Pop‐off mechanisms in fetal megacystis: extravasation, umbilical cord cyst, ureterocele and megaureter
L. A. M. Brinkman, L. K. Duin, P. N. Adama van Scheltema, T. E. Cohen‐Overbeek, E. Pajkrt, M. N. Bekker, C. Willekes, E. J. T. Verweij, C. Bilardo, F. Fontanella

TL;DR
This study examines how different pop-off mechanisms in fetal megacystis affect pregnancy outcomes and ultrasound features.
Contribution
The paper provides a comprehensive analysis of pop-off mechanisms in fetal megacystis and their associations with clinical outcomes.
Findings
Umbilical cord cysts are linked to early-onset and severe megacystis with a high rate of complex diagnoses.
Extravasation is associated with abnormal amniotic fluid and poor survival rates.
Megaureter/ureterocele is linked to better survival and fewer additional anomalies.
Abstract
To analyze comprehensively the incidence, antenatal ultrasound characteristics and prognostic implications of antenatal pop‐off mechanisms of the fetal urinary system in pregnancies with suspected fetal megacystis. This was a retrospective multicenter study of pregnancies with suspected fetal megacystis conducted across all academic hospitals in The Netherlands. Three antenatal pop‐off mechanisms were identified: presence of an umbilical cord cyst (UCC), extravasation of urine into the intraperitoneal space (ascites) or perirenal subcapsular (urinoma), and megaureter/ureterocele. Cases that exhibited two different pop‐off mechanisms, underwent vesicoamniotic shunt placement or had unclear information regarding shunt placement were excluded. We compared the antenatal ultrasound characteristics and outcomes among pregnancies with UCC, those with extravasation, those with…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
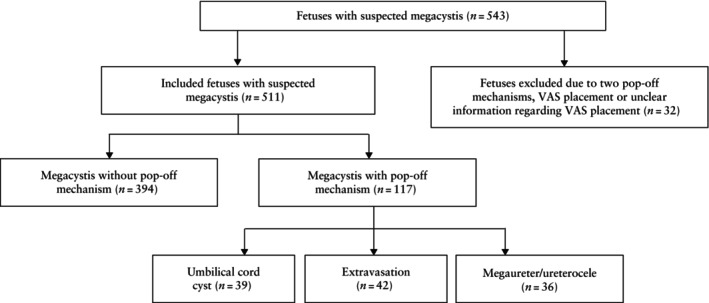 Figure 1
Figure 1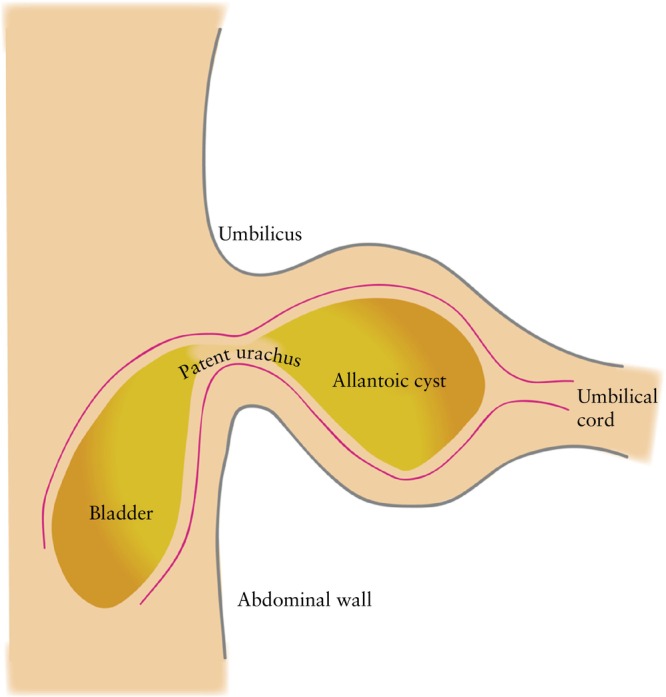 Figure 2
Figure 2| Characteristic | Value |
|---|---|
| Gestational age at diagnosis | 20.00 (13.29–25.61) |
| Pop‐off mechanism | |
| None | 413 (76.1) |
| Umbilical cord cyst only | 39 (7.2) |
| Extravasation only | 47 (8.7) |
| Megaureter/ureterocele only | 39 (7.2) |
| Two mechanisms | 5 (1.0) |
| eGFR (mL/min/1.73 m2) | 85.50 (47.87–109.53) |
| Characteristic | No pop‐off mechanism ( | Umbilical cord cyst ( | Extravasation ( | Megaureter/ureterocele ( |
|
|---|---|---|---|---|---|
| GA at diagnosis | 19.86 (13.14–26.57) | 13.57 (12.14–17.00) | 20.50 (16.53–23.04) | 21.22 (20.04–33.15) | < 0.001 |
| Onset of megacystis | < 0.001 | ||||
| Early (< 18 weeks) | 173/391 (44.2) | 30/39 (76.9) | 13/42 (31.0) | 6/36 (16.7) | |
| Late (≥ 18 weeks) | 218/391 (55.8) | 9/39 (23.1) | 29/42 (69.0) | 30/36 (83.3) | |
| LBD (mm) | 30.00 (18.00–45.00) | 25.05 (16.00–34.75) | 40.00 (26.23–56.00) | 29.50 (23.30–46.00) | 0.026 |
