Incidence of fidaxomicin allergy in patients with macrolide allergies: a large database analysis
Chia-Yu Chiu, Daniel B. Chastain, Madison E. Salam, Joseph Sassine, Andrés F. Henao-Martínez

TL;DR
The study finds that patients with macrolide allergies have a higher risk of developing an allergy to fidaxomicin, with varying odds depending on the specific macrolide.
Contribution
The study quantifies the increased risk of fidaxomicin allergy in patients with specific macrolide allergies using large database analysis.
Findings
Patients with azithromycin allergy had 2.31 times higher odds of fidaxomicin allergy.
Anaphylaxis and angioedema risk was highest within one year of a non-fidaxomicin macrolide allergy.
Abstract
Fidaxomicin may exhibit cross-reactivity in patients with known macrolide allergies. In this analysis, compared to patients without macrolide allergies, the odds of fidaxomicin allergy were 2.31, 8.37, and 1.58 times higher in patients with azithromycin, clarithromycin, and erythromycin allergies, respectively; the absolute risk of fidaxomicin allergy was 0.033, 0.01, and 0.039 in patients with azithromycin, clarithromycin, and erythromycin allergies, respectively. The highest risk of anaphylaxis and angioedema was observed within 1 year of a non-fidaxomicin macrolide allergy.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
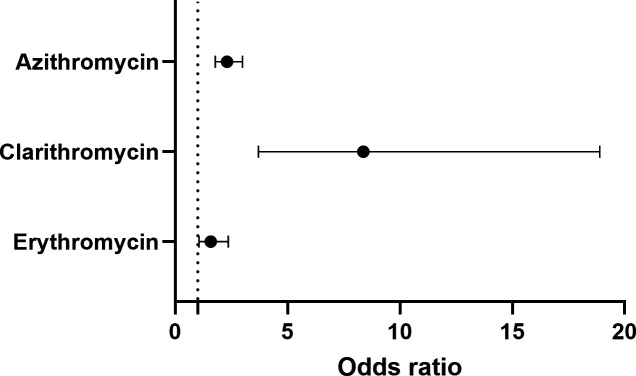 Fig 1
Fig 1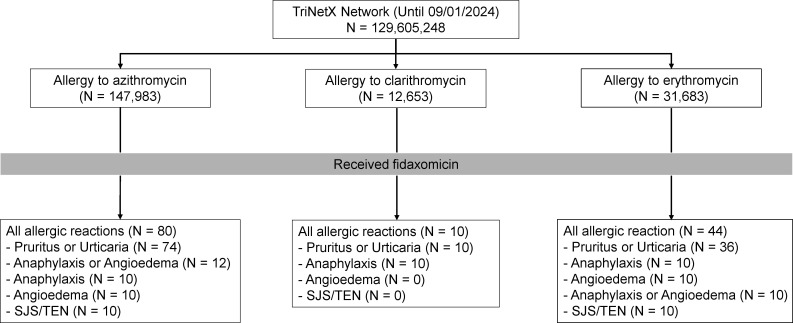 Fig 2
Fig 2| Total | ≤1 year | >1 year | |
|---|---|---|---|
| Azithromycin | |||
| All allergic reactions | 80 | 43 (54%) | 37 (46%) |
| Pruritus or urticaria | 74 | 42 (57%) | 32 (43%) |
| Anaphylaxis or angioedema | 12 | 10 (83%) | 2 (17%) |
| SJS/TEN | 10 | 10 (100%) | 0 (0%) |
| Clarithromycin | |||
| All allergic reactions | 10 | 10 (100%) | 0 (0%) |
| Erythromycin | |||
| All allergic reactions | 44 | 26 (59%) | 18 (41%) |
| Pruritus or urticaria | 36 | 23 (64%) | 13 (36%) |
| Anaphylaxis or angioedema | 10 | 10 (100%) | 0 (0%) |
| SJS/TEN | 10 | 0 (0%) | 10 (100%) |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsDrug-Induced Adverse Reactions · Asthma and respiratory diseases · Respiratory and Cough-Related Research
INTRODUCTION
Adverse event rates for non-fidaxomicin macrolides range from 6% to 27%, with hypersensitivity reactions occurring in only 0.4% to 3% of cases (1, 2). Due to structural similarities, the fidaxomicin package insert warns clinicians about the potential for cross-reactivity in patients with known macrolide allergies (3). We conducted a retrospective analysis using the TriNetX database to investigate the incidence of patients with pre-existing non-fidaxomicin macrolide allergies who experienced allergic reactions to fidaxomicin.
