Assessing user experience with the Bioline™ HCV point-of-care test in primary healthcare settings: a mixed-methods study
Evans Duah, Evans Mantiri Mathebula, Kuhlula Maluleke, Tinyiko Violet Baloyi, Richard Kobina Dadzie Ephraim, Tivani Mashamba-Thompson

TL;DR
This study evaluates how well healthcare workers in Ghana can use a point-of-care test for Hepatitis C in clinics without labs.
Contribution
The study provides new insights into the usability and acceptability of the Bioline™ HCV POC test in resource-limited PHC settings using the REASSURED criteria.
Findings
The test scored 88.7 on the System Usability Scale, with 88% of HCWs finding it easy to use.
81.5% of HCWs completed all testing steps independently, but 83% made errors, mainly during pre-testing.
Qualitative feedback showed high acceptance and confidence, but storage infrastructure was a challenge.
Abstract
Hepatitis C Virus (HCV) is a major public health challenge, particularly in resource-limited settings with inadequate diagnostic services. The Bioline™ HCV Point-of-Care (POC) test provides a promising solution for improving diagnosis in Primary Healthcare (PHC) clinics without laboratory infrastructure. This study evaluated the test’s usability, acceptability, and deliverability in Ghana using user-oriented REASSURED criteria. A convergent parallel mixed-methods design was adopted. Quantitative data was collected through direct observation of Healthcare Workers (HCWs) using audit checklists and analyzed with Stata 16. The analysis included descriptive statistics, inter-rater concordance assessment, and the application of the System Usability Scale (SUS). Qualitative data, analyzed using Atlas.ti 24.2.0, explored user experiences, confidence, storage infrastructure, and suggestions for…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
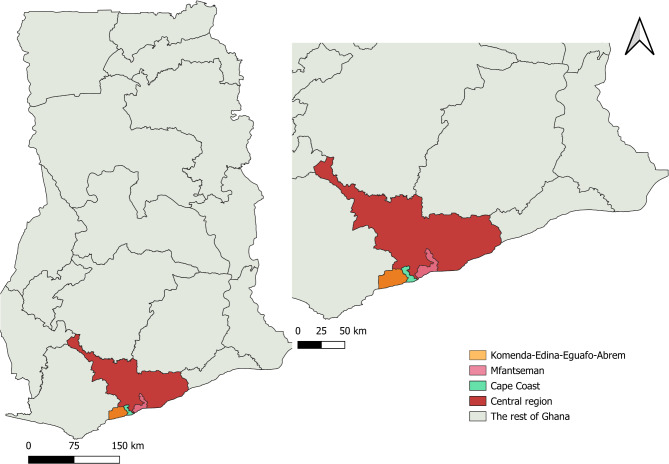 Figure 1
Figure 1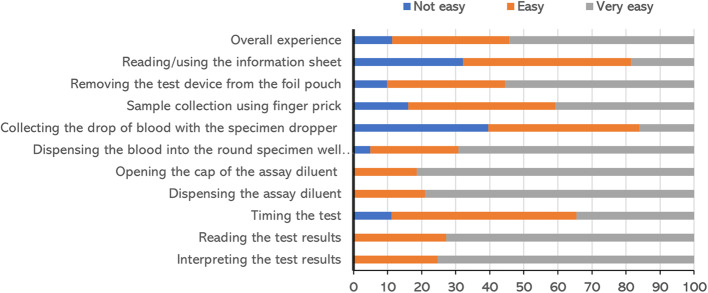 Figure 2
Figure 2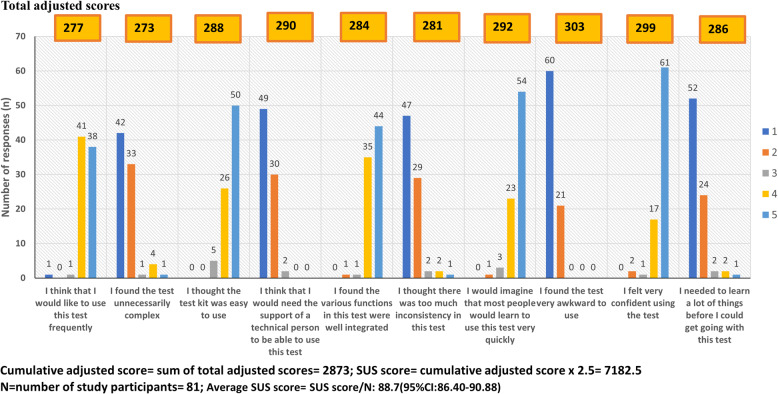 Figure 3
Figure 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsHepatitis C virus research · HIV, Drug Use, Sexual Risk
Introduction
Hepatitis C Virus (HCV) infection, often termed a “silent epidemic”, is a major public health challenge due to its typically asymptomatic nature and delayed diagnosis [1]. Globally, over 130 million individuals are affected by HCV [2], with 58 million living with chronic infection [3], of whom more than 50% are unaware of their status [4]. Sub-Saharan Africa (SSA) accounts for over 2% of the global HCV burden, with more than 200,000 viral hepatitis-related deaths annually [5, 6]. Ghana, like most SSA countries, is impacted by HCV, with studies reporting an HCV seroprevalence of 1–3% [7–9], though national viraemic prevalence remains undocumented.
