Sebaceous carcinoma: clinical and demographic profile of patients in a tertiary referral hospital in Brazil
Tatiana Mina Yendo, Flavia Mascarenhas Damiani, Suzana Matayoshi, Marcello Menta Simonsen Nico

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
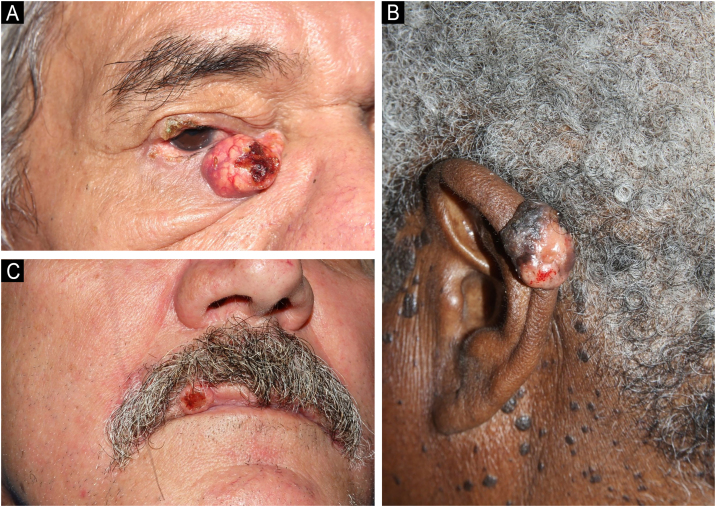 Figure 1
Figure 1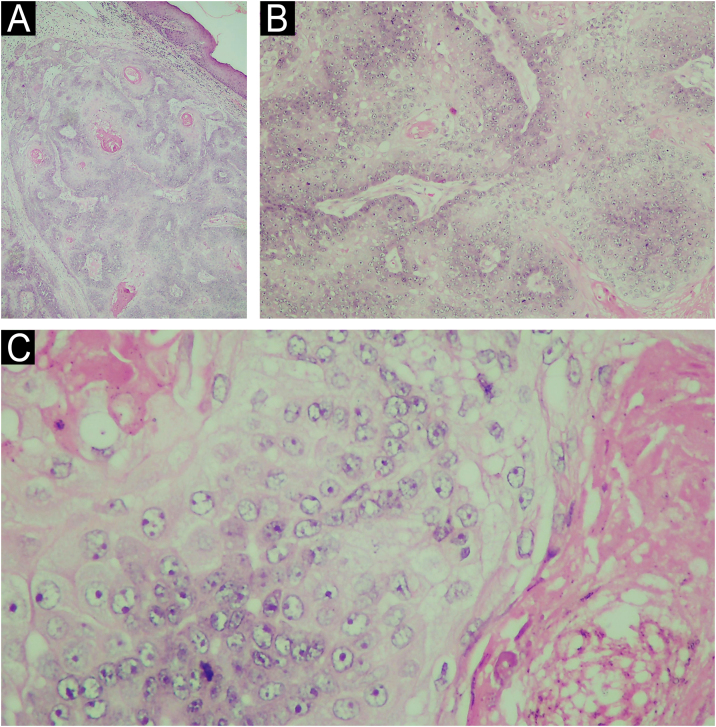 Figure 2
Figure 2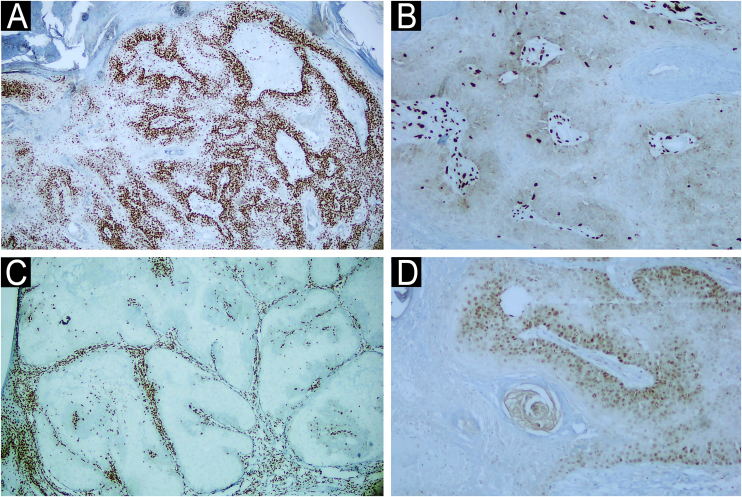 Figure 3
Figure 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsNonmelanoma Skin Cancer Studies · Herpesvirus Infections and Treatments · Polyomavirus and related diseases
Dear Editor,
Sebaceous carcinoma (SC) is a rare malignant neoplasm, described by Allaire in 1891, usually located in the head and neck and with a predilection for the periocular region (38.7%).1 It has a higher incidence in the elderly (6^th^ to 7^th^ decades of life), in males (58% of cases), and in Caucasian population (86.2%).1, 2 The authors retrospectively evaluated 22 cases of patients diagnosed with at least one SC, including three patients diagnosed with two primary SC, between January 2006 and December 2020, in a Brazilian university hospital. As described in previous studies,2 males had a higher incidence of SC, corresponding to 55% of the evaluated cases. The mean age at diagnosis was 67 years (24 to 94 years of age) and the majority of patients were Caucasian.
