Counseling and Educating About Vasa Previa Using Intraoperative Photographs of Vessel Rupture: A Case Report
Allan Barraza, Amy J Gagnon

TL;DR
This case report shows how intraoperative photos can help educate and counsel about the risks of vasa previa during cesarean delivery.
Contribution
The use of intraoperative photographs to visually demonstrate vasa previa rupture is proposed as a novel educational and counseling tool.
Findings
Intraoperative photos captured the rupture of fetal vessels during a scheduled cesarean for type I vasa previa.
Visual documentation can enhance understanding of the condition's acuity for learners and patients.
Abstract
Vasa previa describes vessels that are unprotected by Wharton’s jelly and traverse over or near the endocervix. Rupture of membranes or labor increases the risk of vessel rupture, followed by rapid fetal exsanguination. Learners are often taught to manage this condition by case scenarios and simulations. We present a case of type I vasa previa where intraoperative photographs demonstrate the potentially catastrophic rupture of membranes into the unprotected fetal vessels during a scheduled cesarean delivery. We recommend using intraoperative photographs to educate learners and counsel patients on the potential acuity inherent to this condition.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
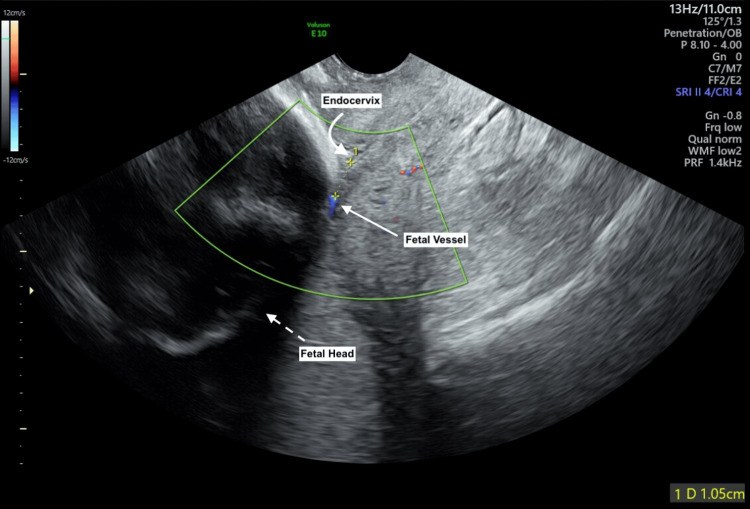 Figure 1
Figure 1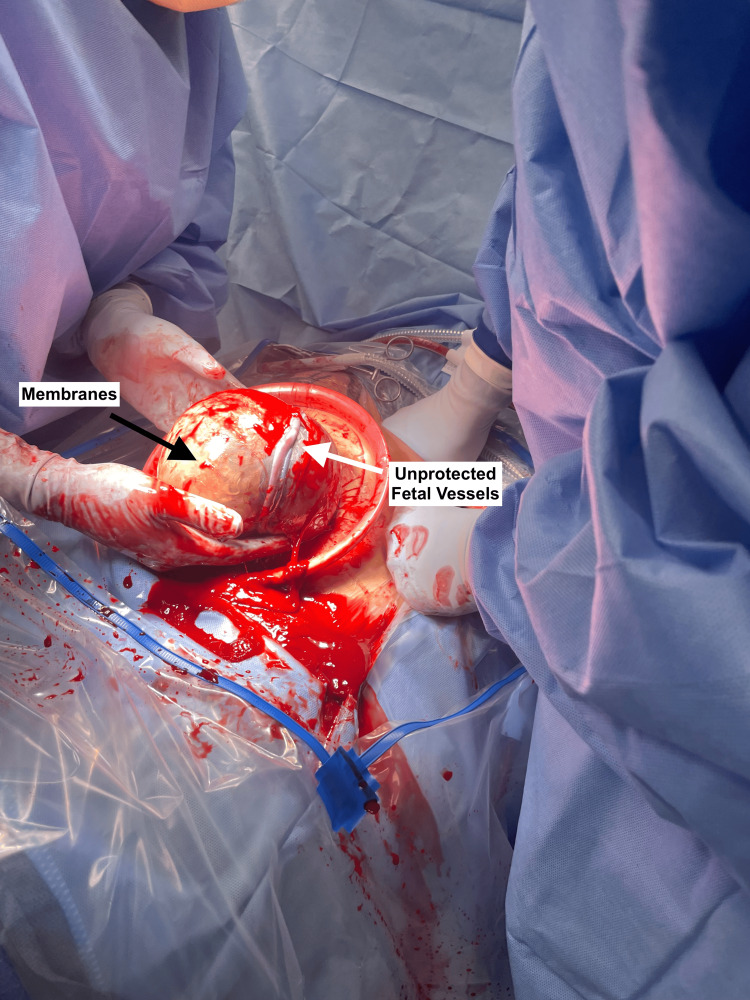 Figure 2
Figure 2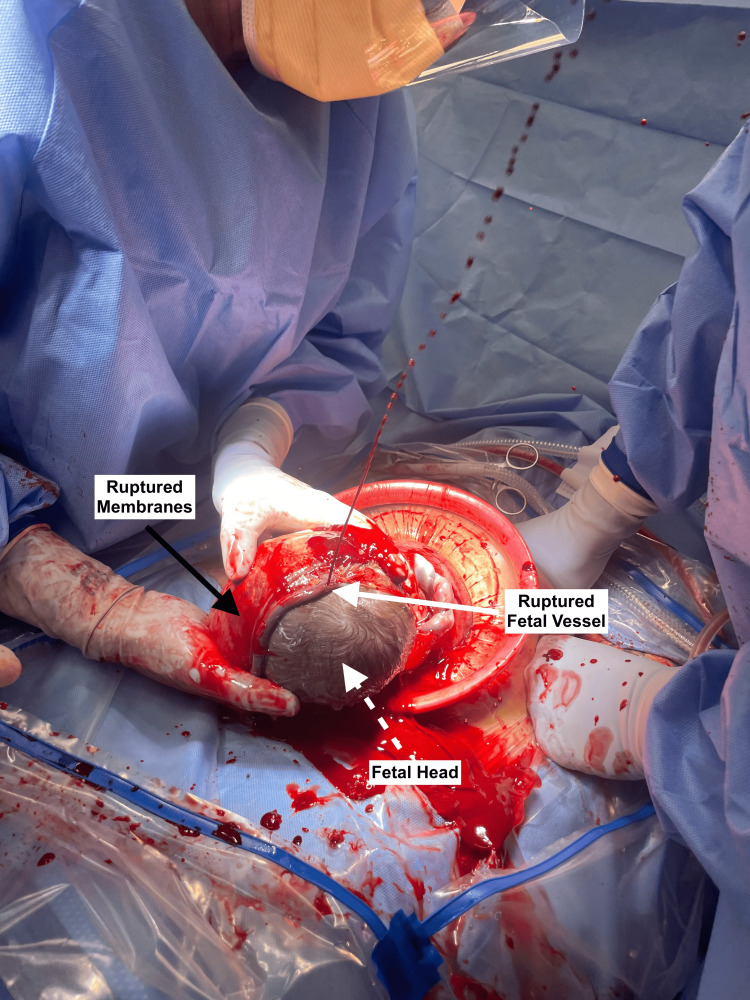 Figure 3
Figure 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsTrauma Management and Diagnosis · Vascular Procedures and Complications · Maternal and fetal healthcare
Introduction
Vasa previa describes fetal vessels that are not covered by Wharton’s jelly and traverse over or proximal to the endocervix [1]. Vasa previa affects around 1 in 2,500 births and is classified into three types [1]. Type I vasa previa occurs when a velamentous placental cord insertion has unprotected fetal vessels within the membranes over or near the endocervix [1]. Type II vasa previa occurs when unprotected fetal vessels connecting a succenturiate or multilobed placenta traverse over or near the endocervix [1]. Type III vasa previa occurs when unprotected vessels connecting two placental edges traverse over or near the endocervix [2]. Vasa previa incurs the risk of fetal exsanguination at the time of membrane rupture or onset of labor. For this reason, inpatient surveillance and antenatal corticosteroids are considered as early as 28 weeks, followed by planned cesarean delivery between 34 and 37 weeks [1,3].
