Divergent psychological stress response patterns to the COVID-19 pandemic in psychiatric patients with vs. without PTSD: A real-world exploratory study
Marit Treptow, Claudia Bartels, Mirjana Ruhleder, Alexander Kratzenberg, Thorgund Reh-Bergen, Mona Abdel-Hamid, Luisa Heß, Jörg Signerski-Krieger, Katrin Radenbach, Björn-Hendrik Schott, Jens Wiltfang, Claus Wolff-Menzler, Ulrike Schmidt, Michael Belz

TL;DR
This study found that psychiatric patients with PTSD experienced higher psychological stress during the pandemic compared to those without PTSD.
Contribution
The study explores pandemic-related stress response patterns in psychiatric patients with PTSD, a previously underconsidered area.
Findings
Psychosocial burden and adjustment disorder symptoms were significantly higher in PTSD patients during the pandemic.
PTSD patients showed no changes in general psychiatric symptoms during the pandemic.
PTSD patients may cope less efficiently with pandemic-related stress compared to those without PTSD.
Abstract
The COVID-19 pandemic has been shown to increase psychological burden and requires efficient coping strategies to maintain mental health. In particular, it remains unclear which pandemic-related stress response pattern occurs in pre-existing posttraumatic stress disorder (PTSD) during the pandemic – at the same time these patients potentially exhibit dysfunctional coping of artificially generated psychosocial stressors. To analyze this so far widely unconsidered pandemic-related stress response in PTSD, this study longitudinally measured psychosocial burden and adjustment disorder (AD) symptom load in 14 patients with a primary or secondary diagnosis of PTSD vs. a cohort of 145 psychiatric patients without PTSD. The previously established Goettingen psychosocial Burden and Symptom Inventory (Goe-BSI) was used. Patients were interviewed at the end of the first (April/May 2020) and the…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
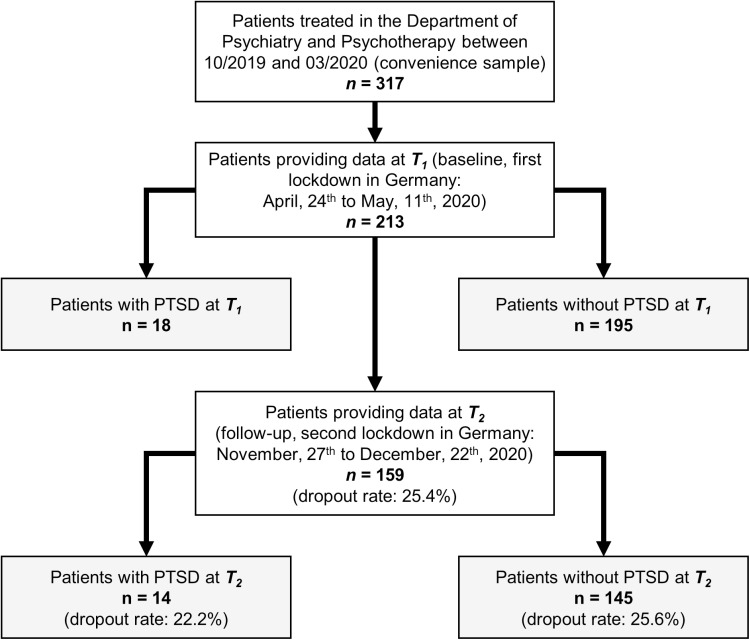 Fig 1
Fig 1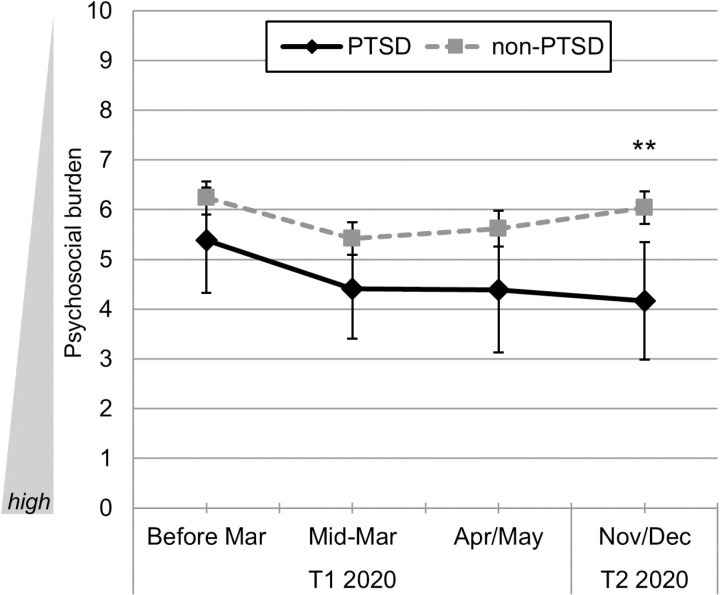 Fig 2
Fig 2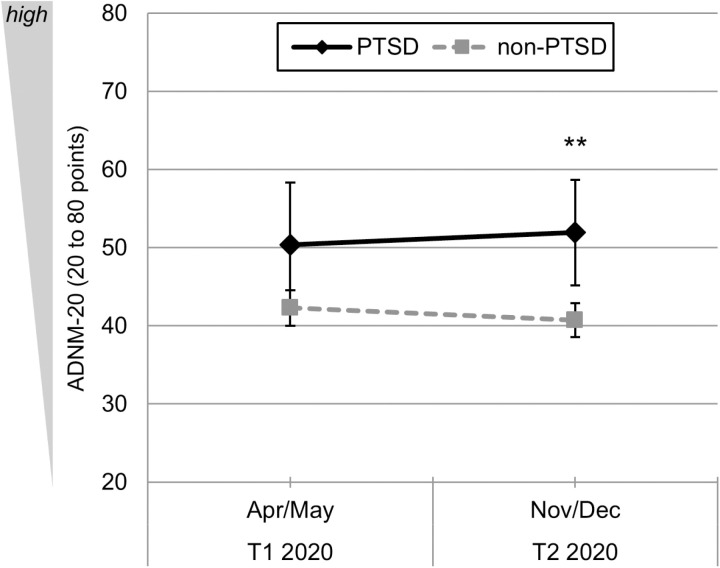 Fig 3
Fig 3- —http://dx.doi.org/10.13039/501100002347Bundesministerium für Bildung und Forschung
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCOVID-19 and Mental Health · Posttraumatic Stress Disorder Research · Long-Term Effects of COVID-19
Introduction
In February 2023, the World Health Organization [1] announced 6.8 million deaths and a rate of 756 million infections caused by the SARS-CoV-2 virus. The pandemic can be considered a strong global stressor due to the global health threat and resulting lockdown restrictions. As such it requires significant adaptation and endangers mental health particularly in those having low resilience.