Clinically, the diagnosed SC showed varied characteristics, presenting as papules, plaques, nodules or tumors, generally yellowish or erythematous, with telangiectasias, a pearly gloss, keratosis or ulceration. The craniocephalic and cervical regions were preferentially affected, and, in ten cases, the SC was located in the periocular region (six in the upper eyelid and four in the lower eyelid; Fig. 1A). One case of SC was described in the neck, one in the ear pinna (Fig. 1B), three in the malar region, five in the nasal region, one in the scalp, one in the lip (Fig. 1C) and one in the chin. Only two SC were diagnosed outside the head and neck area (shoulder and chest). Nine patients were investigated for the presence of Muir-Torre Syndrome (MTS), and only four had the loss of expression of at least one mismatch repair gene confirmed by immunohistochemistry. Half of the studied cases had a diagnosis of other skin tumors such as basal cell carcinomas (BCC), squamous cell carcinomas (SCC), sebaceous adenomas and sebaceomas, single or multiple, with or without association with MTS. Moreover, eight cases had a diagnosis of non-skin neoplasms such as (1) invasive ductal breast carcinoma (without association with MTS), (2) Hodgkin's lymphoma, (3) non-Hodgkin's lymphoma and colon adenocarcinoma, (4) bilateral retinoblastoma (not investigated for MTS), (5) colon adenocarcinoma, (6) sigmoid neuroendocrine tumor and hepatocarcinoma, (7) colon adenocarcinoma, duodenal papilla adenocarcinoma with liver metastasis and prostate adenocarcinoma, (8) colon adenocarcinoma and multiple myeloma (confirmed for MTS).Fig. 1. Clinical photographs of sebaceous carcinomas. (A) Sebaceous carcinoma in the lower eyelid. (B) Sebaceous carcinoma in the ear pinna. (C) Sebaceous carcinoma in the upper lip of a patient with MTS.Fig. 1
The treatment of choice in ten cases of SC was wide excision of the tumor. Mohs micrographic surgery was performed in one case, and in another case, radiotherapy was adopted as an adjuvant method. Only one case was treated with palliative radiotherapy. Four tumors were removed by shaving or saucerization. Patients mean follow-up time was four years, and only nine remained in outpatient follow-up until the end of the study. Three patients had SC metastasis: (1) one SC diagnosed in the lower eyelid, showed metastasis in a cervical lymph node, and wide excision was performed, without new recurrences; (2) two SC diagnosed in the upper and lower eyelids, with parotid and pulmonary metastases, were treated with excision of all tumors associated with radiotherapy, without recurrence; (3) one SC diagnosed in the shoulder, initially treated with wide excision, showed local recurrence one year later associated with lymph node metastasis, and died. There were also two deaths from causes unrelated to SC (hepatocarcinoma and multiple myeloma). The collected data are shown in Table 1.Table 1. Clinical characteristics of patients diagnosed with sebaceous carcinoma.Table 1. Case N.GenderAgeLocationTumor characteristicsOther skin tumorsPersonal historyMuir-Torre SyndromeMetastasisTreatmentRecurrenceFollow-up (time in years)1M51Neck and lipErythematous papule and ulcerated yellowish papule32 sebaceous adenomas and 1 sebaceomaColon adenocarcinomaConfirmed: loss of MLH1 