On 1 September 2024, we queried TriNetX (4), a global research network database that includes data from 100 million patients of all ages across more than 80 medical centers in multiple countries. The supplemental methods provide detailed information on the TriNetX framework and study design. Our group has published several reports using the same methodology, including studies on adverse drug reactions (5, 6).
Baseline characteristic macrolide allergy
At the time of analysis, 129,605,248 patients were included in the TriNetX database. We identified 147,983, 12,653, 31,683, and 1,902 patients with documented allergies to azithromycin, clarithromycin, erythromycin, and fidaxomicin, respectively. The estimated incidence rates of allergy to azithromycin, clarithromycin, erythromycin, and fidaxomicin were 114.2 (95% CI 113.6–114.8), 9.8 (95% CI 9.6–9.9), 24.5 (95% CI 24.2–24.7), and 1.47 (95% CI 1.40–1.54) per 100,000 patients, respectively.
Compared to patients without macrolide allergies, the odds of an allergic reaction to fidaxomicin were 2.31 times (95% CI 1.78–2.99) higher in patients with an azithromycin allergy, 8.37 times (95% CI 3.70–18.90) higher with a clarithromycin allergy, and 1.58 times (95% CI 1.06–2.36) higher with an erythromycin allergy (Fig. 1). The absolute risk of an allergic reaction to fidaxomicin was 0.033 in patients with an azithromycin allergy (80 of the 2,410 patients with a documented azithromycin allergy developed fidaxomicin allergy), 0.01 in patients with a clarithromycin allergy (10 of the 997 patients with a documented clarithromycin allergy developed fidaxomicin allergy), and 0.039 in patients with an erythromycin allergy (44 of the 1,124 patients with a documented erythromycin allergy developed fidaxomicin allergy) (Table S2).
Odds ratio of fidaxomicin allergy in patients with other macrolide allergy. The odds ratios of fidaxomicin allergic reactions in patients with a history of azithromycin, clarithromycin, and erythromycin allergy were 2.31 (95% CI 1.78–2.99), 8.37 (95% CI 3.70–18.90), and 1.58 (95% CI 1.06–2.36), respectively.
Allergy to non-fidaxomicin macrolide and fidaxomicin
In total, 80 patients with a documented azithromycin allergy, 10 with a clarithromycin allergy, and 44 with an erythromycin allergy developed an allergic reaction to fidaxomicin (Table S3; Fig. 2). Anaphylaxis/angioedema and SJS/TEN were more frequent in patients whose azithromycin allergy was recorded within 1 year compared to those documented more than 1 year earlier (83% vs. 17% and 100% vs. 0%, respectively). All 10 patients with a clarithromycin allergy experienced anaphylaxis and pruritus/urticaria, with no cases of angioedema or SJS/TEN. In addition, these patients were all labeled with clarithromycin allergies within 1 year before fidaxomicin administration. Anaphylaxis/angioedema occurred exclusively in patients with erythromycin allergies documented within 1 year before fidaxomicin administration. By contrast, SJS/TEN occurred exclusively in patients labeled with erythromycin allergy more than 1 year before fidaxomicin administration. Notably, patients with anaphylaxis/angioedema were distinct from those with SJS/TEN across all groups (Table 1).
Patients with a non-fidaxomicin macrolide allergy label experienced allergic reactions to fidaxomicin. SJS/TEN, Stevens-Johnson syndrome/toxic epidermal necrolysis.
Fidaxomicin contains an 18-membered lactone ring and has negligible systemic absorption, with plasma concentrations below 20 ng/mL, primarily remaining with the colon (2, 7). By contrast, macrolides with a 14-membered lactone ring (clarithromycin, erythromycin) or a 15-membered lactone ring (azithromycin) have better oral bioavailability (2, 7, 8). Due to their structural similarities, these macrolides may theoretically exhibit cross-reactivity (2, 3). However, this may not occur frequently because of the negligible systemic absorption of fidaxomicin. In addition, hypersensitivity reactions and allergies to macrolides are relatively uncommon compared to other antibiotics (2, 9), making it challenging to study cross-reactions between different macrolides.
In clinical trials, no cases of anaphylaxis due to fidaxomicin have been reported, or patients with a known fidaxomicin allergy were excluded from participation (10–12). The most common allergic reactions to fidaxomicin were gastrointestinal symptoms (5–10%), neutropenia (2%), and anemia (2%) (3). In post-marketing data, two small case series reported a relationship between fidaxomicin allergies and prior allergies to other macrolides (Table S4) (8, 13). Iarikov et al. reported three females (two with erythromycin allergy and one with azithromycin/erythromycin allergy) developed hypersensitivity reactions (one with pruritus/urticaria, one with throat itching without angioedema, and one with angioedema) after receiving fidaxomicin (13). Conversely, Kufel et al. reported no case of fidaxomicin allergy or intolerance in 11 patients with a history of macrolide allergy (eight with erythromycin allergy and three with azithromycin allergy) (8). In our study, anaphylaxis/angioedema predominantly occurred within 1 year of a non-fidaxomicin macrolide allergy. However, in patients with a clarithromycin allergy, all experienced anaphylaxis alone without angioedema (Table 1). Importantly, we observed that a non-fidaxomicin macrolide allergy increases the risk of fidaxomicin allergy (Fig. 1).