| Severity of megacystis | 0.030 | ||||
| Non‐severe | 151/276 (54.7) | 11/32 (34.4) | 10/30 (33.3) | 11/20 (55.0) | |
| Severe | 125/276 (45.3) | 21/32 (65.6) | 20/30 (66.7) | 9/20 (45.0) | |
| Keyhole sign present | 130/238 (54.6) | 9/21 (42.9) | 24/32 (75.0) | 16/24 (66.7) | 0.060 |
| Thickened bladder wall | 89/192 (46.4) | 6/21 (28.6) | 14/25 (56.0) | 17/20 (85.0) | 0.002 |
| Amniotic fluid index | 0.002 | ||||
| Normal (≥ 5 cm) | 95/216 (44.0) | 18/25 (72.0) | 7/32 (21.9) | 9/16 (56.3) | |
| Abnormal (< 5 cm) | 121/216 (56.0) | 7/25 (28.0) | 25/32 (78.1) | 7/16 (43.8) | |
| Megacystis | 0.029 | ||||
| Isolated | 212/325 (65.2) | 14/33 (42.4) | 21/38 (55.3) | 24/33 (72.7) | |
| Non‐isolated | 113/325 (34.8) | 19/33 (57.6) | 17/38 (44.7) | 9/33 (27.3) | |
| Etiology of megacystis | < 0.001 | ||||
| Normal urinary tract | 39/289 (13.5) | 2/32 (6.3) | 1/36 (2.8) | 15/33 (45.5) | |
| Isolated LUTO | 155/289 (53.6) | 9/32 (28.1) | 21/36 (58.3) | 15/33 (45.5) | |
| Complex diagnosis | 95/289 (32.9) | 21/32 (65.6) | 14/36 (38.9) | 3/33 (9.1) | |
| Trisomy | 26 | 2 | 3 | 0 | |
| Anorectal malformation | 14 | 12 | 4 | 0 | |
| Cause of obstruction in LUTO | 0.025 | ||||
| Non‐specified LUTO | 87/162 (53.7) | 5/14 (35.7) | 14/23 (60.9) | 7/15 (46.7) | |
| PUV | 63/162 (38.9) | 5/14 (35.7) | 7/23 (30.4) | 7/15 (46.7) | |
| Urethral stenosis | 9/162 (5.6) | 0/14 (0) | 0/23 (0) | 1/15 (6.7) | |
| Urethral atresia | 3/162 (1.9) | 4/14 (28.6) | 2/23 (8.7) | 0/15 (0) | |
| Additional associated anomaly | 96/394 (24.4) | 20/39 (51.3) | 17/42 (40.5) | 8/36 (22.2) | < 0.001 |
| Minor | 38/96 (39.6) | 9/20 (45.0) | 5/17 (29.4) | 4/8 (50.0) | |
| Severe | 58/96 (60.4) | 11/20 (55.0) | 12/17 (70.6) | 4/8 (50.0) | |
| Outcome | < 0.001 | ||||
| Termination of pregnancy | 143/385 (37.1) | 17/39 (43.6) | 21/42 (50.0) | 7/36 (19.4) | |
| Intrauterine fetal demise | 27/385 (7.0) | 6/39 (15.4) | 5/42 (11.9) | 1/36 (2.8) | |
| Non‐survivor | 26/385 (6.8) | 3/39 (7.7) | 7/42 (16.7) | 2/36 (5.6) | |
| Alive during follow‐up | 189/385 (49.1) | 13/39 (33.3) | 9/42 (21.4) | 26/36 (72.2) | |
| eGFR | 0.546 | ||||
| Normal (≥ 90 mL/min/1.73 m2) | 41/88 (46.6) | 5/9 (55.6) | 3/6 (50.0) | 10/15 (66.7) | |
| Abnormal (< 90 mL/min/1.73 m2) | 47/88 (53.4) | 4/9 (44.4) | 3/6 (50.0) | 5/15 (33.3) |
| Umblical cord cyst | Extravasation | Megaureter/ureterocele | ||||
|---|---|---|---|---|---|---|
| Characteristic | OR (95% CI) |
| OR (95% CI) |
| OR (95% CI) |
|
| Early‐onset megacystis | 4.200 (1.943–9.082) | < 0.001 | 0.565 (0.285–1.119) | 0.102 | 0.252 (0.103–0.619) | 0.003 |
| Severe megacystis | 2.306 (1.071–4.966) | 0.033 | 2.416 (1.091–5.351) | 0.030 | 0.988 (0.397–2.461) | 0.980 |