The World Health Organization (WHO) promotes innovative diagnostic approaches to ensure equitable access and linkage to care, aiming to reduce viral hepatitis mortality by 65% and new infections by 90% by 2030 [10]. While countries like Egypt have expanded community-based HCV testing to meet diagnostic demands [11], Ghana faces challenges in addressing disparities between urban and rural, hard-to-reach communities.
Early detection is critical for linkage to care and treatment with Direct-Acting Antivirals (DAAs) [3]. Point-of-Care (POC) diagnostics offer near-bedside rapid testing, addressing diagnostic needs in hard-to-reach, resource-limited communities typical of low-middle-income countries (LMICs) [12]. In Ghana, there is a significant demand for POC services in Primary Healthcare (PHC) clinics, especially in remote areas where centralized laboratories are either unavailable or located hours away [13]. The Bioline™ HCV POC test (Abbott Rapid Diagnostics) provides an accessible alternative, promoting equitable access to diagnostics and facilitating early detection [14]. This test is WHO prequalified, market-authorized, and CE-marked for use in multiple regions [14].
However, limited research exists on Healthcare Workers’ (HCWs) User Experience (UX) with HCV POC tests in SSA’s PHC settings. Most diagnostic trials in SSA focus on clinical performance in laboratory environments [15], often excluding African populations and favoring high-income countries. Meanwhile, user-oriented indicators, such as ease of specimen collection, user-friendliness, rapidity, and deliverability, are commonly assessed using HCV self-tests [16–18].
The present study constituted part of a diagnostic trial that aimed to evaluate the Bioline™ HCV POC test in PHC settings in Ghana using the Real-time connectivity, Ease of specimen collection, Affordability, Sensitivity, Specificity, User-friendliness, Rapidity and robustness, Equipment-free, and Deliverability (REASSURED) criteria as a benchmark [19]. Guided by the Morville UX Honeycomb model [20], we specifically investigated the UX, employing a mixed-methods design to evaluate the usability, acceptability, and deliverability of the Bioline™ HCV POC test among non-laboratory HCWs in PHC clinics in Ghana’s Central Region.
Methods
Study design
A convergent parallel mixed-methods design was used to evaluate the UX of the Bioline™ HCV POC test as part of a broader diagnostic trial registered in the Pan African Clinical Trial Registry (PACTR202410837698664) whose protocol is published elsewhere [19]. The study was conducted from August-December 2024.
Study setting
The study was conducted in the Central region of Ghana (5.6444° N, 1.2891° W) (Fig. 1), covering 42 Community-based Health Planning and Services (CHPS) facilities across Cape Coast, Komenda-Edina-Eguafo-Abirem (KEEA), and Mfantseman districts. These facilities, identified as PHC clinics, were purposively selected based on the study objectives (Additional file 1).
Fig. 1. Map of the Central Region of Ghana highlighting the three study districts
Study population
Non-laboratory HCWs at the PHC clinics including nurses and midwives were recruited to participate in this study.
Participants selection and eligibility criteria
Inclusion criteria
- All PHC clinics within the three districts (Cape Coast, KEEA, and Mfantseman) were eligible to be included in the study.
- All staff of the PHC clinics were eligible to participate in the study.
Exclusion criteria
- PHC clinics that had laboratories were excluded from the study.
- All PHC clinics that did not have physical structures were excluded from the study.
- All laboratory staff of the clinics were excluded from the study.
- Participants who withdrew consent were excluded from the study.
- Interns and non-medical support staff at the PHC clinics were excluded from the study.
HCWs who met the eligibility criteria were selected through purposive sampling.
Sample size
Using Yamane’s sample size formula, a minimum of 80 HCWs were required to obtain a representative sample from the available 100 HCWs at the PHC clinics to ensure study validity [21].