Neonatal survival for vasa previa is as high as 97.6%, largely secondary to improvements in prenatal diagnosis at the second-trimester ultrasound [1]. Mortality approaches 56% when vasa previa is not diagnosed antenatally [1]. Careful surgical skill during cesarean delivery is also essential for a good outcome, with surgeons being mindful of the location of the unprotected fetal vessels. This can be accomplished by exposing the membranes and incising them away from the vessels or attempting fetal delivery en caul [2]. Perioperative ultrasound mapping may also be considered [2,4].
However, prolonged antepartum admissions are known to cause social and financial hardship on patients, many of whom also have jobs and young children [5,6]. One in three antepartum patients have clinically significant anxiety and depression, twice the prevalence of the general obstetric population [4]. Asymptomatic patients with vasa previa may be hesitant to the recommendation for admission due to these socioeconomic implications. Thorough counseling by providers is imperative to achieving patient engagement and shared decision making.
Providers, caregivers, and support staff are educated on vasa previa by written case scenarios and simulation exercises. While these activities help care teams understand the management of vasa previa, there is a potential gap in illustrating the acuity inherent to this diagnosis. We present a case where intraoperative photographs of vessel rupture during a scheduled cesarean section were used for patient counseling and multidisciplinary education on the acuity of a ruptured vasa previa.
Case presentation
A 30-year-old gravida 2 para 1001 at 22 weeks gestation was referred to Maternal Fetal Medicine (MFM) following a second trimester screening ultrasound where fetal vessels were overlying the endocervix. An MFM ultrasound confirmed the diagnosis of type I vasa previa, with a velamentous cord insertion at 1.9 cm from the endocervix. Serial interval ultrasounds confirmed persistent type I vasa previa with these vessels lying at 1.05 cm from the endocervix at 32 weeks gestation (Figure 1).
Transvaginal ultrasound using color Doppler to locate unprotected fetal vessels in type 1 vasa previa.Transvaginal ultrasound at 32 weeks gestation where color Doppler identified an unprotected fetal vessel (straight arrow) overlying the fetal head (dotted arrow) at 1.05 cm from the endocervix (curved arrow).
The patient was admitted at 32 weeks gestation for inpatient surveillance. At admission, she received a course of antenatal corticosteroids and fetal monitoring three times per day. A shared decision was made by the obstetrician, MFM, and the patient to schedule a cesarean delivery at 35 weeks with intraoperative photographs to document the vasa previa.
The patient remained stable without signs of preterm labor or rupture of membranes. Her cesarean delivery occurred at 35 weeks, as planned. The surgeon carefully incised the uterus, visualizing the unprotected fetal vessels overlying the fetal head (Figure 2). An attempt was made for en caul delivery or delivering the fetus with unruptured membranes. Spontaneous rupture of membranes occurred during the fetal delivery and extended into the unprotected fetal vessels (Figure 3). Rapid and high-pressure bleeding ensued and was managed with expeditious fetal delivery and immediate cord clamping. The neonate was resuscitated in the delivery room and had APGAR scores of 8 and 9 at 1 and 5 minutes, respectively. The neonate was hemodynamically stable and without signs of anemia throughout their admission.
Attempted en caul delivery for type I vasa previa.Surgeons attempting an en caul cesarean delivery, where the fetus is delivered with unruptured membranes. The unprotected fetal vessels (white arrow) are overlying the fetal head, surrounded by intact membranes (black arrow).