| Keyhole sign present | 0.623 (0.253–1.534) | 0.304 | 2.492 (1.076–5.772) | 0.033 | 1.662 (0.685–4.031) | 0.261 |
| Thickened bladder wall | 0.463 (0.172–1.244) | 0.127 | 1.473 (0.636–3.409) | 0.366 | 6.558 (1.861–23.114) | 0.003 |
| Abnormal AFI | 0.305 (0.122–0.761) | 0.011 | 2.804 (1.163–6.761) | 0.022 | 0.611 (0.219–1.700) | 0.345 |
| Isolated megacystis | 0.393 (0.190–0.813) | 0.012 | 0.658 (0.334–1.298) | 0.228 | 1.421 (0.639–3.161) | 0.389 |
| Additional associated anomaly | 3.268 (1.674–6.377) | < 0.001 | 2.111 (1.094–4.075) | 0.026 | 0.887 (0.391–2.011) | 0.774 |
| Severe associated anomaly | 0.801 (0.303–2.115) | 0.654 | 1.572 (0.513–4.822) | 0.429 | 0.655 (0.154–2.779) | 0.566 |
| Alive during follow‐up | 0.519 (0.259–1.039) | 0.064 | 0.283 (0.132–0.607) | 0.001 | 2.696 (1.266–5.743) | 0.010 |
| Abnormal eGFR | 0.698 (0.176–2.774) | 0.609 | 0.872 (0.167–4.561) | 0.871 | 0.436 (0.138–1.381) | 0.158 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPediatric Urology and Nephrology Studies · Urological Disorders and Treatments · Ureteral procedures and complications
INTRODUCTION
Fetal megacystis, identifiable as early as 10 weeks' gestation, is characterized by the presence of a dilated fetal urinary bladder and may result from lower urinary tract obstruction (LUTO), a chromosomal anomaly or another congenital anomaly1, 2, 3. Although pregnancies with severe megacystis are often terminated, milder degrees of bladder dilatation may resolve spontaneously during pregnancy with favorable postnatal outcome1. In severe cases, fetal megacystis has been associated with renal failure, oligohydramnios and pulmonary hypoplasia2. Due to its diverse etiology and unpredictable evolution, the management and counseling of fetal megacystis remain challenging1, 2.
With the natural progression of fetal megacystis, a spectrum of ‘pop‐off’ mechanisms has been observed, reflecting an attempt to alleviate elevated intraluminal urinary pressure and thus protect the renal parenchyma. These mechanisms include the development of an umbilical cord cyst (UCC), which is sometimes detectable sonographically even before the bladder can be identified at 10 weeks' gestation4. Additionally, urine may extravasate into the intraperitoneal space (ascites) or the perirenal subcapsular area (perinephritic urinoma) due to rupture of the renal or upper urinary tract, often resulting in irreversible renal damage. Another pop‐off mechanism is the formation of a megaureter or ureterocele.
These natural pop‐off mechanisms may align with the rationale behind antenatal intervention, which aims to reduce intraluminal pressure and thereby mitigate renal damage. Moreover, these mechanisms may contribute to the vast variability in the antenatal course of fetal megacystis and its postnatal outcome.