and PMS2 expressionAbsentShavingAbsentOutpatient follow-up (6)2F94Malar regionNo description2 BCCNNAbsentNo descriptionWide local excisionNo descriptionLost to follow-up (2)3M64NoseNo description11 SCC, 7 BCC and 1 malignant sweat gland tumorNNNot investigatedAbsentNo descriptionAbsentOutpatient follow-up (14)4M79MalarPearly keratotic papule3 BCCNNNot investigatedNo descriptionWide local excisionNo descriptionLost to follow-up (<1)5M60NoseUlcerated erythematous plaque1 BCCSigmoid neuroendocrine tumor and hepatocellular carcinomaConfirmed: loss of MSH-2 and MSH-6 expressionAbsentShavingAbsentDeath from hepatocarcinoma (2)6M67ScalpPearly erythematous tumor with telangiectasia1 SCCNNAbsentNo descriptionWide local excisionNo descriptionLost to follow-up (<1)7F61Lower eyelidYellowish nodule with telangiectasias and ulcerationAbsentNNNot investigatedCervical lymph nodeWide local excisionAbsentOutpatient follow-up (5)8F81Upper eyelidReddish nodule with telangiectasiasAbsentNNNot investigatedNo descriptionLocal excisionNo descriptionLost to follow-up (1)9M65NoseNo description2 sebaceous adenomas and 1 SCCNon-Hodgkin lymphoma and colon adenocarcinomaNot investigatedNo descriptionNo descriptionNo descriptionLost to follow-up (<1)10F69ShoulderErythematous nodule with pearly gloss1 BCCNNNot investigatedLymph nodeWide local excisionLocal recurrence after one year with lymph node involvementDeath (2)11F86Malar regionKeratotic plaque2 SCCNNNot investigatedNo descriptionSaucerizationNo descriptionLost to follow-up (<1)12F64Upper eyelidNo descriptionAbsentNNAbsentAbsentWide local excisionAbsentOutpatient follow-up (4)13M71ChestErythematous and grayish tumor2 SCCNNNot investigatedAbsentWide local excisionAbsentOutpatient follow-up (2)14M67NoseExophytic ulcerated noduleAbsentColon adenocarcinoma, duodenal papilla adenocarcinoma with liver metastasis and prostate adenocarcinomaConfirmed: loss of MSH-2 and MSH-6 expressionAbsentSaucerizationAbsentOutpatient follow-up (<1)15F24Upper eyelidNo descriptionAbsentBilateral retinoblastomaNot investigatedNo descriptionLocal excisionNo descriptionLost to follow-up (<1)16M52ChinExophytic plaque1 BCC, 1 sebaceoma and 2 sebaceous adenomasColon adenocarcinoma and multiple myelomaConfirmed: loss of MSH-2 expressionNo descriptionWide local excisionAbsentDeath from multiple myeloma (1)17F74NoseYellowish exophytic nodule with telangiectasias and ulcerationAbsentHodgkin's lymphomaNot investigatedNo descriptionNo descriptionNo descriptionLost to follow-up (<1)18F82Ear pinnaKeratotic noduleAbsentInvasive ductal breast carcinomaAbsentAbsentMohs micrographic surgeryAbsentOutpatient follow-up (1)19M62Upper eyelidNo descriptionAbsentNNNot investigatedNo descriptionUnknownUnknownLost to follow-up (<1)20M71Upper and lower eyelidsYellowish ulcerated noduleAbsentNNAbsentAbsentLocal excision and adjuvant RTAbsentOutpatient follow-up (1)21F43Upper and lower eyelidsNo descriptionAbsentNNNot investigatedParotid gland and lungExcision of the primary tumor, parotid gland and lung metastases and RTAbsentOutpatient follow-up (14)22M93Lower eyelidUlcerated plaqueAbsentNNNot investigatedNo descriptionPalliative RTUnknownLost to follow-up (3)BCC, Basal Cell Carcinoma; SCC, Squamous Cell Carcinoma; F, Female; M, Male; NN, Nothing Noteworthy; RT, Radiotherapy.