Cutaneous manifestations of antibiotic allergies encompass a broad spectrum of clinical phenotypes with varying onset times and immune mechanisms (14). In our study, pruritus/urticaria were the most common allergic reactions but were not reported in patients with a history of clarithromycin allergy more than 1 year before fidaxomicin administration. In addition, SJS/TEN occurred exclusively in patients with an azithromycin allergy documented within 1 year before fidaxomicin administration. In comparison, it occurred exclusively in those with an erythromycin allergy documented more than 1 year before fidaxomicin administration (Table 1). Although drug eruptions or pruritus occurred in less than 2% of patients receiving fidaxomicin in Clostridioides difficile infection (CDI) clinical trials (3), a handful of hypersensitivity cases have been reported post-marketing in the FDA adverse Event Reporting System (15). It is possible that in patients with non-fidaxomicin macrolide allergies, re-exposure to a similar chemical structure, even with minimal serum levels of fidaxomicin, could trigger severe hypersensitivity or severe cutaneous adverse events.
Our study has several limitations, primarily due to its retrospective design and the available information in TriNetX. Second, the reported macrolide allergies were presumably self-reported, and we could not confirm the index reactions. Cross-reactivity would ostensibly produce the same reaction, mediated by the same immune pathway (16). Therefore, dissimilar reactions may indicate a lower likelihood of true cross-reactivity. Literature on penicillin allergies indicates that self-reported allergies are less likely to involve cross-reactivity to cefazolin, underscoring the importance of validating and characterizing patients’ allergies (17). Third, fidaxomicin intolerance was not included in our search because these gastrointestinal symptoms are difficult to differentiate from those of CDI.
In summary, although macrolide allergies are infrequent, a history of non-fidaxomicin macrolide allergy slightly increases the risk of fidaxomicin allergy, particularly within 1 year of the initial allergy. Given the low absolute risk of fidaxomicin allergic reactions in patients with macrolide allergies and the minimal systemic absorption of fidaxomicin, we recommend accurately documenting the history of non-fidaxomicin macrolide allergies and closely monitoring patients for adverse drug reactions when administering fidaxomicin.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Araújo L, Demoly P. 2008. Macrolides allergy. Curr Pharm Des 14:2840–2862. doi:10.2174/13816120878636981218991703 · doi ↗ · pubmed ↗
- 2Shaeer KM, Chahine EB, Varghese Gupta S, Cho JC. 2019. Macrolide allergic reactions. Pharmacy 7:135. doi:10.3390/pharmacy 703013531540456 PMC 6789826 · doi ↗ · pubmed ↗
- 32020. Dificid (Fidaxomicin) package insert. Available from: https://www.accessdata.fda.gov/drugsatfda_docs/label/2020/213138 lbl.pdf
- 4Tri Net X. 2024. Available from: https://trinetx.com. Retrieved 1 Dec 2024.
- 5Henao-Martínez AF, Chastain DB, Thompson GR. 2023. Treatment pathways, switches, and inappropriate treatment during invasive pulmonary aspergillosis: real-world experiences from a global research network study. Antimicrob Agents Chemother 67:e 0072123. doi:10.1128/aac.00721-2337671871 PMC 10583675 · doi ↗ · pubmed ↗
- 6Chiu C-Y, Henao-Martínez AF, Agudelo Higuita NI. 2025. Incidence of anaphylaxis in patients with alpha-gal syndrome receiving gelatin-containing vaccines: a large database analysis. J Allergy Clin Immunol Pract 13:421–423. doi:10.1016/j.jaip.2024.11.01039579978 · doi ↗ · pubmed ↗
- 7Venugopal AA, Johnson S. 2012. Fidaxomicin: a novel macrocyclic antibiotic approved for treatment of Clostridium difficile infection. Clin Infect Dis 54:568–574. doi:10.1093/cid/cir 83022156854 · doi ↗ · pubmed ↗
- 8Kufel WD, Hitchcock AM, Delbalso AN, Paolino KM. 2023. Evaluation of fidaxomicin use in patients with a macrolide allergy/intolerance. J Antimicrob Chemother 78:1127–1128. doi:10.1093/jac/dkad 03636790902 · doi ↗ · pubmed ↗