Previous studies have focused mainly on the postnatal incidence of pop‐off mechanisms in infants with LUTO5. However, despite their potential relevance in protecting the renal parenchyma during fetal life, the incidence, typical ultrasound appearance and outcomes of pop‐off mechanisms during pregnancy remain largely unexplored. Consequently, their specific roles in determining perinatal and long‐term outcomes remain unclear. It is uncertain whether pop‐off mechanisms offer protection against harmful effects on the urinary system or signify a severe insult which leads to urinary and bladder dysfunction later in life. This study aimed to provide a thorough evaluation of the incidence, antenatal ultrasound characteristics and outcomes of pop‐off mechanisms identified in fetuses with suspected megacystis.
METHODS
Study design and data collection
This retrospective multicenter study was carried out at the fetal medicine units (FMUs) of all academic hospitals in The Netherlands. Data on cases of suspected fetal megacystis were extracted from local databases from the point of digital registration inception in each respective database: from 2000 to the end of 2014 in three centers (Academic Medical Center Amsterdam, Amsterdam; Erasmus MC‐Sophia Children's Hospital University Medical Center, Rotterdam; University Medical Center Maastricht, Maastricht), from 2004 to the end of 2014 in two centers (Radboud University Medical Center, Nijmegen; University Medical Center Groningen, Groningen) and from 2007 to the end of 2014 in three centers (Utrecht University Medical Center, Utrecht; Leiden University Medical Center, Leiden; VU University Medical Center, Amsterdam). This study was approved by the medical ethics committee of the University Medical Center Groningen (METc 2015/445).
In The Netherlands, when there is suspicion of fetal megacystis, referral to a FMU is indicated for confirmation of diagnosis and further investigation. These referrals typically occur following a dating scan, first‐trimester scan, 20‐week anomaly scan or a scan performed later in gestation for another indication. Each referred case underwent a detailed anomaly scan, and parents were counseled on the prognosis of the condition. Information about potential in‐utero treatment options was offered to parents with a male fetus with normal chromosomal analysis, displaying isolated signs of LUTO and with concomitant oligohydramnios. Fetuses that underwent vesicoamniotic shunt placement or cases for which reported information regarding shunt placement was unclear were excluded from data analysis. Pre‐ and postnatal clinical data were collected from the medical records of both the mother and child.
Definitions
In this study, we considered three antenatal pop‐off mechanisms. First, UCC was defined broadly as a hypoechogenic area within the umbilical cord or (suspicion of) a patent urachus, accompanied by the presence of an allantoic cyst. Second, extravasation was defined as ascites (caused by rupture or leakage of the distended bladder) and/or the presence of a urinoma, meaning extravasation of urine into the intraperitoneal space or perirenal subcapsular, respectively, resulting from high intraluminal pressure6, 7. Third, a ureterocele or megaureter was defined as the (intravesical cystic) dilatation of the ureter or dilatation of the portion of the ureter between the renal pelvis and bladder insertion. In the case of a ureterocele, the sonographic presentation may also include a duplex kidney, which indicates duplication of the renal collecting system. This additional finding can be an important diagnostic feature when evaluating the extent and implications of the ureterocele.
Measurements of the longitudinal bladder diameter (LBD) were conducted in a midsagittal view, by measuring the distance from the fetal bladder dome to the bladder neck. Fetal megacystis was defined as a LBD ≥ 7 mm in the first trimester8. After 14 weeks' gestation, a bladder was considered dilated if it failed to empty over a period of at least 45 min8, 9. Furthermore, our study distinguished between early‐onset megacystis, defined as a diagnosis before 18 weeks' gestation, and late‐onset megacystis, defined as a diagnosis at or after 18 weeks' gestation. Moreover, severe megacystis was defined as a LBD ≥ 14 mm before 15 weeks' gestation or as a Z‐score > 5.2 at or after 15 weeks up to and including week 35 of gestation, according to published reference charts10. The keyhole sign was considered to represent a dilatated posterior urethra. The bladder wall was considered ‘thickened’ if > 2 mm, or if labeled as such by the fetal medicine specialist in charge. The uterus was divided into four quadrants to measure the amniotic fluid index (AFI). An AFI < 5 cm was defined as abnormal11.