A pandemic-related increase in first-onset mental illnesses in the general population has been described by several studies in different populations [2–11], including health-care professionals [4,5,12–16] and patients with COVID-19 [17,18]. For the period from March until May 2020 which covered a first lockdown in numerous countries, the COVID-19 pandemic has led to worsening of mental disorders as it is the case for eating disorders [19], bipolar disorder [20] as well as obsessive-compulsive disorder [21]. Moreover, independent from the presence of any psychiatric disorder, the pandemic-related stress response pattern included an increased level of depressive and anxiety symptoms during this early period of the pandemic [22]. Beyond that, the temporal dynamic of the pandemic – e.g., termination of lockdowns, variations of social restrictions – should be considered from a longitudinal perspective. In our previous study we could identify a specific stress response pattern: there, psychosocial burden for different pre-existing mental disorders did not exclusively worsen during the pandemic, but varied over time. We found an increase in psychosocial burden from pre-pandemic until Mid-March 2020, a steady decrease from Mid-March until April/May 2020 and a continued decrease until November/December 2020 [23]. Furthermore, patients with an ICD-10 F4-diagnosis reached the highest scores for all time-points over time compared to patients with other mental disorders.
An exposure-based intervention is the most effective therapy for PTSD [24], which usually could not be continued in presence during the first months of the pandemic due to lockdown restrictions. Many of those patients did not receive any treatment, or could merely be treated via telemedicine (telephone or video contacts). In general, people have experienced a lack of social support during the pandemic with increased feelings of loneliness [25,26]. This social support is a specifically important factor for patients with PTSD to cope with stress-related events [27]. In particular, social support enables for social discrimination learning, proactive coping, healthier behaviors, more positive mood and the release of oxytocin in patients with PTSD [28]. Oxytocin has been shown to increase feelings of security and to reduce the stress response in such patients [29] whereas social isolation, on the other hand, is associated with a negative neurobiological impact [30]. Additionally, symptoms of depression, anxiety, and acute stress which widely increased during the early phase of the pandemic (see above) are also posttraumatic factors with a potential to facilitate the development and/or increase the severity of PTSD [31]. In sum, patients with PTSD seemed specifically vulnerable during the nationwide lockdowns.