\documentclass[12pt]{minimal} \usepackage{amsmath} \usepackage{wasysym} \usepackage{amsfonts} \usepackage{amssymb} \usepackage{amsbsy} \usepackage{mathrsfs} \usepackage{upgreek} \setlength{\oddsidemargin}{-69pt} \begin{document}$$\:{n}_{1}\ge\:N/(1+N{e}^{2})$$\end{document}
Where:
N = The total number of HCWs available at the PHC clinics in the three districts = 100
e = margin of error = 5% =0.05 at 95% Confidence Interval
\documentclass[12pt]{minimal} \usepackage{amsmath} \usepackage{wasysym} \usepackage{amsfonts} \usepackage{amssymb} \usepackage{amsbsy} \usepackage{mathrsfs} \usepackage{upgreek} \setlength{\oddsidemargin}{-69pt} \begin{document}$$\:n_1\geq\:N/(1+Ne^2)$$\end{document}
\documentclass[12pt]{minimal} \usepackage{amsmath} \usepackage{wasysym} \usepackage{amsfonts} \usepackage{amssymb} \usepackage{amsbsy} \usepackage{mathrsfs} \usepackage{upgreek} \setlength{\oddsidemargin}{-69pt} \begin{document}$$\:n_1\geq\:100/((1+100\left(0.05\right)^2)$$\end{document}
\documentclass[12pt]{minimal} \usepackage{amsmath} \usepackage{wasysym} \usepackage{amsfonts} \usepackage{amssymb} \usepackage{amsbsy} \usepackage{mathrsfs} \usepackage{upgreek} \setlength{\oddsidemargin}{-69pt} \begin{document}$$\:{n}_{1}\ge\:80$$\end{document}
Also, the minimum required sample size for the qualitative component was set at 20 in-depth interviews until data saturation was reached.
Study procedures
The Bioline™ HCV test is a manually performed, immunochromatographic IVD for detecting HCV antibodies in human serum, plasma, or whole blood at POC within 5 to 20 min [14]. It has a sensitivity of 99.3% and specificity of 98.1% [14]. The test is WHO prequalified, CE marked [14], and registered with the Ghana FDA (FDA/D.21–11702) [19]. Its packaging includes test cassettes, safety lancets, specimen droppers, alcohol swabs, diluent, and instructions (Additional file 2), designed for resource-limited settings, especially in SSA.
The manufacturer’s test instructions included both text and diagramatic illustrations in multiple languages. The Bioline™ HCV test workflow adapted from the test instruction leaflet for this study involved a 23-step process categorized into 3 phases i.e. pre-testing, testing and post-testing (Additional file 3).
Quantitative methods
The principal investigator and trained research assistants (medical laboratory scientists, nurses, and public health officers) demonstrated the Bioline™ HCV test workflow to participants according to the manufacturer’s instructions. A baseline questionnaire collected sociodemographic data, including sex assigned at birth, education, occupation, and rank. Participants were paired to perform the HCV test on each other, interpreting results while referring to the instructions. Research assistants observed the 23-step process, documenting errors and difficulties (Additional file 3).
Inter-reader and inter-operator concordance were estimated by comparing participants’ results with those of the research assistants. Participants also tested one of randomly-selected five blinded standard samples (A to E), and the results were compared to known outcomes. A 10-item Likert-scale questionnaire was used to assess the participants’ experiences after testing (Additional file 3).
Finally, the standard and validated System Usability Scale (SUS) was employed to evaluate user interactions with the test and their experiences [22]. The standard SUS, comprising ten 5-point Likert-scale items alternating between positive (odd) and negative (even) statements, assesses test usability and overall user satisfaction (Additional file 3). The SUS scores range from 0 to 100, with scores ≤ 51.8 indicating the system requires fixing; 51.9–67.9: system improvement is recommended; 68–73.9: high usability but potential for improvement exists; 74–80.2: high usability; ≥80.3: excellent usability [23]. The standard SUS score for a set of raw item ratings from each respondent was calculated using the following formula:
\documentclass[12pt]{minimal} \usepackage{amsmath} \usepackage{wasysym} \usepackage{amsfonts} \usepackage{amssymb} \usepackage{amsbsy} \usepackage{mathrsfs} \usepackage{upgreek} \setlength{\oddsidemargin}{-69pt} \begin{document}$$\:SUS\:score=\left(\sum\limits_{i=\text{1,3},\text{5,7},9}{(score}_{i}-1)+\sum\limits_{i=\text{2,4},\text{6,8},10}{(5-score}_{i})\right)\times\:\:2.5$$\end{document}Statements 1, 3, 5, 7, and 9 represent the odd or positive statements, while statements 2, 4, 6, 8, and 10 represent the even or negative statements. The frequencies of responses for each Likert scale option (1–5) for each statement were enumerated and adjusted according to the following adjusted score rules:
- Odd-numbered items: Adjusted score = Response score– 1 = 0, 1, 2, 3, 4
- Even-numbered items: Adjusted score = 5 - response score = 4, 3, 2, 1, 0
To obtain total adjusted scores, the frequency of each response was multiplied by its adjusted score. The cumulative adjusted score was calculated as the sum of the total adjusted scores. The average SUS for N number of respondents was computed as:
\documentclass[12pt]{minimal} \usepackage{amsmath} \usepackage{wasysym} \usepackage{amsfonts} \usepackage{amssymb} \usepackage{amsbsy} \usepackage{mathrsfs} \usepackage{upgreek} \setlength{\oddsidemargin}{-69pt} \begin{document}$$\:Average\:SUS\:score=\frac{SUS\:score}{N}$$\end{document}Qualitative methods
Concurrently, the study explored users’ experiences and acceptability of the Bioline™ HCV test through qualitative methods. In-depth interviews were conducted using a semi-structured guide (Additional file 4), consisting of 15 open-ended questions about participants’ experiences, confidence, usability, reliability of the test instructions, challenges, ease of sample collection, quality assurance, and recommendations. Interviews, lasting 20–45 min, were conducted in Fanti, Twi, or English, based on participant preference. They were audio-recorded, with field notes taken to supplement the recordings.
