Unmasking the Basilar Culprit: A Case of Acute Posterior Circulation Stroke in a Diabetic Septuagenarian
Muhammad Rizwan Akram, FNU Veena, FNU Sabah Afroze, Matthew Peachey, Rene Elkin

TL;DR
A 76-year-old diabetic man experienced a stroke due to basilar artery stenosis, highlighting the importance of early detection and diabetes management in preventing severe outcomes.
Contribution
The case emphasizes the link between poorly controlled diabetes and posterior circulation stroke, advocating for preventative treatment in high-risk patients.
Findings
The patient showed partial neurological recovery with dual antiplatelet treatment and intensive risk factor management.
Basilar artery stenosis combined with diabetes leads to difficult therapy and poor prognosis.
Early detection and comorbidity control can improve outcomes and reduce recurrence risk in such cases.
Abstract
A 76-year-old man with poorly controlled diabetes mellitus, with an HbA1c of 10.9% (4.7%-6.4%), presents with acute right facial numbness, transient right eye foggy vision, and near syncope. Neuroimaging revealed substantial basilar artery stenosis with acute infarction in the region of the right posterior cerebral artery, impacting the medial temporal, occipital, thalamus, and midbrain. Although basilar artery stenosis is uncommon, its combination with poorly managed diabetes and posterior circulation involvement makes therapy difficult. Partial neurological recovery was observed with dual antiplatelet treatment and intensive risk factor management. Basilar artery stenosis has a poor prognosis; however, early detection, medical therapy, and comorbidity control can improve patient outcomes and reduce recurrence risk. The example further emphasizes the necessity of preventative treatment…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
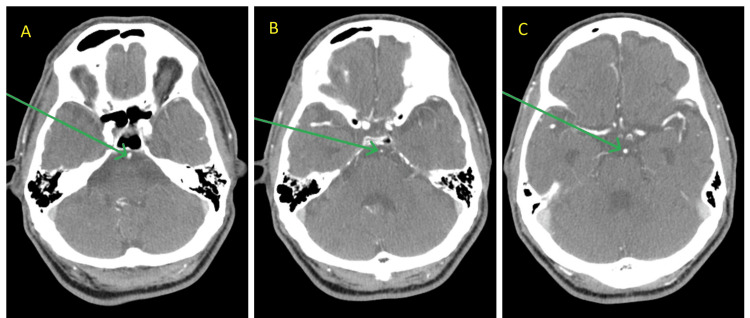 Figure 1
Figure 1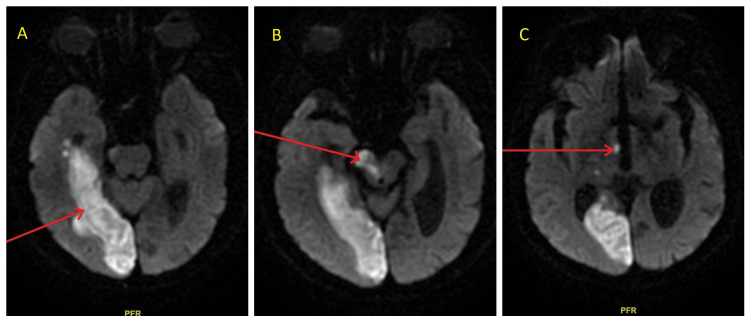 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAcute Ischemic Stroke Management · Cardiovascular Syncope and Autonomic Disorders · Cerebrovascular and Carotid Artery Diseases
Introduction
Basilar artery stenosis is an uncommon but potentially fatal cerebrovascular disease that affects around 1.43% of individuals suffering from acute ischemic stroke or transient ischemic attack [1]. The illness primarily impacts males in their sixties, with artery-to-artery embolism as the most prevalent stroke mechanism [1]. Posterior circulation strokes account for 20%-25% of all ischemic strokes, with severe basilar artery occlusive disease representing around 21.4% of posterior circulation incidents [1,2].
Basilar artery stenosis can manifest clinically in various ways, from minor symptoms to serious neurological impairments. Significant hazards are associated with the condition; research indicates that people with ≥50% basilar stenosis had a 46% 90-day probability of experiencing a transient ischemic attack or recurrent stroke [3]. Patients with ≥80% stenosis, mid-basilar placement, and poor collateral circulation face a higher risk [1].
We discuss the case of a 76-year-old patient with poorly controlled diabetes mellitus, who had abrupt neurological symptoms and was diagnosed with significant basilar artery stenosis, followed by a posterior circulation infarction. This case is notable because it highlights the complicated interplay between vascular risk factors and posterior circulation stroke, as well as the need for early detection and treatment of this potentially fatal illness [1,2].