Of note we did not find any study specifically analyzing the pandemic-related stress response pattern caused by the impact of the COVID-19 pandemic on distress perception, psychosocial burden and psychiatric symptom load in patients suffering from posttraumatic stress disorder (PTSD). However, some studies could show that patients with pre-existing anxiety disorders (such as PTSD) reached a significantly higher rate of distress caused by self-isolation in comparison to patients with mood disorder and healthy controls [32]. In addition, a low level of social support combined with a high rate of pandemic-related stressors could increase the symptom severity of PTSD [33].
Beyond that, the prevalence of PTSD during or in response to the COVID-19 pandemic has been assessed in various populations. For instance, a meta-analysis reported an increased prevalence of PTSD in the general population (about 24%) after the beginning of the COVID-19 pandemic [3]. Furthermore, a web-based survey revealed a COVID-19-related PTSD prevalence of 29.5% in the Italian population and thus classified the pandemic as a traumatic stressor [34]. Accordingly, a recent study detected that about 75% of COVID-19 survivors in Manipur suffered from PTSD [35].
PTSD is a severe psychiatric syndrome that comprises aversive re-experiencing of trauma-related details, associated avoidance behavior, emotional numbing and nervous hyperarousal [36]. Several studies showed that psychological stress coping is impaired in patients with PTSD compared to healthy controls (e.g., [37,38]), possibly due to alterations in the regulation of the two major stress axes, the hypothalamic-pituitary-adrenal (HPA) axis (e.g., [38]) and the sympathetic nervous system [39]. Of note, PTSD and major depression were found to be predicted by different psychological stress coping styles [40] suggesting that pathological alterations in stress coping might differ among psychiatric disorders.
However, we found no study analyzing whether impaired stress coping in PTSD also occurs in response to enduring real-world stressors such as the COVID-19 pandemic and results in a higher symptom load. This motivated us to compare psychosocial burden and adjustment disorder (AD) symptom load in psychiatric patients with vs. without PTSD during the course of the pandemic using our previously established Goe-BSI inventory and our previously published cohort [23,41]. In this convenience sample, we previously found a specific stress response pattern: during the course of the pandemic, the initial increase in psychosocial burden was relieved while AD symptom load remained unchanged between the first (April, 24^th^ to May, 11^th^ 2020) and the second lockdown (November 27^th^ to December, 22^th^ 2020) in Germany [23]. So far, we concentrated on analyzing the total cohort of patients suffering from various mental disorders and did not focus on specific diagnostic subgroups such as patients with PTSD.
The aim of this study was to focus on patients with pre-existing PTSD and to compare them to a cohort of psychiatric patients with other pre-existing mental disorders, in order to analyze possible differences in the pandemic-related stress response pattern between both groups. To achieve this, psychosocial burden and symptoms of AD were measured at two different time-points during nationwide lockdown periods.
Materials and methods
Please note that further details are given in the legends of Tables 1–3, Figs 1–3.
Table 1: Comparison of general psychiatric symptoms and resilience during the first (T1: Q2/2020) vs. the second lockdown (T2: Q4/2020) in patients with PTSD.
Table 2: Correlations between diagnostic groups, sociodemographic variables and general psychiatric symptoms and resilience (secondary endpoints).
Table 3: Comparison of sociodemographic variables in the PTSD sample vs. the non-PTSD sample at baseline (T1: Q2/2020).
Selection of study patients.
Study sample
For the total sample recruited at baseline (T1: first lockdown, April, 24^th^ to May, 11^th^ 2020 [41], we applied the following inclusion criteria: (1) patients who were ≥ 18 years old, (2) patients who were treated in the Department of Psychiatry and Psychotherapy of the University Medical Center (UMC) Göttingen, Germany between 10/2019 to 03/2020, (3) patients who received no hospitalization at the time-point of inclusion, (4) patients with presence of at least one ICD-10 mental/psychiatric diagnosis (F00-F99) at the time-point of inclusion, (5) patients with capacity for providing informed consent and study data. As we reported previously, of 213 patients at baseline (T1), 159 patients took part in follow-up-measurements (T2; second lockdown, November 27^th^ to December, 22^th^ 2020 [23]; dropout rate of 25.4%). At T1, due to pandemic-related contact restrictions, written informed consent could not be obtained in person but only by mail. Only those patients that had already given consent at T1 were contacted again at T2. In general, informed consent was obtained for study participation and anonymized publication of individual data. In order to comply with the applicable data protection regulations, the data were analyzed in pseudonymized form. First, each study participant was assigned a unique identification number. Subsequently, these identification numbers were converted into consecutive numbers by a person independent of the project. Personal data for re-contacting were stored on a separate list. This list was stored in a location physically accessible only to the study director and his deputy. Beyond this, the authors did not have access to any information that could identify individual participants.