Data management and analysis
Quantitative data
Quantitative data were entered into Microsoft Excel, cleaned for duplicates, missing data, and errors, then exported to Stata/IC version 16 [24]. Descriptive statistics were used to summarize the study population, presented as frequencies and percentages. Estimates of errors, difficulties, and assistance during the hands-on audit were generated. HCV invalid ratings by PHC non-laboratory HCWs were also estimated. Inter-rater concordance (inter-reader and inter-operator) was calculated as percentage agreement and Cohen’s kappa coefficient. SUS scores were computed using the provided formula. Statistical results were presented in tables and graphs, with all tests two-sided, a 95% confidence interval, and p < 0.05.
Qualitative data
Interview recordings were transcribed verbatim in Microsoft Word, with translations of local languages into English, and then exported to ATLAS.ti software version 24.2.0 [25]. Two independent coders (ED and TVB) used thematic analysis to inductively code the data in parallel [26]. Inter-coder reliability was assessed using percent agreement (85.4%), the Holsti index (0.91), and Krippendorff’s alpha-binary coefficient (0.909), all indicating acceptable agreement (≥ 80% or ≥ 0.80) (Additional file 5) [27]. Major themes and sub-themes were generated to explore users’ experiences of the Bioline™ HCV test, following Braun & Clarke’s six-phase framework: familiarizing with data, extracting codes, generating themes, reviewing themes, defining themes, and writing up [26]. Results were presented as relevant quotes from the transcripts.
Results
Characteristics of the study participants
Table 1 presents the sociodemographic characteristics of 81 non-laboratory HCWs with a median age of 34 years (IQR:31–37), recruited from PHC clinics across three districts: Cape Coast (34.6%), Mfantseman (33.3%), and KEEA (32.1%). Participants had a median total work experience of 8 years (IQR:4–11). Most participants were females (91.4%), with certificate-level education (59.3%) and diplomas (33.3%). Nurses constituted the largest occupational group (76.6%), followed by midwives (22.2%). Participants included community health nurses (20.9%) and senior community health nurses (23.5%) being the most common. Leadership roles were held by 39.5% of participants, with 34.6% serving as general managers of the PHC clinic.Table 1. Sociodemographic characteristics of study participantsVariablesN = 81n(%)Median age, years (IQR^^)34(31–37)Median total working experience, years (IQR^^)8(4–11)Median working experience in that specific PHC clinic, years (IQR^^)2(1–4)Sex assigned at birth Male7(8.6) Female74(91.4)Highest level of education Certificate (1–2 years)48(59.3) Diploma (3 years)27(33.3) Degree (4 years)6(7.4)Occupation Health Assistant1(1.2) Midwife18(22.2) Nurse62(76.6)Rank Community health nurse17(20.9) Senior community health nurse19(23.5) Principal community health nurse11(13.6) Enrolled nurse3(3.7) Senior enrolled nurse5(6.2) Principal enrolled nurse1(1.2) Midwifery officer7(8.7) Senior midwifery officer2(2.5) Nursing officer1(1.2) Principal health assistant1(1.2) Senior public health nurse1(1.2) Staff midwife2(2.5) Senior staff midwife7(8.7) Staff nurse3(3.7) Senior staff nurse1(1.2)Leadership role General manager28(34.6) RCH^#^ unit manager4(4.9) None49(60.5)Distribution by district KEEA^∞^26(32.1) Cape Coast28(34.6) Mfantseman27(33.3)^^IQR Inter-quartile range, PHC Primary healthcare^#^RCH Reproductive and child health^∞^KEEA Komenda-Edina-Eguafo-Abrem
The in-depth interviews included 22 HCWs, of whom 17 were facility managers. Detailed description is provided in Additional file 6.