The example also highlights the importance of complete vascular imaging in stroke evaluation and the need for aggressive risk factor management in high-risk groups to prevent repeated cerebrovascular episodes. Modern treatment strategies, such as dual antiplatelet therapy (DAPT) and high-dose statins, have shown promise in improving outcomes in these difficult situations [2,3].
Case presentation
A 76-year-old man presented to the emergency room with a chief complaint of a sudden onset of right-sided facial numbness. The patient had a history of poorly controlled diabetes mellitus, with an HbA1c of 10.9% (4.7%-6.4%), hypertension, and long-term peripheral artery disease, resulting in the amputation of the right foot toes.
The patient reported that his symptoms commenced at approximately 10 AM when he was in a pharmacy. He experienced a near-syncope episode, accompanied by hazy vision and a burning sensation in his right eye. The first vital signs showed a blood pressure of 154/50 mmHg, a heart rate of 71 beats per minute, a respiration rate of 18 breaths per minute, a temperature of 98.1°F (ca. 37°C), and an oxygen saturation of 100% in ambient air. Point-of-care glucose testing revealed hyperglycemia with a 431 mg/dL (normal, 70-120 mg/dL). An NIHSS (National Institutes of Health Stroke Scale) score of 2 was found on the neurological exam, along with signs of right-sided facial palsy affecting the lower face, tongue deflection to the right, and left-sided weakness, with motor strength of 2/5 in both the upper and lower limbs on the left side. The patient was alert and aware of his identity, surroundings, and temporal situation. A stroke code was initiated because the symptoms presented within 4.5 hours after onset. The preliminary non-contrast computed tomography (CT) scan of the head revealed no indications of an acute cerebral hemorrhage. However, stable encephalomalacia was observed in the left occipital lobe, and a lacunar infarct was observed in the left basal ganglia. CT perfusion imaging revealed a right frontal ischemic penumbra. CT angiography of the head and neck demonstrated a significant finding of short-segment severe stenosis of the basilar artery and a small V4 segment of the left vertebral artery (Figures 1A-1C). The follow-up magnetic resonance imaging (MRI) of the brain without contrast revealed an acute to early subacute infarction in the right posterior cerebral artery (PCA) territory, affecting the medial temporal and occipital lobes, and the right thalamus and midbrain (Figures 2A-2C).
CT angiography head and neckImages (A)-(C) show short-segment severe stenosis of the basilar artery at three points (arrows), where maximum stenosis is apparent in Image (B).CT: computed tomography
MRI brain without contrastImages (A)-(C) show acute or early subacute infarction (arrows) in the right posterior cerebral artery (PCA) territory, involving the medial temporal (A) and occipital lobes (A), as well as the midbrain (B) and the right thalamus (C).MRI: magnetic resonance imaging
The patient was hospitalized in the stroke unit and initiated on DAPT (aspirin and clopidogrel) in conjunction with high-dose statin therapy. Blood sugars were also well-managed while in the hospital. The neurosurgical evaluation determined that immediate surgical intervention was unnecessary.
The patient was recently hospitalized two months ago because of three observed seizures, accompanied by hyperglycemia and electrolyte abnormalities; nevertheless, the electroencephalogram (EEG) conducted at that time showed no epileptiform discharges. This recent history has introduced complexity to the contemporary presentation and management problems. The patient's health stabilized during hospitalization, with enhancement in right eye vision and preservation of stable neurological status. He required vigilant oversight and assertive alteration of risk factors, especially with his inadequately managed diabetes.
Discussion
Basilar artery stenosis constitutes a rare yet significant cerebrovascular disorder, affecting approximately 1.43% of individuals experiencing acute ischemic stroke [1]. Case studies like this one show how difficult it may be to treat and predict outcomes when diabetes mellitus is poorly managed, and significant basilar artery stenosis is also present.
Research shows that people with diabetes are more likely to get posterior circulation ischemic strokes compared to those without diabetes [4], making the association between the two conditions all the more noteworthy. Since posterior circulation arteries differ from anterior circulation vessels in vasoreactivity, wall thickness, elastin content, and concentric intima thickening, these physiological variations may be responsible for the observed connection [4].
The clinical presentation of our patient is consistent with the established elevated risk of early recurrent stroke associated with vertebrobasilar stenosis. Research indicates that patients suffering from basilar or intracranial vertebral stenosis experience a 90-day recurrent stroke rate of 33%, which is markedly higher than the 16% rate noted for extracranial vertebral stenosis [5]. The existence of significant stenosis in the basilar artery, especially when coupled with inadequate glycemic control, significantly elevates the patient's risk for unfavorable outcomes.
Our treatment strategy conformed to contemporary evidence-based guidelines. Recent guidelines for high-risk scenarios endorsed the patient's DAPT with aspirin and clopidogrel [6]. The choice to forgo immediate stenting aligned with the results of the SAMMPRIS trial, which revealed that basilar artery stenting is associated with a significantly elevated risk of peri-procedural ischemic stroke (20.8% vs. 6.7% for other arteries) [7].