Study design
After ethical approval by the Ethics Committee of the UMC Goettingen (#36/4/20), all interviews were performed by phone in German language and were conducted at two time-points during the COVID-19 pandemic in Lower Saxony, Germany, i.e., at T1 (April, 24^th^ to May, 11^th^ 2020) and T2 (November 27^th^ to December, 22^th^ 2020; see Fig 1 for details). Interviews were performed by 28 qualified and specialized clinicians (psychologists/psychotherapists and psychiatrists) who all received a rater training before the start of assessments. ICD-10 diagnoses of included patients were established during clinical routine by their treating clinicians (residents, board-certified psychiatrists, psychologists, or licensed psychotherapists). For the analyses presented here, we extracted a PTSD subsample from our cohort: in case PTSD (ICD-10: F43.1) was diagnosed as primary or secondary diagnosis, patients were assigned to the PTSD sample while all remaining cases constitute the non-PTSD sample (please see results section for details). All patients with suspected PTSD were diagnosed with trauma-specific instruments (interviews and questionnaires) using the Essen Trauma-Inventory (ETI) [42] and the Impact of Event Scale - Revised (IES-R) [43].
Study measures
The Goettingen psychosocial Burden and Symptom Inventory (Goe-BSI), a standardized and structured telephone interview, was applied at T1 and T2 – please see our previous publications for detailed information about scale development, quality criteria and further details [23,41]. Besides demographic data, the Goe-BSI allows assessment of the course of general psychiatric symptoms during the pandemic along with resilience. It is, so far, exclusively available in German language. We defined two primary outcome measures to operationalize stress coping in PTSD, namely (1) psychosocial burden and (2) the presence of AD symptoms in response to the pandemic (AD New Module – 20 Item version [ADNM-20] [44]).
Briefly, the assessment of psychosocial burden consisted of three items rated on 11-point numeric scales which were formulated as questions: psychosocial stress, psychiatric symptoms, and quality of life with lower scores indicating higher psychosocial burden (0: It could not be worse; 10: It could not be better). At T1, not only the current state was assessed but also, retrospectively, the states before and at the beginning of the pandemic when maximum pandemic-related restrictions had become active in Germany (first lockdown, mid-March, 2020). This resulted in four ratings per patient (three at T1, one at T2) and allowed to generate a trajectory of psychosocial burden from baseline to follow-up. The ADNM-20 was used at T1 and at T2 (current states only, no retrospective assessments) to measure psychological reactions to stressful life events (here: the pandemic). The ADNM-20 consists of 20 four-point items; 48 out of 80 points are defined as cut-off reflecting a high risk for the presence of an AD [45]. Assessment of psychiatric symptoms (20 items/statements) and resilience (two items/statements) was performed at both, T1 and T2. The spectrum of possible answers ranged from 0 (strongly disagree) to 10 (strongly agree) – please see Table 1 for all translated items).
Statistical analyses
IBM SPSS Statistics, version 29 was employed for data analysis. Frequencies, means (M), standard deviations (±/ SD), and correlations (depending on scale level: Pearson correlations (metric), mean square contingency/phi coefficients (binary) – see Table 2) were computed for descriptive representation of metric variables.
Two general linear models for repeated measurements (GLM) were calculated for the two primary outcomes of this study, i.e., psychosocial burden and symptoms of AD (i.e., ADNM-20 sum score). For psychosocial burden, multiple measurements were added as four-staged within-subjects factor: each participant contributed three measurements at baseline (T1: before the pandemic, at the beginning of the pandemic, at current state during first lockdown), and one measurement at follow-up (T2: current state during second lockdown). A two-staged between-subjects factor was also added (PTSD sample vs. non-PTSD sample). For symptoms of AD (ADNM-20), two repeated measurements were included (T1 and T2: current state during first/second lockdown). Again, allocation to the PTSD sample was added as two-staged between-subjects factor. Besides main effects, the interaction effect (PTSD status × repeated measurement) was tested in each GLM to map possible different trajectories between patients with vs. without PTSD on both primary outcomes. Pairwise comparisons (t-tests) were then used to validate possible interaction effects. Missing data can be derived from degrees of freedom for each model. For multiple comparisons, p-values were corrected within each GLM, using the Bonferroni method (initial significance: p < 0.05, two-tailed).
For explorative analysis of psychiatric symptoms and resilience from T1 to T2, multiple t-tests for dependent measures were used without Bonferroni-correction (please see results section for details, Table 1).