Table 2 summarizes the characteristics of the PHC clinics included in the study. These were 42 CHPS compounds with physical structures distributed across three districts: KEEA (35.7%), Cape Coast (31.0%), and Mfantseman (33.3%). The condition of roads leading to the clinics was predominantly poor but pliable (59.5%). The majority of the clinics (95.2%) lacked air-conditioned storage infrastructure.Table 2. Characteristics of the PHC clinicsVariablesN = 42n(%)District KEEA^^15(35.7) Cape Coast13(31.0) Mfantseman14(33.3)Condition of road leading to PHC^#^ clinic Good15(35.7) Poor but pliable25(59.5) Non-pliable2(4.8)Availability of air-conditioned storage room No40(95.2) Yes2(4.8)^^KEEA Komenda-Edina-Eguafo-Abrem^#^PHC Primary healthcare
Results of the hands-on usability audit of the Bioline™ HCV POC are presented in Table 3. Out of the 81 study participants, 33 opted to perform self-testing, either because they were the only healthcare worker on duty at the time of the study or to maintain confidentiality, as they did not want a colleague (testing partner) to know their HCV status. Overall, errors were observed in about 83% of the participnats for at least one step, common among those with testing partners (100% vs. 57.6%, p < 0.0001). Pre-testing errors were common, with 64.2% failing to wash and dry their hands, 62.9% not reading or using the test information sheet, and 60.5% not wearing examination gloves. Specifically, significantly higher percentage of self-testers failed to wear examination gloves (100% vs. 33.3%, p < 0.0001) compared with those with testing partners. However, most participants with testing partners failed to read or use the test information sheet (72.9% vs. 48.5%, p = 0.03) compared with self-testers. During testing, 37.0% failed to wipe away the first drop of blood, and 27.2% did not collect the required 10 µl of blood. There were minimal or no post-testing errors. Difficulties were noted in 18.5% of participants for at least one step, primarily in removing the test device from the foil (13.6%) and using the specimen dropper (8.6%). Assistance was provided in 18.5% of cases for at least one step, mainly for timing the test (12.4%). Despite the errors and challenges, 81.5% completed all steps without assistance and reported correct test results, with self-testers showing a higher success rate than testing partners (87.9% vs. 77.1%).Table 3. Bioline™ HCV POC hands-on usability audit: observed errors, difficulties and assistance providedVariablesOverallN = 81Testing partnerN = 48Self-testN = 33P-valuen(%)n(%)n(%)Observed errorsPre-testing Failed to wash hands and dried52(64.2)29(60.4)23(69.7)0.39 Replaced handwash with hand sanitizer23(28.4)9(18.8)14(42.4)- Didn’t read/use test information sheet51(62.9)35(72.9)16(48.5)0.03* Didn’t place the test kit on a flat surface1(1.2)1(2.1)0(0.0)1.00 Didn’t wear examination gloves49(60.5)16(33.3)33(100.0)< 0.0001* Failed to label the test kit28(34.6)19(39.6)9(27.3)0.25Testing Chose the wrong finger for fingerpricking0(0.0)0(0.0)0(0.0)- Didn’t massage and warm finger5(6.2)4(8.3)1(3.0)0.64 Failed to clean the finger with an alcohol swab and let it dry0(0.0)0(0.0)0(0.0)- Didn’t press down firmly to prick their skin1(1.2)1(2.1)0(0.0)1.00 Unsafe disposal of the used lancet0(0.0)0(0.0)0(0.0)- Didn’t wipe away the first drop of blood30(37.0)19(39.6)11(33.3)0.57 Didn’t use the specimen dropper1(1.2)1(2.1)0(0.0)- Failed to collect the blood up to the marked ring of the specimen dropper (10 µl)22(27.2)15(31.3)7(21.2)0.32 Didn’t drop the whole blood into the round specimen well (marked ‘S’)1(1.2)0(0.0)1(3.0)0.65 Unsafe disposal of used specimen dropper0(0.0)0(0.0)0(0.0)- Didn’t use the assay diluent0(0.0)0(0.0)0(0.0)- Failed to dispense exactly 4 drops of the assay diluent8(9.9)7(14.6)1(3.0)0.13 Didn’t close the cap of the assay diluent after use1(1.2)1(2.1)0(0.0)1.00 Didn’t time the test10(12.4)8(16.7)2(6.1)0.17Post-testing Read the test results outside the stipulated time (5–20 min)0(0.0)0(0.0)0(0.0)- Read/interpreted the results incorrectly0(0.0)0(0.0)0(0.0)- Unsafe disposal of the used test kit0(0.0)0(0.0)0(0.0)-Errors observed for at least one step67(82.7)48(100.0)19(57.6)< 0.0001Observed difficulties Removing the test device from the foil11(13.6)6(12.5)5(15.2)0.73 Using the specimen dropper7(8.6)7(14.6)0(0.0)0.41Experienced difficulties for at least one step15(18.5)12(25.0)3(9.1)0.09Assistance provided Asked for more information mid-way testing1(1.2)1(2.1)0(0.0)1.00 Reminded by testing partner to clean finder with alcohol swab1(1.2)1(2.1)0(0.0)1.00 Collecting blood with specimen dropper4(4.9)2(4.2)2(6.1)0.41 Dispensing blood from the specimen dropper unto the test kit1(1.2)0(0.0)1(3.0)1.00 Timing10(12.4)8(16.7)2(6.1)0.17Assistance provided for at least one step15(18.5)11(22.9)4(12.1)0.26All steps completed correctly without assistance and test results reported correctly66(81.5)37(77.1)29(87.9)0.26^^Statistically significant at p < 0.05
