealed multiple erythematous macules, measuring 5-10 mm in size, on the front of the left lower leg and bilateral dorsal surfaces of the feet, which blanched on palpation (Figure 1). The soles were spared, with no visible rash in these areas. No other skin abnormalities were observed, including on the face, neck, chest, or upper extremities. A review of systems revealed pharyngeal erythema: painless, pale erythema of the soft palate without petechiae, vesicles, or ulcers. There were no additional findings, such as a red or white strawberry tongue, tonsillitis, or cervical lymphadenopathy.
(A) Multiple blanchable erythematous macules were observed on the bilateral dorsal surfaces of the feet and the front of the left lower leg (arrows). (B) A close-up image of the left foot.
A consultation with pediatrics indicated that the rash characteristics were nonspecific, and initially, a viral-induced exanthema was considered. However, due to the outbreak of Streptococcus pyogenes infections in the surrounding area, it was recommended to rule out streptococcal infection despite the atypical distribution of the rash for scarlet fever. Further history-taking from his parent revealed an outbreak of streptococcal pharyngitis at his daycare center, and the rapid pharyngeal streptococcal antigen test yielded a positive result. There was no history of exposure to other bacterial or viral infections. Based on these findings, and excluding other diseases, a diagnosis of scarlet fever was made. Due to a penicillin shortage, he was treated with cefditoren pivoxil 100 mg twice daily (9 mg/kg/day), leading to an improvement in pruritus and rash. After seven days of treatment, his symptoms resolved completely, and no additional symptoms, including fever, malaise, sore throat, or new rashes, were reported during the treatment period.
Discussion
Scarlet fever is an acute infectious condition caused by exotoxin-producing strains of group A Streptococcus (GAS), also known as Streptococcus pyogenes [2]. Hypersensitivity of the patient to exotoxin is involved in the development of scarlet fever [5]. Scarlet fever occurs in approximately 10% of children with streptococcal pharyngitis [5]. Its classical presentation includes fever and sore throat, followed by a rash appearing 12-48 hours later [5]. This rash is characterized by confluent, erythematous, blanching, fine macules, resembling sunburn and sandpaper-like papules [5,6]. The rash typically starts on the chest and abdomen and gradually extends to the extremities [2,6]. In rare cases, skin symptoms or atypical rash distributions may present as the primary complaint; however, to the best of our knowledge, only one adult case has been reported in case reports [7].
The diagnosis of scarlet fever is primarily clinical, based on characteristic findings and evidence of GAS pharyngitis. The Centor score and rapid antigen tests are commonly used for diagnosing GAS pharyngitis, with cultures ordered if there is a high suspicion of GAS pharyngitis and a negative rapid antigen test result [2,5]. Erythema in children can result from various etiologies, including viral, bacterial, and fungal infections, autoimmune diseases, or drug reactions. We highlighted common and clinically significant differential diagnoses (Table 1) [5,8,9]. Diagnosis requires assessing the rash's morphology and distribution, along with medication history, infection exposure, and a thorough physical examination.
While the typical form of scarlet fever is usually easy to identify, diagnosing atypical cases can be challenging because they resemble other conditions. Fernández Romero et al. reported that 10% of scarlet fever cases presented with a rash only [10]. In this retrospective study, 20 out of 91 scarlet fever patients presented with atypical exanthema, but erythema limited to the distal extremities, as seen in this case, was not included, suggesting that this case represents a rare manifestation. Therefore, even when a rash is the sole symptom, considering scarlet fever in the differential diagnosis is crucial for early diagnosis and treatment to prevent both suppurative complications (e.g., otitis media, peritonsillar abscess, pneumonia, endocarditis, and meningitis) and non-suppurative complications (e.g., rheumatic fever and streptococcal glomerulonephritis) [2,6]. In this case, other conditions presenting with a rash were initially considered, but the patient’s history of exposure and pharyngeal erythema, which was painless and therefore unnoticed even by the patient, provided key diagnostic clues.
Conclusions
It is essential to diagnose scarlet fever early to prevent both suppurative and non-suppurative complications. The classical features of scarlet fever are often incomplete, and patients may present with skin manifestations as the primary symptom. Clinicians should remain vigilant when evaluating erythema, considering not only the skin findings but also the patient's history and a thorough physical examination. Additionally, awareness of local epidemiological data and potential outbreaks is essential for prompt diagnosis and appropriate management.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Dermatologic services provided to children and adolescents by primary care and other physicians in the United States Pediatr Dermatol Krowchuk DP Bradham DD Fleischer AB Jr 199203111994797155210.1111/j.1525-1470.1994.tb 00586.x · doi ↗ · pubmed ↗
- 2Scarlet fever: a guide for general practitioners London J Prim Care (Abingdon) Basetti S Hodgson J Rawson TM Majeed A 77799201710.1080/17571472.2017.1365677 PMC 564931929081840 · doi ↗ · pubmed ↗
- 3Resurgence of scarlet fever in England, 2014-16: a population-based surveillance study Lancet Infect Dis Lamagni T Guy R Chand M 1801871820182919162810.1016/S 1473-3099(17)30693-X · doi ↗ · pubmed ↗
- 4Surveillance of noninvasive group A Streptococcus infections in French ambulatory pediatrics before and during the COVID-19 pandemic: a prospective multicenter study from 2018-2022 Int J Infect Dis Cohen JF Rybak A Werner A 13514113420233729057310.1016/j.ijid.2023.06.003 · doi ↗ · pubmed ↗
- 5Common skin rashes in children Am Fam Physician Allmon A Deane K Martin KL 211216922015 https://www.aafp.org/pubs/afp/issues/2015/0801/p 211.html 26280141 · pubmed ↗
- 6Managing scarlet fever BMJ Drug and Therapeutics Bulletin 0362201810.1136/dtb.2017.8.052928882851 · doi ↗ · pubmed ↗
- 7Atypical presentation of scarlet fever Cureus Alotaibi A Binsaqr MA Mutlaq MR Khojah AA Khojah SA Mohamed HA 014202210.7759/cureus.33142 PMC 988449836721591 · doi ↗ · pubmed ↗
- 8Pediatric exanthems Prim Care Gable EK Liu G Morrell DS 3533692720001081504810.1016/s 0095-4543(05)70200-1 · doi ↗ · pubmed ↗