The extensive imaging methodology employed in this instance, encompassing CT angiography and MRI, exemplifies contemporary best practices. Recent studies have shown how important full vascular imaging is for the diagnosis and characterization of a stroke, especially when it comes to detecting basilar artery stenosis and checking for collateral circulation [8]. The acute infarction in the right PCA region was detected by MRI, which helped determine the patient's prognosis and course of therapy.
This case emphasizes the critical need for proactive risk factor management, particularly in managing diabetes. Studies demonstrate that diabetes increases the risk of stroke by 150% to 400%, especially in cases involving posterior circulation [9]. The patient's previous toe amputations highlight the systemic aspect of his vascular disease.
Recent data endorse the application of DAPT as more beneficial than single antiplatelet therapy when started early after a small stroke or high-risk transient ischemic attack, with a decreased 90-day risk of recurrent ischemic stroke [10]. For strokes not caused by blood clots in the heart, the European Stroke Organisation (ESO) guidelines strongly recommend short-term DAPT with aspirin and clopidogrel. This is especially important in cases with high-risk factors, such as intracranial stenosis [6].
In the past, medical treatment for basilar artery stenosis was thought to have poor outcomes. However, new research shows that modern therapeutic strategies can lower death rates to as low as 2.3%, with 75% of patients having mild or no deficits at follow-up [11]. The existence of inadequately managed diabetes and considerable stenosis may affect long-term prognosis.
This shows how important it is to continue researching the best ways to treat posterior circulation strokes, especially in people who have multiple risk factors. Some endovascular techniques have shown promising results in recent trials; however, medical care remains the most important method for treating basilar stenosis [12,13].
Conclusions
This case demonstrates the complex interaction between poorly managed diabetes mellitus and basilar artery stenosis, which results in posterior circulation stroke. Basilar artery stenosis is rare but can have serious consequences; thus, it must be detected and treated promptly. We successfully treated our patient with DAPT (aspirin and clopidogrel) and aggressive risk factor modification. This case highlights the importance of employing a comprehensive treatment plan. It also shows that, although posterior circulation strokes with basilar stenosis remain challenging to manage, good results can be achieved with current therapies and close attention to other health issues that may be present.
This example shows that blood sugar control is crucial for preventing cerebrovascular accidents, particularly in the posterior circulation. Because of their numerous vascular risk factors, these patients require regular monitoring and strong preventive measures to avoid recurrent stroke and worsening cerebrovascular disease.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Stroke mechanisms and outcomes of isolated symptomatic basilar artery stenosis Stroke Vasc Neurol Samaniego EA Shaban A Ortega-Gutierrez S 189197420193203020210.1136/svn-2019-000246 PMC 6979872 · doi ↗ · pubmed ↗
- 2Isolated focal basilar artery stenosis with acute stroke treated with emergency thrombectomy and stenting Case Rep Neurol Daga K Taneja M Ahmad MT Venketasubramanian N 273312202010.1159/000506973 PMC 780247733505269 · doi ↗ · pubmed ↗
- 3Incidence and prognosis of > or = 50% symptomatic vertebral or basilar artery stenosis: prospective population-based study Brain Marquardt L Kuker W Chandratheva A Geraghty O Rothwell PM 98298813220091929324410.1093/brain/awp 026 · doi ↗ · pubmed ↗
- 4Poor glycemic control and posterior circulation ischemic stroke Neurol Clin Pract Kuroda J Matsuo R Yamaguchi Y 129139920193104112710.1212/CPJ.0000000000000608 PMC 6461411 · doi ↗ · pubmed ↗
- 5Vertebrobasilar stenosis predicts high early recurrent stroke risk in posterior circulation stroke and TIA Stroke Gulli G Khan S Markus HS 273227374020091947821010.1161/STROKEAHA.109.553859 · doi ↗ · pubmed ↗
- 6The use of dual antiplatelet therapy for ischemic cerebrovascular events Neurol Sci Mele F Gendarini C Pantoni L 37434420233611498210.1007/s 10072-022-06395-z PMC 9816218 · doi ↗ · pubmed ↗
- 7Treatment of posterior circulation stroke: acute management and secondary prevention Int J Stroke Markus HS Michel P 7237321720223565862410.1177/17474930221107500 PMC 9358302 · doi ↗ · pubmed ↗
- 8Current endovascular strategies for posterior circulation large vessel occlusion stroke: report of the Society of Neuro Interventional Surgery Standards and Guidelines Committee J Neurointerv Surg Kayan Y Meyers PM Prestigiacomo CJ Kan P Fraser JF 105510621120193110399410.1136/neurintsurg-2019-014873 · doi ↗ · pubmed ↗