The qualitative findings highlight similar challenges as part of the five emerging themes contributing to these difficulties and errors, particularly issues with the test instruction sheet and specimen dropper (Additional file 7).
Challenge with reading/using the test instruction sheet
Participants found the instruction leaflet cumbersome due to its size, multiple languages, small font, and overwhelming appearance (Additional file 8).
“When I saw the leaflet,* I got scared. I was like*,* “Ei*,* what is this big thing? When will I even finish reading this? (She laughed)”* (HCW of PHC clinic 19)
“I had a little difficulty with the pamphlet (instruction sheet). It’s quite large and includes multiple languages,* which made it hard to locate the specific information needed to perform the test”* (HCW of PHC clinic 11)
“The font is too small for some of us with poor eyesight” (HCW of PHC clinic 13)
Challenge with using the specimen dropper
Approximately half of the participants struggled with the sample dropper (Additional file 8).
“I had a problem with the pipette. I had to press it before picking up the sample. It requires some skill to do that. If you don’t know how,* you can’t take enough sample for the test”* (HCW of PHC clinic 14)
However, the study participants suggested several modifications to enhance the usability and functionality of the Bioline™ HCV POC test (Additional file 7).
Suggestion to modify the test package
Participants emphasized the need for integrating all test components into a single packaging unit to prevent shortages and improve convenience.“Okay. I would suggest they improve the packaging. If the pipette (dropper) and lancet are included in the foil with the cassette,* it would be more convenient. That way*,* when you pick one*,* everything you need is inside. Currently*,* since the pipettes and lancets are packed separately*,* sometimes we run out of them even though we still have cassettes available. Including them together would solve this issue”* (HCW of PHC clinic 1)
Suggestion to include additional consumables
Recommendations were made for manufacturers to consider.
“They should include additional droppers since we may accidentally drop them while working” (HCW of PHC clinic 2)
***“*Adding lancet holders would be very helpful, as it would reduce clients’ fear of needles by hiding the needle during finger pricks… (HCW of PHC clinic 3)
“You should add a lancet holder to automate the pricking process and protect us from needle pricks during our work. This would also reduce the pain caused by the prick” (HCW of PHC clinic 4)
“We often lack sufficient gloves. Including gloves,* even simple rubber gloves*,* in the test package would greatly enhance safety”* (HCW of PHC clinic 7)
“…including a timer would be beneficial to help with timing,* as we might forget to check the result on time”* (HCW of PHC clinic 3)
Suggestion to modify specimen dropper
Similarly, recommendations were made for the modification of the sample dropper.“I would recommend changing the pipette (dropper). It’s difficult to pick the sample with it compared to what we are used to with the malaria RDT. With the malaria RDT,* you don’t need to press or hold anything to pick the sample. It picks the sample with just a touch”* (HCW of PHC clinic 6)
Suggestion to modify test instruction sheet
Participants made suggestions for test design improvement.“…the leaflet should be simplified. I don’t know if this is in Chinese,* but if you’re bringing the test to this level of healthcare in Ghana*,* most of us are certificate and diploma holders. When someone sees a language other than English*,* they might not even continue to look at the instructions. So*,* I would recommend designing a country-specific leaflet with test instructions in diagrams showing the steps*,* to make it simpler and easier to read”* (HCW of PHC clinic 14)
The HCWs shared their experiences on the ease-of-use of the Bioline™ HCV POC test as illustrated in Fig. 2. Overall, 88% of the HCWs found the test easy or very easy to use with various ease-of-use ratings in the testing steps. The commonest difficulty was with the use of the sample dropper (Fig. 2).