Morphologically, SC can present with varied characteristics, mimicking benign tumors (sebaceous hyperplasias, sebaceous adenomas, sebaceomas, nevocellular nevi), malignant neoplasms (BCC and SCC), as well as inflammatory diseases, such as chalazion, blepharitis and keratitis. The latter conditions are considered differential diagnoses of periocular lesions.1, 3 SC diagnosis is confirmed by histopathology of biopsies representing the deep dermis (Fig. 2) and immunohistochemical examination (positive EMA (epithelial membrane antigen) positive oil red O stain, positive Sudan black, with these last two stains performed on frozen sections; Fig. 3). Histopathology of SC is characterized by the presence of irregular and asymmetric sebaceous lobules; sebocytes present a vacuolated cytoplasm, hyperchromasia and nuclear atypia (Fig. 2).2, 4 Because it is rare and mimics other dermatoses, inadequate diagnostic procedures, such as shaving and saucerization, are performed, causing a further delay in the diagnosis of SC.Fig. 2(A) Histopathology of sebaceous carcinoma in the left mandibular region (Hematoxylin & eosin, 10x). (B) Histological examination revealed the presence of disordered invasion of the dermis by ill-defined lobules of atypical sebocytes (Hematoxylin & eosin, ×100). (C) In a higher power view, atypical sebocytes can be observed in this tumor (Hematoxylin & eosin, ×400).Fig. 2
Most cases of SC occur sporadically and have as risk factors immunosuppression, especially solid organ transplantation and acquired immunodeficiency syndrome, exposure to ultraviolet (UV) radiation, radiotherapy, viral infections, a history of familial retinoblastoma and MTS.5 The predominance of SC lesions in photoexposed areas was documented in the present study, with 90% of the tumors located in the head and neck and 40% in the eyelid region (among them, two cases with lesions in the upper and lower eyelids). Another piece of evidence that the patients in the present sample had significant photodamage is the diagnosis of other UV-induced skin tumors, such as BCC and SCC, observed in 45% of the cases. Brazil is a country with a high incidence of UV radiation due to its geographic location, thus increasing the risk of the population for developing UV-induced skin malignant tumors.
MTS is a rare autosomal dominant disease in which there is a mutation in a DNA mismatch repair gene (MLH-1, MSH-2, MSH-6, PMS1 Homolog 2 and PMS-2),4, 6, 7 characterized by the presence of benign or malignant neoplasms originating in sebaceous glands that may or may not occur concomitantly with other malignant neoplasms, especially of the gastrointestinal tract and genitourinary system, the most common being colorectal cancer (80% of cases). Keratoacanthoma and BCC with sebaceous differentiation are also commonly diagnosed in these patients.6 In this disease, SC occurs at earlier age ranges and is common in extraocular regions.8 Suspicion of MTS based on the diagnosis of sebaceous tumors allows the early screening for visceral malignancies, which may favor a better prognosis for patients with this syndrome. In the present series, four cases were diagnosed with MTS, showing loss of expression of at least one DNA mismatch repair gene (Fig. 3) and with a history of colon neoplasia accompanied or not by another primary neoplasia. Only one case of MTS did not have another cutaneous neoplasia.Fig. 3. Immunohistochemical examination of a skin biopsy of sebaceous carcinoma from the left mandibular region of a patient with MTS. Immunohistochemical examination demonstrated the expression of mismatch repair genes (A) MLH-1 present (×40), (B) loss of MSH-2 (×400), (C) loss of MSH-6 (x40) and (D) loss of PMS-2 (x400).Fig. 3
Surgical treatment with tumor excision and intraoperative margin assessment is the most indicated for SC.2, 9 However, in periocular tumors, this can be challenging. In cases of margin involvement or locally advanced tumor with narrow margins, adjuvant radiotherapy may be indicated.2, 10 In the present series, there is a report of only one case treated with Mohs micrographic surgery (SC of the ear pinna) and one of adjuvant radiotherapy (SC of the upper and lower eyelids). Both patients were maintained on outpatient follow-up without recurrence of the primary tumor or metastases. The limited availability of trained professionals and equipment to perform Mohs micrographic surgery limits its use.