All postnatal investigations and postmortem examinations were reviewed thoroughly to establish a final diagnosis. LUTO was defined as a bladder outlet obstruction caused by urethral stenosis, urethral valves or urethral atresia. Cases with LUTO reported as the final diagnosis, but without further details concerning the type of obstruction, were defined as non‐specified LUTO. Regarding the etiology of the megacystis, infants with neither LUTO nor a congenital syndrome/severe congenital anomaly were categorized as having a normal urinary tract. The group with complex megacystis included fetuses with trisomy 13, 18 or 21, anorectal malformation (ARM), complex LUTO or another congenital syndrome/chromosomal anomaly (for example, Turner syndrome or overgrowth syndrome). ARM describes a group of complex congenital anomalies marked by abnormal development of the urorectal septum, resulting in congenital abnormalities of the genitourinary tract, rectum and distal anus, such as cloacal malformation and VACTERL association12.
Associated structural anomalies were divided into minor and severe anomalies. Minor associated anomalies included single umbilical artery, echogenic bowel, choroid plexus cyst, macroglossia, hypoplastic nasal bone, shortened long bones, increased nuchal translucency thickness, isolated ventriculomegaly, strawberry sign and arachnoid cyst. Severe associated anomalies included cardiac anomaly, hydrops, skeletal anomaly, renal agenesis, genital anomaly, hygroma colli, abdominal wall defect, central nervous system anomaly, diaphragmatic hernia and sacrococcygeal teratoma.
Termination of pregnancy was defined as the choice by parents to end the pregnancy by medical intervention or induction before 24 weeks' gestation. Intrauterine fetal demise (IUFD) was defined as fetal death after 20 weeks' gestation. Non‐survivor was defined as the death of a liveborn infant during follow‐up.
Estimated glomerular filtration rate (eGFR), as a measure of postnatal renal function, was calculated using the Schwartz formula, considering the length of the infant and the creatinine nadir within the first year of diagnosis, as the literature has shown this to be a good long‐term predictor for renal function13, 14. eGFR ≥ 90 mL/min/1.73 m^2^ was classified as normal and eGFR < 90 mL/min/1.73 m^2^ was classified as abnormal.
Statistical analysis
Data are presented as median (interquartile range (IQR)) or n (%). The Kruskal–Wallis test was used to compare continuous variables. The chi‐square test or Fisher's exact test was used to compare categorical variables. A P‐value ≤ 0.05 was considered statistically significant. Logistic regression analysis was used to evaluate the association of pop‐off mechanisms with antenatal characteristics and postnatal outcomes, and results are expressed as odds ratios (ORs) with 95% CI. Statistical Package for the Social Sciences (SPSS) version 28.0 (IBM Corp., Armonk, NY, USA) was employed for statistical analysis.
RESULTS
Patient characteristics
In total, 543 fetuses with suspicion of megacystis were identified. Among these cases, the majority (74%) were male and the median gestational age at diagnosis was 20.0 (IQR, 13.3–25.6) weeks (Table 1). Within this cohort, 413 (76%) fetuses exhibited no pop‐off mechanism, 39 (7%) presented with UCC only, 47 (9%) presented with extravasation only, 39 (7%) presented with a megaureter/ureterocele only and 5 (1%) fetuses exhibited two pop‐off mechanisms. This latter group (n = 5) was excluded from analysis, as were 27 fetuses who received vesicoamniotic shunt placement or had unclear information reported regarding shunt placement, leaving 511 fetuses for analysis (Figure 1). Further details concerning the underlying etiology and outcome of the study population have been published previously1.
Flowchart summarizing inclusion of cases with suspected fetal megacystis in the study population. VAS, vesicoamniotic shunt.
Umbilical cord cyst
Among the 39/511 (8%) fetuses with UCC, diagnosis occurred at a median gestational age of 13.6 (IQR, 12.1–17.0) weeks. Compared to the group with no pop‐off mechanism, fetuses with UCC had a significantly higher prevalence (77% vs 44%) and higher odds (OR, 4.2 (95% CI, 1.9–9.1); P < 0.001) of early‐onset megacystis (Tables 2 and 3). Furthermore, UCC was associated with severe megacystis (OR, 2.3 (95% CI, 1.1–5.0); P = 0.033). Fetuses with megacystis associated with UCC were more often characterized by a normal AFI (72%; OR, 3.3 (95% CI, 1.3–8.2); P = 0.011) and had the lowest prevalence of a thickened bladder wall (29%) compared to the groups with other pop‐off mechanisms.