Fig. 2. Ease-of-use of the Bioline™ HCV POC test: user-experience audit
The in-depth interviews complement the UX findings, highlighting the test’s ease-of-use and the participants willingness to use and recommend to other PHC clinics outside the study districts (Additional file 7).
Ease-of-use of the test
The Bioline™ HCV POC test was widely regarded as simple and user-friendly by the HCWs.
“Every equipment needed for the test is found in the small box. You don’t need any other equipment to perform the test,* which makes it very simple to use”* (HCW of PHC clinic 18)
“The test kit is quite compact and lightweight. It’s something we can easily work with” (HCW of PHC clinic 11)
Willingness to use test in the PHC clinics
As the first point of contact for healthcare in underserved areas, the partcipants expressed strong willingness to use the test.“Yes. As the first point of contact in the hierarchy of Ghana’s health service,* having this test kit will make our work much easier. Clients will no longer need to travel long distances and incur financial costs for laboratory tests” (HCW of PHC clinic 7)*
Willingness to recommend to other PHC clinics
Participants noted that misconceptions about higher healthcare levels often deter community members from seeking care, making PHC clinics the preferred point for diagnostic services hence their willingness to recommend to all PHC settings.
“Yes. Most people in these communities see hospitals as something big,* so they are scared to go there. They are comfortable coming to the CHPS compounds since we are closer to their homes. It will also make the HCV diagnostic service easily accessible to them” (HCW of PHC clinic 15)*
“Yes,* it will be very helpful because most community members prefer accessing healthcare in CHPS zones (PHC clinics). Even when referred to a higher level of care*,* they often refuse to go. They are scared of larger health facilities. Having this test will help us diagnose them here and provide appropriate follow-up treatment” (HCW of PHC clinic 12)*
The overall usability score for the Bioline™ HCV POC was 88.7 (95% CI: 86.40–90.88) based on the validated SUS scale as shown in Fig. 3.
Fig. 3. Bioline™ HCV POC test usability assessment using the SUS scale
The overall inter-reader and inter-operator concordance was high using both the person-testing and standard sample testing approaches (100%, Cohen’s kappa coefficient:1.00 ± 0.11, p-value < 0.0001), with no invalid rating recorded (Additional file 9).
Discussion
The overall usability score of the Bioline™ HCV POC test was 88.7 (95% CI: 86.40–90.88), an excellent rating according to the SUS [22]. This finding highlights the test’s ease of use, acceptability, and practicality, making it suitable for adoption in resource-limited PHC settings with minimal additional resources or training. While the SUS is widely used in technology and consumer electronics [22], its application in healthcare and diagnostics is growing. For instance, similar usability scores were recorded for the SureStatus POC SARS-CoV-2 Antigen test (85.0) in India and Germany [28], and the Abbott i-STAT^®^ POC blood analyzer (84.0) in Canada [23]. Comparable studies in South Africa also reported high usability scores (90.7–94.9%) for HCV self-tests [29].
In this study, 88% of HCWs found the test easy or very easy to use, consistent with the high usability scores and qualitative feedback. The compact design, rapid results, and familiarity with rapid diagnostic testing contributed to this positive perception. The finger-prick procedure was also straightforward, with minimal discomfort for patients. Familiarity with dual-format instruction sheets further improved ease of use, reflecting findings from other studies where usability scores were similarly high among lay users of HCV self-tests in South Africa [29], and Georgia [16].
Approximately 81.5% of HCWs successfully completed all test steps without assistance and reported accurate results, with no invalid ratings, yielding 100% inter-rater reliability. This performance surpasses findings from a similar study in Georgia, where 60–80% of lay users correctly completed HCV tests without assistance [16]. This discrepancy may reflect differences in target populations, with HCWs being more familiar with diagnostic procedures than lay users. This was evident in lay users occasionally misinterpreting the test lines and facing difficulties distinguishing between positive and negative results [16].
Despite these successes, errors were observed in 83% of participants during at least one testing step, primarily in the pre-testing phase. Common errors included failure to wash hands (64.2%), not using the test information sheet (62.9%), and neglecting to wear gloves (60.5%). These lapses could be attributed to overconfidence and routine familiarity with the procedures, which seemed habitual and normalized within PHC settings, as highlighted in the qualitative analysis. Furthermore, many HCWs trusted their testing partners, perceiving little need to wear gloves. The shortage of consumables, such as gloves, reported in most facilities further exacerbates these unsafe practices. In contrast, other studies rather reported post-analytic errors, such as misinterpreting test results [16, 17].