SC is an aggressive malignant tumor with high mortality (5%‒10%) and recurrence (16%‒18%) rates.3 Poor prognosis factors include tumors larger than 2 cm, multicentric disease, poorly differentiated lesions, and simultaneous involvement of the upper and lower eyelids.9 Three cases of metastases, one case of recurrence, and one death were observed in the present series, but these data were not sufficient to determine the metastasis, recurrence, and mortality rates, since among the limitations of the present study, the loss of patients to follow-up and incomplete documentation made it impossible to calculate them.
This retrospective case series discusses the importance of considering SC as a differential diagnosis, especially in periocular lesions. Early diagnosis, investigation of risk factors, and MTS are important to adopt the appropriate management for the benefit of the patient.
Authors' contributions
Tatiana Mina Yendo: Design and planning of the study; collection, analysis and interpretation of data; drafting and editing of the manuscript, collection, analysis and interpretation of data; critical review of the literature; approval of the final version of the manuscript.
Flavia Mascarenhas Damiani: Collection, analysis and interpretation of data; statistical analysis; drafting and editing of the manuscript; collection, analysis and interpretation of data; critical review of the literature; approval of the final version of the manuscript.
Suzana Matayoshi: Critical review of important intellectual content; approval of the final version of the manuscript.
Marcello Menta Simonsen Nico: Design and planning of the study; critical review of important intellectual content; effective participation in research orientation; intellectual participation in the propaedeutic and/or therapeutic conduct of the studied cases; critical review of the literature; approval of the final version of the manuscript.
Financial support
None declared.
Conflicts of interest
None declared.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Dasgupta T.Wilson L.D.Yu J.B.A retrospective review of 1349 cases of sebaceous carcinoma Cancer 11520091581651898829410.1002/cncr.23952 · doi ↗ · pubmed ↗
- 2Owen J.L.Kibbi N.Worley B.Kelm R.C.Wang J.V.Barker C.A.Sebaceous carcinoma: evidence-based clinical practice guidelines Lancet Oncol 202019 e 699e 7143179779610.1016/S 1470-2045(19)30673-4 · doi ↗ · pubmed ↗
- 3Orr C.K.Yazdanie F.Shinder R.Current review of sebaceous cell carcinoma Curr Opin Ophthalmol 2920184454502998517510.1097/ICU.0000000000000505 · doi ↗ · pubmed ↗
- 4Cicinelli M.V.Kaliki S.Ocular sebaceous gland carcinoma: an update of the literature Int Ophthalmol 392019118711972969646710.1007/s 10792-018-0925-z · doi ↗ · pubmed ↗
- 5Wu A.Rajak S.N.Huilgol S.C.James C.Selva D.Cutaneous sebaceous carcinoma Australas J Dermatol 612020 e 283e 2923195699410.1111/ajd.13234 · doi ↗ · pubmed ↗
- 6Sargen M.R.Starrett G.J.Engels E.A.Cahoon E.K.Tucker M.A.Goldstein A.M.Sebaceous carcinoma epidemiology and genetics: emerging concepts and clinical implications for screening, prevention, and treatment Clin Cancer Res 2720213893933290784310.1158/1078-0432.CCR-20-2473 PMC 7854832 · doi ↗ · pubmed ↗
- 7Cohen P.R.Kurzrock R.Germline testing of mismatch repair genes is needed in the initial evaluation of patients with Muir-Torre Syndrome-associated cutaneous sebaceous neoplasms: a case series Cureus 152023 e 3397510.7759/cureus.33975 PMC 994102736824550 · doi ↗ · pubmed ↗
- 8John A.M.Schwartz R.A.Muir-Torre syndrome (MTS): an update and approach to diagnosis and management J Am Acad Dermatol 7420165585662689265510.1016/j.jaad.2015.09.074 · doi ↗ · pubmed ↗