Results
Demographical and clinical characteristics of the study sample
In total, 159 patients treated in the Department of Psychiatry and Psychotherapy of the UMC Goettingen completed the Goe-BSI by interview twice, i.e., both during the first (baseline: April, 24^th^ to May, 11^th^ 2020, T1) and the second (follow-up: November 27^th^ to December, 22^th^ 2020, T2) national lockdown phase. Out of these 159, 14 patients were assigned to the PTSD sample, either due to their main diagnosis (n = 7, 50.0%) or secondary diagnosis (n = 7, 50.0%) which had been determined by the patients’ treating clinicians (see material and methods). The remaining patients, i.e., the non-PTSD sample, consisted of n = 145 patients. The five most frequent main psychiatric ICD-10 diagnoses of this sample were (1) affective disorders (F3, n = 61, 42.1%), (2) disorders of adult personality and behavior (F6, n = 25, 17.2%), (3) schizophrenia, schizotypal and delusional disorders (F2, n = 21, 14.5%), (4) neurotic, stress-related and somatoform disorders (F4, n = 17, 11.7%), and (5) disorders of psychological development (F8, n = 14, 9.7%). The enrichment of the latter can be explained by the fact that our Autism Spectrum Outpatient Unit participated in recruitment of study subjects.
Table 3 shows sociodemographic variables of the PTSD in comparison to the non-PTSD sample. Two variables differed significantly between the PTSD and the non-PTSD sample, namely living space and sum of F-diagnoses: in comparison to psychiatric patients without PTSD, those suffering from this stress-related disorder had smaller living spaces (M = 58.69 m² ± 26.83 vs. M = 95.70 m² ± 54.38, p = .017) and a higher number of F-diagnoses (M = 2.79 ± 1.42 vs. non-PTSD sample: M = 1.74 ± 0.96, p < .001). The latter suggests a comparably higher level of comorbidity in PTSD patients. The number of persons of female gender were elevated in the PTSD sample with a trend for statistical significance (p = .092; PTSD: n = 9 female (64.3%), n = 4 male (28.6%), n = 1 patient of non-binary gender (7.1%) vs. non-PTSD: n = 55 female (44.7%), *n = * 68 male (46.9%), n = 22 of non-binary gender (15.2%)). In the PTSD vs. the non-PTSD sample there were no differences in the mean age (PTSD: M = 39.86 years, SD = 13.42, range: 23 to 70 years; non-PTSD M = 41.25 years, SD = 16.21, range: 18 to 82 years). Half of the patients with PTSD reported that they belonged to a risk group for a severe course of a SARS-CoV-2 infection (n = 7), whereas this was the case in only 33.1% (n = 48) of those without PTSD (ns). Until the time-point of the second lockdown, n = 6 of the PTSD sample (42.9%) vs. n = 45 of the non-PTSD sample (31.3%) had been tested for COVID-19 at least once (no positive results, no quarantine; ns). The majority of patients with and without PTSD reported that during the pandemic no changes had occurred in the following areas: family status, living condition, work situation, financial situation and childcare – there were no significant between-group differences in these parameters.
Course of psychosocial burden
The GLM revealed a significant variation in psychosocial burden over time (total score of the Goe-BSI) for the total sample (F(3, 462) = 3.67, p = .012, partial η^2^ = 0.023): As we found previously [23], psychosocial burden significantly increased from the time-point before the pandemic/lockdown to its beginning, but then decreased during the first and second lockdown in the total cohort. Comparing the PTSD to the non-PTSD subsample, a significant between subjects-effect with a medium effect size was found (F(1, 154) = 8.02, p = .005, partial η^2^ = 0.05): Patients with PTSD showed comparably higher levels of psychosocial burden for the global set of measurement points (Fig 2). Although we did not find a significant interaction effect (F(3, 462) = 1.09, ns), descriptive analysis suggested that patients with PTSD showed an increase of psychosocial burden from the time-point before the pandemic (M = 5.38, SD = 2.02) to its beginning (M = 4.40, SD = 1.92), to the first lockdown (T1: M = 4.38, SD = 2.39) and to the second lockdown (Fig 2, T2: M = 4.17, SD = 2.25). In comparison, descriptive analysis of patients without PTSD also showed an increase of psychosocial burden from the time-point before the pandemic (M = 6.24, SD = 2.01) to its beginning (M = 5.42, SD = 1.98), followed by a decrease of psychosocial burden at the first lockdown (T1: M = 5.62, SD = 2.19), followed by an additional decrease at the second lockdown (Fig 2, T2: M = 6.04, SD = 1.97). While pairwise comparisons were non-significant for the first three time-points after Bonferroni-correction (t between 1.54 and 1.98, ns), we found a significant difference with a large effect size during the second lockdown (Fig 2, current state T2: t(155) = 3.34, p = .004, demp = 0.88) indicating a comparably higher psychosocial burden in the patient group with PTSD at the last time-point. Please see Table 4 for all mean values and differences between both subsamples.