Acceptance of the Bioline™ HCV POC test was high among HCWs, who expressed willingness to recommend and use the test in PHC settings. HCWs emphasized the importance of community-based testing, citing reliance by farming and fishing communities and reluctance to visit higher-level facilities due to financial and cultural barriers. Similar acceptability trends were noted in Kenya, Egypt, Vietnam, and China, where HCV self-tests gained widespread approval despite limited literature on Bioline™ HCV POC testing among HCWs [18].
Deliverability, encompassing physical accessibility and storage capabilities, is critical for deploying the test in hard-to-reach areas. Most PHC clinics in this study had poor infrastructure and lacked temperature-controlled storage. However, HCWs demonstrated adaptability by creating suitable storage environments using existing resources. On the other hand, limited awareness of HCV RDTs among HCWs raised concerns about broader population knowledge in rural areas. For instance, a study in India found that over 50% of at-risk individuals were unaware of HCV testing due to a lack of awareness [30].
This study’s findings have significant implications for scaling up the Bioline™ HCV POC test in resource-limited settings. High usability and acceptability suggest its potential as a viable diagnostic tool, even in infrastructure-poor environments. Recommendations for improving usability include enhancing packaging, instruction sheets, and sample droppers, as well as providing supplementary components like gloves. Targeted training programs are necessary to address knowledge gaps and improve familiarity with HCV RDTs, which could enhance early detection and management of the disease.
Policy efforts should prioritize integrating user-friendly POC tools into national health programs and addressing infrastructural challenges. Continuous implementation research is needed to monitor usability under real-world conditions, optimize delivery mechanisms, and compare performance with alternative diagnostics. The adaptability and resilience demonstrated by HCWs in overcoming logistical challenges underscore the potential for deploying similar tests in other low-resource settings, contributing to global health goals for HCV care and prevention.
Despite its strengths, the study is limited by potential response bias, as HCWs were aware of being observed. However, the use of validated tools like the SUS, well-trained research assistants, and observational audits helped mitigate this risk. The congruence between quantitative and qualitative findings further supports the study’s validity and reliability.
Conclusion
Our study evaluated the UX of non-laboratory HCWs with the Bioline™ HCV POC test in Ghana, highlighting its usability, acceptability, and deliverability. Despite some procedural errors and infrastructure challenges, HCWs found the test user-friendly, rapid, and suitable for resource-limited settings. The findings suggest the test’s potential for integration, with recommendations for targeted training and design improvements. These outcomes align with SDG 3 by promoting equitable access to HCV diagnostics, advancing Universal Health Coverage, and addressing health disparities in underserved regions.
Supplementary Information
Additional file 1.
Additional file 2.
Additional file 3.
Additional file 4.
Additional file 5.
Additional file 6.
Additional file 7.
Additional file 8.
Additional file 9.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1WHO. Hepatitis C. World Health Organization. 2023. [cited 2023 Sep 2]. Available from: https://www.who.int/news-room/fact-sheets/detail/hepatitis-c.
- 2WHO. Hepatitis: disease burden. World Health Oganisation. 2021. Available from: https://www.afro.who.int/health-topics/hepatitis.
- 3Agyeman AA, Ofori-asenso R, Mprah A, Ashiagbor G. Epidemiology of hepatitis C virus in Ghana: a systematic review and meta-analysis. BMC Infect Dis. 2016;16(1):391. 10.1186/s 12879-016-1708-7PMC 497788327507267 · doi ↗ · pubmed ↗
- 4Birjandi MM, Oroei M. The prevalence of positive rapid diagnostic test of hepatitis C virus infection in Ghana. Pan Afr Med J. 2020;36(1):322.10.11604/pamj.2020.36.322.22490 PMC 760383433193976 · doi ↗ · pubmed ↗
- 5WHO. Hepatitis C. World Health Organization, Geneva. 2022. [cited 2022 Jun 10]. Available from: https://www.who.int/news-room/fact-sheets/detail/hepatitis-c.
- 6Larkins MC, Thombare A. Point-of-Care Testing. In: Stat Pearls. Treasure Island: Stat Pearls Publishing; 2023 [cited 2023 Sep 2]. Available from: http://www.ncbi.nlm.nih.gov/books/NBK 592387/.
- 7Abbott. Bioline™ HCV. Abbott Laboratories. 2023. [cited 2023 Sep 2]. Available from: https://www.globalpointofcare.abbott/ww/en/product-details/bioline-hcv.html.
- 8ATLAS.ti. ATLAS.ti Desktop & Web| Free Trial| Get started for free!. ATLAS.ti. 2024. [cited 2024 May 18]. Available from: https://atlasti.com/free-trial-version.