Spontaneous rupture of membranes extending into unprotected fetal vessels of a type I vasa previa during attempted en caul delivery.Spontaneous rupture of membranes (black arrow) during an attempted en caul cesarean delivery for type 1 vasa previa, resulting in rupture of an unprotected fetal vessel (white arrow) overlying the fetal head (white dotted arrow).
Discussion
Vasa previa is a diagnosis that can lead to one of the highest-acuity scenarios at a labor and delivery unit, fetal exsanguination. Obstetric trainees are indoctrinated on the urgency of this diagnosis via case scenarios on standardized exams and simulation drills.
This case offers the opportunistic benefit of photographic evidence to demonstrate the brisk fetal bleeding that can occur when a fetal vessel is ruptured. Figure 2 demonstrates the attempted en caul delivery after carefully entering the uterine cavity and exposing the membranes. Figure 3 clearly depicts the high-pressure fetal bleeding after spontaneous rupture of these vessels during an attempt at en caul delivery.
These photographs were validating to the patient as she better understood the reason for her prolonged antepartum admission. She initially was hesitant for prolonged inpatient management, as she was asymptomatic throughout her pregnancy and did not easily perceive the risk surrounding vasa previa. This is not uncommon for obstetric patients faced with the recommendation for a prolonged hospitalization, as these experiences have been associated with anxiety, financial hardship, and social isolation [4,5]. Observational studies by Doyle and Hesson et al. have shown that patient involvement in their care via counseling and feeling listened to can improve their satisfaction [4,5]. We encourage that these photos be used to supplement counseling in a way that engages patients to achieve shared decision making.
With the patient's consent, these photographs were used for multidisciplinary education. These were shared with a team of physicians, nurse midwives, and nurses at a teaching hospital during a daily education meeting. The patient's case was de-identified and presented, using the photographs to illustrate the acuity of vessel rupture.
We consider that these photographs can be incorporated into multidisciplinary obstetric emergency simulations and professional competency exams. In addition, the nursing and medical student clinical rotation experience can be enhanced by reviewing these photographs as part of an obstetric emergency lecture. Future improvements would include recreating this image into a physical model that demonstrates the velocity at which fetal intravascular volume is depleted with vessel rupture during labor or cesarean delivery.
Conclusions
This clinical scenario is an excellent demonstration of the continuum of screening, diagnosis, and management of vasa previa. These intraoperative photographs can be used to counsel patients and educate providers and support staff on the potential for sudden acuity that is inherent to vasa previa. We encourage other care teams to consider obtaining intraoperative photographs at the time of a vasa previa cesarean section.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1#37: diagnosis and management of vasa previa Am J Obstet Gynecol Sinkey RG Odibo AO Dashe JS 61561921320152629204810.1016/j.ajog.2015.08.031 · doi ↗ · pubmed ↗
- 2Vasa previa Obstet Gynecol Oyelese Y Javinani A Shamshirsaz AA 50351814220233759098110.1097/AOG.0000000000005287 PMC 10424826 · doi ↗ · pubmed ↗
- 3Medically indicated late-preterm and early-term deliveries: ACOG Committee Opinion, number 831 Obstet Gynecol 09138202110.1097/AOG.000000000000444734259491 · doi ↗ · pubmed ↗
- 4Prevalence of depression or anxiety during antepartum hospitalizations for obstetric complications: a systematic review and meta-analysis Obstet Gynecol Toscano M Royzer R Castillo D Li D Poleshuck E 88189113720213383192810.1097/AOG.0000000000004335 PMC 8087456 · doi ↗ · pubmed ↗
- 5Maternal stressors during prolonged antepartum hospitalization following transfer for maternal-fetal indications Am J Perinatol Doyle NM Monga M Kerr M Hollier LM 27302120041501747910.1055/s-2004-820506 · doi ↗ · pubmed ↗
- 6There's no place like home: optimizing the antepartum inpatient experience Matern Health Neonatol Perinatol Hesson AM Davuluri K Corbin CK Rujan AM Berman DR 151020243908594610.1186/s 40748-024-00185-5PMC 11293146 · doi ↗ · pubmed ↗