Table 4: Stress response patterns between the PTSD sample and the non-PTSD sample (T1: Q2/2020, T2: Q4/2020).
Course of psychosocial burden during different phases of the Covid-19 pandemic in psychiatric patients with PTSD (PTSD sample, ICD-10: F43.1, n = 14) vs. psychiatric patients without PTSD (non-PTSD sample, diagnosis other than ICD-10: F43.1, n = 142; n = 3 were excluded due to missing values).Mean values with 95%-CIs and Bonferroni-corrected pairwise comparisons. Psychosocial burden was assessed with the Goe-BSI and is presented as mean of ratings on the 11-point numeric scales for psychosocial stress, psychiatric symptomatology, and quality of life. Time-points of analyses: T1: before the pandemic (before March of 2020); at the beginning of the pandemic (mid-March 2020); first lockdown (April, 24th to May, 11th 2020); T2: second lockdown (November 27th to December, 22th 2020). Symbols: p < 0.05, ** p < 0.01, *** p < 0.001.
Symptoms of AD
As we reported previously [23], the GLM did not reveal a significant change in the ADNM-20 sum score from first to second lockdown in the total sample (F(1, 150) = .00, p = .998, ns). Focusing again on differences between the PTSD and non-PTSD subsample, we found a significant between subjects-effect with a medium effect size (F(1, 150) = 8.03, p = .005, partial η^2^ = 0.05): Symptoms of AD were generally more pronounced in patients with PTSD than in patients without PTSD for the global set of time-points (Fig 3). Again, we did not find a significant interaction effect (F(1, 150) = 0.95, ns). However, descriptive analysis suggested that patients with PTSD had an increase in AD symptoms from the first (T1: M = 50.36, SD = 15.19) to the second lockdown (Fig 3, T2: M = 51.93, SD = 12.86) whereas patients without PTSD had a decrease in AD symptoms (Fig 3, T1: M = 42.27, SD = 13.63; T2: M = 40.70, SD = 13.12). Bonferroni-corrected pairwise comparisons showed no significant difference during the first lockdown (T1: t(150) = 2.09, p = .076) but revealed a significant difference during the second lockdown, with a large effect size (T2: t(150) = 3.06, p = .005, demp = 0.86). Please see Table 4 for all mean values and differences between both subsamples.
Course of symptom levels of AD during different phases of the Covid-19 pandemic measured with the ADNM-20 in psychiatric patients with PTSD (PTSD sample, ICD-10: F43.1, n = 14) vs. psychiatric patients without PTSD (non-PTSD sample, diagnosis other than ICD-10: F43.1, n = 138; n = 7 were excluded due to missing values).Mean values with 95%-CIs and Bonferroni-corrected pairwise comparisons. Symptom level of AD was assessed with the ADNM-20 sum score (range: 20 to 80 points). Time-points of analyses: T1: first lockdown (April, 24th to May, 11th 2020); T2: second lockdown (November 27th to December, 22th 2020). Symbols: p < 0.05, ** p < 0.01, *** p < 0.001.
Exploratory analysis: Course of general psychiatric symptoms and resilience
Please see Table 2 for correlations between the diagnostic status of PTSD (yes/no) and (1) baseline sociodemographic variables in the total sample, (2) the five mostly pronounced psychiatric symptoms at second lockdown (T2), and (3) both resilience items. Three out of eleven correlations reached significance: in comparison with other diagnoses, PTSD status correlated directly with sum of F-diagnoses (Table 2, r = -0.284, p < .001), inversely with living space (r = -0.196, p = .017), and directly with loss of joy (r = 0.161, p = .043). However, following the definition by Cohen (1988), these r-values are to be interpreted between “small” (r = 0.10) and “medium” (r = 0.30) [46].
The development of a total of 22 pre-defined psychiatric symptoms was analyzed in the PTSD sample between the first (T1) vs. the second lockdown (T2) – please see Table 1 for all pairwise comparisons and items. In sum, analyses did not reveal any significant difference for these items; however, a trend (p < .100) could be found for three variables: (1) the time spent with internet/media decreased from first to second lockdown (p = .080), (2/3) both, the attention to symptoms of illness in others and the patients themselves, increased from first to second lockdown (p = .092 and .095). We found no effect of the ongoing pandemic on subjectively perceived resilience as both items did not differ between T1 and T2 in patients with PTSD (Table 1, p = .847 and.707).