The etiology of megacystis was established from postnatal investigation or postmortem examination in 32/39 (82%) fetuses, of which 21 (66%) had complex megacystis, 9 (28%) had isolated LUTO and 2 (6%) had a normal urinary tract. ARM was the most common underlying etiology among cases in the UCC group with a complex diagnosis (n = 12). Additionally, UCC was associated with the presence of other anomaly (OR, 3.3 (95% CI, 1.7–6.4); P < 0.001), and was the sole pop‐off mechanism for which over 50% of cases manifested additional associated anomaly. Among the cases with additional associated anomaly, 45% were minor and 55% were severe. Compared to fetuses with no or another pop‐off mechanism, fetuses with megacystis associated with UCC experienced the highest rate of IUFD (15%).
Extravasation
Extravasation was noted in 42/511 (8%) fetuses, for which the median gestational at diagnosis was 20.5 (IQR, 16.5–23.0) weeks (Table 2). The majority (69%) of fetuses with extravasation exhibited late‐onset megacystis. The highest frequency (67%) and highest odds (OR, 2.4 (95% CI, 1.1–5.4); P = 0.030) for severe megacystis were reported in this group. Furthermore, compared to fetuses with no or another pop‐off mechanism, this group had the highest prevalence (78%) of abnormal AFI and highest odds (OR, 2.8 (95% CI, 1.2–6.8); P = 0.022) (Tables 2 and 3). Moreover, fetal megacystis with extravasation was associated with the presence of the keyhole sign (OR, 2.5 (95% CI, 1.1–5.8); P = 0.033).
The etiology of megacystis was established from postnatal investigation or postmortem examination in 36/42 (86%) cases, of which the majority (n = 21 (58%)) had isolated LUTO. A normal urinary tract was observed in only one case (3%) in this group. A complex diagnosis was identified as the underlying etiology in 14 (39%) cases, including 4 cases of ARM and 3 cases of trisomy. Furthermore, extravasation was significantly associated with other anomaly (OR, 2.1 (95% CI, 1.1–4.1); P = 0.026). Among cases with additional associated anomaly, fetuses with extravasation exhibited the highest prevalence of severe associated anomaly (71%) compared to fetuses with no or another pop‐off mechanism. These fetuses also had the highest rates of pregnancy termination (50%) and non‐survivors (17%). Consequently, survival was less likely in this group, with decreased odds of survival (OR, 0.3 (95% CI, 0.1–0.6); P = 0.001).
Megaureter/ureterocele
Megacystis associated with a megaureter/ureterocele was identified in 36/511 (7%) fetuses. Diagnosis occurred at a median gestational age of 21.2 (IQR, 20.0–33.2) weeks, which was notably later compared with the other groups (Table 2). Consequently, megaureter/ureterocele was associated with late‐onset megacystis (OR, 4.0 (95% CI, 1.6–9.7); P = 0.003). This group had the highest prevalence of non‐severe megacystis (55%), and the highest prevalence (85%) and highest odds (OR, 6.6 (95% CI, 1.9–23.1); P = 0.003) for a thickened bladder wall (Table 3).
The etiology of megacystis was established from postnatal investigation or postmortem examination in 33/36 (92%) of cases. With respect to the etiology of megacystis, this group exhibited the highest frequency of a normal urinary tract (45%) and the lowest frequency of complex diagnosis (9%), meaning that additional associated anomaly was less common in this group (22%). Isolated LUTO was also a common underlying etiology of megacystis in this group (45%), largely caused by posterior urethral valves (PUV) (47%).
Regarding postnatal outcomes, cases with a megaureter/ureterocele had the highest survival rate (72%) compared with other groups and had the highest odds of being alive during follow‐up (OR, 2.7 (95% CI, 1.3–5.7); P = 0.010). Finally, the highest rate of normal postnatal eGFR was reported in this group (67%), although this finding was not statistically significant.
DISCUSSION
This is the first study to investigate the incidence, ultrasound findings and clinical implications of three antenatal pop‐off mechanisms in pregnancies with suspected fetal megacystis. UCC is associated with early‐onset and severe megacystis, normal AFI and additional associated anomaly, and these cases had the highest rate of IUFD. Extravasation was associated with severe megacystis, abnormal AFI, the keyhole sign and additional associated anomaly, and these cases had the highest rates of pregnancy termination and non‐survivors. Megaureter/ureterocele was associated with late‐onset megacystis and a thickened bladder wall, and these cases had the highest postnatal survival rate.
Pop‐off mechanisms, including ascites and urinoma, have been reported previously in approximately 30% of infants with PUV^5^. Our study investigated their occurrence in fetuses with megacystis and found a prevalence of 23%. Antenatal decompression, facilitated either by intervention or a natural pop‐off mechanism, may protect the renal parenchyma from increased intraluminal pressure15. It can be hypothesized that fetuses with increased intraluminal pressure that do not exhibit a pop‐off mechanism may experience worse outcomes.
Umbilical cord cyst
In our cohort, early‐onset megacystis occurred in 77% of fetuses with megacystis associated with UCC, with a significant OR of 4.2, indicating an association between early‐onset fetal megacystis and UCC and suggesting a potential embryological origin16. The fetal urinary bladder develops from the urogenital sinus, continuous with the allantois, extending to the umbilical cord17. Normally, the allantois is obliterated between 6 and 12 weeks' gestation, leaving behind a structure, the urachus, which connects the umbilicus to the bladder apex (Figure 2)18, 19. Consequently, megacystis occurring before the obliteration of the allantois may result in a small drainage within the umbilical cord, hindering allantois closure and causing a patent urachus/allantoic cyst.
Representation of an allantoic cyst resulting from patent urachus.
Furthermore, our study found significant clinical implications of UCC, including a 66% prevalence of complex diagnosis, primarily represented by ARM. Beyond fetal megacystis, UCC has been associated with chromosomal and structural defects, with a prevalence of 20% among all cases18. In our study, fetuses with UCC had 3.3 times higher odds of additional associated anomaly compared to fetuses without a pop‐off mechanism. Furthermore, the UCC group experienced the highest rate of IUFD observed in our study. UCC may predispose fetuses to umbilical cord hematoma near the fetal insertion, possibly due to vessel compression from the expanding cyst, leading to vessel wall ischemia and weakness as well as tearing of the umbilical cord20. Such hematomas could contribute to IUFD at any stage of pregnancy20.
Extravasation
Extravasation of urine may result from elevated pressure within the urinary tract, leading to rupturing of the calyceal fornix and subsequent formation of ascites or urinoma21. This accounts for up to 30% of all cases of neonatal ascites22. Previous studies proposed antenatal ascites and urinoma as pop‐off mechanisms in fetuses with PUV, leading to improved renal function and lower rates of chronic kidney disease, and highlighted the clinical relevance of antenatal intervention15, 21, 23, 24. In our study, abnormal postnatal eGFR was more common in the group without pop‐off mechanisms, albeit not significantly so, suggesting that pop‐off mechanisms could exert a positive influence on postnatal eGFR. Among those with pop‐off mechanisms, abnormal eGFR was reported more frequently in the group with extravasation. This could be due to the inclusion of urinomas, which still exert pressure on the developing renal parenchyma, and the resorption capacity within the retroperitoneal space is less efficient than that in the peritoneum25.
The exact pathogenesis of extravasation remains unclear, but it is strongly linked to obstructions of the upper and lower urinary tract; more than 60% of urinomas are caused by LUTO26, 27, 28. This aligns with our findings, as LUTO emerged as the major underlying etiology of megacystis with extravasation.
Megaureter/ureterocele
Increased intravesical pressure or obstruction can lead to ureteral dilatation in the fetal urinary system, as seen in conditions such as LUTO and vesicoureteral reflux. This dilatation could alleviate pressure within the bladder and facilitate urine flow. Our study found that fetuses with a megaureter/ureterocele exhibited the highest frequency of thickened bladder wall, which is likely due to the high prevalence of PUV associated with this condition and the presence of the keyhole sign19. Furthermore, fetuses with a megaureter/ureterocele had the highest likelihood of postnatal survival, which could be attributed to the low rate of additional associated anomaly and high rates of late‐onset megacystis and non‐severe megacystis. These fetuses also demonstrated the highest prevalence of normal eGFR postnatally, suggesting a potential protective effect of this pop‐off mechanism on kidney function, although this finding was not statistically significant.