Discussion
To the best of our knowledge, this is the first study directly comparing the influence of the COVID-19 pandemic on psychosocial burden and AD symptom load as measures of stress coping in psychiatric patients with vs. without PTSD. This finding is of clinical relevance since, although both PTSD and AD belong to the group of stress-related disorders in the ICD-10, they have clear diagnostic boundaries and require different types of treatment [47]. In summary, we found that, in relation to psychiatric patients without PTSD, the pandemic-related stress response pattern of patients with PTSD showed both a significantly higher psychosocial burden and AD severity during the COVID-19 pandemic.
Interestingly a deviation in pandemic-related stress response pattern was found between the subgroups. Psychosocial burden and AD severity differed significantly between both samples during the latest time-point during the pandemic examined here (second lockdown): While both outcomes are suggestive of an improvement for patients without PTSD, they seem to relatively aggravate in those with this type of stress-related disorder. This might suggest that, among adult psychiatric populations, patients with PTSD have a particularly high stress vulnerability and/or a particularly impaired stress coping which might, in turn, contribute to a possibly reduced resilience as described in previous literature (e.g., [26]). Specifically, the latter hypothesis is in line with previous findings showing that coping of various stressors is reduced in individuals suffering from PTSD (e.g., [38]) and that stress coping abilities differ between various psychiatric disorders (e.g., [37,40]). Accordingly, stress-coping styles have been found altered in PTSD [48,49]. Interestingly, several studies suggest that the time-point of traumatization, in particular traumata survived in childhood vs. those experienced in adulthood, highly likely modulates the psychological and/or molecular stress response in PTSD [38,50]. Thus, for future experiments, it would be highly interesting to assess whether patients with PTSD caused by childhood vs. those with PTSD caused by adulthood traumata respond differently to chronic multifaceted stressors such as the COVID-19 pandemic.
Speculatively, the higher comorbidity load (here: 2.79 vs. 1.74 F-Diagnoses) and the comparably smaller living spaces (here: < 60m^2^ vs.> 95m^2^) might contribute to their relative increase in vulnerability for stress caused by the pandemic: As PTSD is highly associated with an increased comorbidity of other mental disorders like substance abuse, anxiety disorders or major depression including suicidal ideation [51], coping with stressors may be impeded due to a higher overall symptom load. A smaller living space under 60m^2^ can significantly increase the level of depressive symptoms [52] – this would also potentially impede stress coping and the development of a high level of resilience. However, the relation between smaller living space and stress coping specifically in patients with PTSD has not yet been investigated. Of note, and in contrast to the previously published total sample [23], this could not be verified here as we found no changes in resilience in the PTSD sample. Clearly, the two resilience items of the Goe-BSI inventory employed in this study do not reflect every facet of psychological resilience. As stated by multiple authors (see [53] for an overview) the lacking perception of “own controllability” during the pandemic may indicate a decreased resilience level. This may have been an additional long-term stressor in patients with PTSD during the pandemic, and should be considered for a next version of the Goe-BSI.
The results of this study are limited by various factors, mainly by the small PTSD sample size that classifies it as an exploratory study. These small numbers did not allow Bonferroni-correction between GLM main effects, but, at least, Bonferroni-correction of post-hoc tests. The inclusion of a healthy control group would have been desirable to analyze the impact of the pandemic on mental health in comparison with psychiatric patients, and to improve the overall sample size. Furthermore, our study relied on a monocentric convenience sample which may be considered less representative for a global population of patients with PTSD. The reliance on self-report scales (psychosocial burden, ADNM-20, resilience, psychiatric symptoms) may be subject to biases and should be supplemented by clinician/expert ratings in future studies.
PTSD has been assessed in daily clinical routine by treating clinical experts, which is clearly a strength of our study regarding the fact that many (online) surveys exclusively rely on self-reported diagnoses only. However, systematically using validated diagnostic inventories would add more preciseness to the differentiation of the PTSD and the non-PTSD sample in future studies. So would the additional use of stress coping style questionnaires. In addition, using an approach combining current and retrospective data, we cannot fully exclude the creation of pseudo-trajectories of psychosocial burden and thus the retrospective estimations included in our study must be interpreted with caution [23]. Finally, as we stated previously [23,41], several ICD-10 diagnoses are underrepresented in this convenience sample, in particular diagnoses belonging to the ICD-10 chapters F1 and F5. In sum, the assessment of patients under “pandemic conditions” did largely dictate our inclusion criteria, longitudinal design, and the methods of statistical analysis (see points above). As described, the instruments presented here constituted a compromise to measure a valid stress response pattern and had to be partially developed (Goe-BSI) during the first phase of the pandemic in 2020 – please see our previous studies [23,41] for detailed information (scale development and quality criteria).