Strengths and limitations
One notable limitation of our study is the lack of routine examination of the entire umbilical cord, potentially resulting in an underestimation of the prevalence of UCC. Additionally, due to the retrospective design and lack of definitive postmortem or postnatal pathological confirmation, details about UCC type (i.e. allantoic cyst, pseudocyst or true cyst) were unavailable. Moreover, although there seemed to be a higher prevalence of normal eGFR among cases with an antenatal pop‐off mechanism, the lack of statistical significance may be attributed to the small number of available eGFR measurements in postnatally surviving patients. Additionally, fetuses without a pop‐off mechanism may have minimal or lower intravesical pressure compared to those with a pop‐off mechanism. To investigate more objectively the role of pop‐off mechanisms, antenatal intravesical pressure should be measured to provide more relevant insights5.
Strengths of this study include its large sample size, making it the first nationwide study on this topic across all academic centers in The Netherlands and providing a comprehensive representation of this condition. Additionally, our investigation highlights the role of UCC as a pop‐off mechanism, particularly in early‐onset fetal megacystis, which is a largely underexplored area.
Conclusions
The presence of antenatal pop‐off mechanisms in fetuses with megacystis, occurring in 23% of cases, may crucially alleviate intraluminal pressure. UCC is associated with early‐onset and severe megacystis, normal AFI and high prevalence of complex diagnosis, notably ARM. Extravasation is associated with severe megacystis, abnormal AFI, the keyhole sign and additional associated anomaly. Megaureter/ureterocele is associated with late‐onset megacystis, a thickened bladder wall and low prevalence of additional associated anomaly. Fetuses presenting with extravasation had the highest rates of termination of pregnancy and non‐survivors, while those with UCC had the highest rate of IUFD, compared to the other groups. In contrast, fetuses with a megaureter/ureterocele demonstrate the most favorable outcomes regarding survival. Understanding the manifestations and outcomes associated with the three described pop‐off mechanisms in the context of fetal megacystis could inform antenatal management strategies and parental counseling.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Fontanella F , Maggio L , Verheij J , et al. Fetal megacystis: a lot more than LUTO. Ultrasound Obstet Gynecol. 2019;53:779‐787.30043466 10.1002/uog.19182 PMC 6593717 · doi ↗ · pubmed ↗
- 2Chen L , Guan J , Gu H , Zhang M . Outcomes in fetuses diagnosed with megacystis: systematic review and meta‐analysis. Eur J Obstet Gynecol Reprod Biol. 2019;233:120‐126.30594021 10.1016/j.ejogrb.2018.12.007 · doi ↗ · pubmed ↗
- 3Sanchez‐Prieto M , Perdomo L , Cortes B , et al. Fetal megacystis: associated structural abnormalities and obstetric outcomes. Fetal Pediatr Pathol. 2023;42:394‐399.36582017 10.1080/15513815.2022.2158052 · doi ↗ · pubmed ↗
- 4Sepulveda W , Leible S , Ulloa A , Ivankovic M , Schnapp C . Clinical significance of first trimester umbilical cord cysts. J Ultras Med. 1999;18:95‐99.10.7863/jum.1999.18.2.9510206815 · doi ↗ · pubmed ↗
- 5Delefortrie T , Ferdynus C , Paye‐Jaouen A , et al. Evaluating the impact of pop‐off mechanisms in boys with posterior urethral valves. Front Pediatr. 2022;10:1014422.36330367 10.3389/fped.2022.1014422 PMC 9622767 · doi ↗ · pubmed ↗
- 6Oktar T , Salabas E , Kalelioglu I , et al. Fetal urinoma and prenatal hydronephrosis: how is renal function affected? Turk J Urol. 2013;39:96‐100.26328088 10.5152/tud.2013.016PMC 4548599 · doi ↗ · pubmed ↗
- 7Miller M , Korzets Z , Blumenfeld Y , et al. Fetal urinoma as a sign of a dysplastic kidney. Pediatr Nephrol. 2003;18:65‐67.12488994 10.1007/s 00467-002-0862-x · doi ↗ · pubmed ↗
- 8Sebire NJ , Von Kaisenberg C , Rubio C , Snijders RJ , Nicolaides KH . Fetal megacystis at 10–14 weeks of gestation. Ultrasound Obstet Gynecol. 1996;8:387‐390.9014277 10.1046/j.1469-0705.1997.08060387.x · doi ↗ · pubmed ↗