Taken together, we provide preliminary and first evidence that, among psychiatric populations, patients with PTSD might be particularly burdened by comorbid AD symptoms and psychosocial stress load in response to the COVID-19 pandemic. The well-known enhanced stress vulnerability of patients with PTSD (e.g., [37,38,50]) might significantly contribute to these findings. Of note, in contrast to the majority of studies on the biological and psychological stress coping in PTSD patients that employed artificially generated stressors such as the Trier Social Stress Test, our study shows that impaired stress coping in patients with PTSD is relevant also in a real-world context. Even though the COVID-19 pandemic has been overcome, this study calls for awareness of the here-proposed exceptionally high vulnerability of patients with PTSD. Other real-world stressors like globally increasing social tensions may have a comparable effect on such patients, but are neither sufficiently investigated nor comparable to a pandemic situation with far-reaching restrictions. The risk of future global pandemics will potentially increase further due to global warming and livestock farming [54], leading to the necessity for policy makers to ensure care of highly vulnerable patients in such times (e.g., via telemedicine).
Based on the experience gathered here, future pandemic-related studies should aim to implement multiple improvements: (1) acquisition of a larger sample size, possibly within a multicenter approach, to also enable the analysis of moderating factors (e.g., trauma type 1 vs. 2); (2) initiation of the first assessment as early as possible, to reduce the number of potentially biased retrospective assessments; (3) implementation of additional measures (e.g., stress coping) and comprehensive measurement of resilience.
Supporting information
S1 FileDataset of the study.The minimal dataset of the study is provided as SAV-file (SPSS).(SAV)
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1WHO Coronavirus (COVID-19) Dashboard. [cited 8 Feb 2023]. Available from: https://covid 19.who.int
- 2Bäuerle A, Teufel M, Musche V, Weismüller B, Kohler H, Hetkamp M, et al. Increased generalized anxiety, depression and distress during the COVID-19 pandemic: a cross-sectional study in Germany. J Public Health (Oxf). 2020;42(4):672–8. doi: 10.1093/pubmed/fdaa 106 32657323 PMC 7454766 · doi ↗ · pubmed ↗
- 3Cooke JE, Eirich R, Racine N, Madigan S. Prevalence of posttraumatic and general psychological stress during COVID-19: a rapid review and meta-analysis. Psychiatry Res. 2020;292:113347. doi: 10.1016/j.psychres.2020.113347 32763477 PMC 7392847 · doi ↗ · pubmed ↗
- 4Gilan D, Röthke N, Blessin M, Kunzler A, Stoffers-Winterling J, Müssig M, et al. Psychomorbidity, resilience, and exacerbating and protective factors during the SARS-Co V-2 pandemic. Dtsch Arztebl Int. 2020;117(38):625–30. doi: 10.3238/arztebl.2020.0625 33200744 PMC 7817784 · doi ↗ · pubmed ↗
- 5Huang Y, Zhao N. Generalized anxiety disorder, depressive symptoms and sleep quality during COVID-19 outbreak in China: a web-based cross-sectional survey. Psychiatry Res. 2020;288:112954. doi: 10.1016/j.psychres.2020.112954 32325383 PMC 7152913 · doi ↗ · pubmed ↗
- 6Li J, Yang Z, Qiu H, Wang Y, Jian L, Ji J, et al. Anxiety and depression among general population in China at the peak of the COVID-19 epidemic. World Psychiatry. 2020;19(2):249–50. doi: 10.1002/wps.20758 32394560 PMC 7214959 · doi ↗ · pubmed ↗
- 7Mc Ginty EE, Presskreischer R, Han H, Barry CL. Psychological distress and loneliness reported by US Adults in 2018 and April 2020. JAMA. 2020;324(1):93–4. doi: 10.1001/jama.2020.9740 32492088 PMC 7270868 · doi ↗ · pubmed ↗
- 8Petzold MB, Bendau A, Plag J, Pyrkosch L, Mascarell Maricic L, Betzler F, et al. Risk, resilience, psychological distress, and anxiety at the beginning of the COVID-19 pandemic in Germany. Brain Behav. 2020;10(9):e 01745. doi: 10.1002/brb 3.1745 32633464 PMC 7361063 · doi ↗ · pubmed ↗