Assessing the Impact: The Damage Index for Antiphospholipid Syndrome in the Context of Other Autoimmune Diseases and Cardiovascular Risk Factors
João Faia, Eulália Antunes, Ana Luisa Marques, Pedro Bem Haja, Graziela Carvalheiras

TL;DR
This study shows that secondary APS causes more organ damage than primary APS, and that conditions like hypertension and diabetes worsen outcomes in APS patients.
Contribution
The study identifies SAPS and cardiovascular risk factors as significant contributors to increased organ damage in APS patients.
Findings
Secondary APS patients had significantly higher DIAPS scores compared to primary APS patients.
Hypertension and diabetes were associated with increased organ damage in APS patients.
Dyslipidemia influenced the relationship between APS autoimmunity and cumulative damage.
Abstract
Background Antiphospholipid syndrome (APS) is a chronic autoimmune disorder characterized by thrombotic events and organ damage, often leading to significant morbidity and mortality. The Damage Index for Antiphospholipid Syndrome (DIAPS) was developed to quantify irreversible damage in these patients, providing a tool for better disease management. Objectives This study investigates the long-term accumulation of organ damage in patients with thrombotic APS. Specifically, it examines how damage severity differs between primary APS (PAPS) and secondary APS (SAPS) and how traditional cardiovascular risk factors contribute to disease progression. Understanding these interactions may help refine patient management strategies. Methods A retrospective analysis of 141 patients diagnosed with thrombotic APS was conducted using medical records. The DIAPS score was calculated for each…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
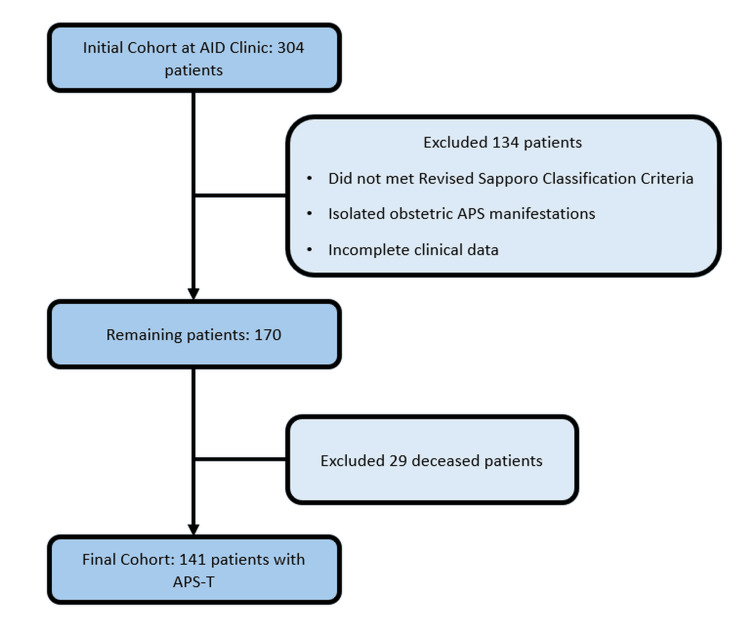 Figure 1
Figure 1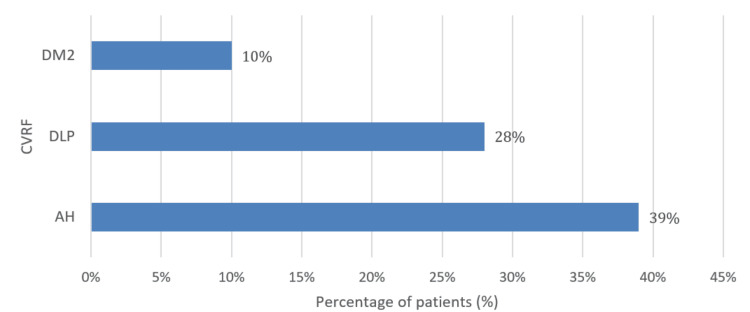 Figure 2
Figure 2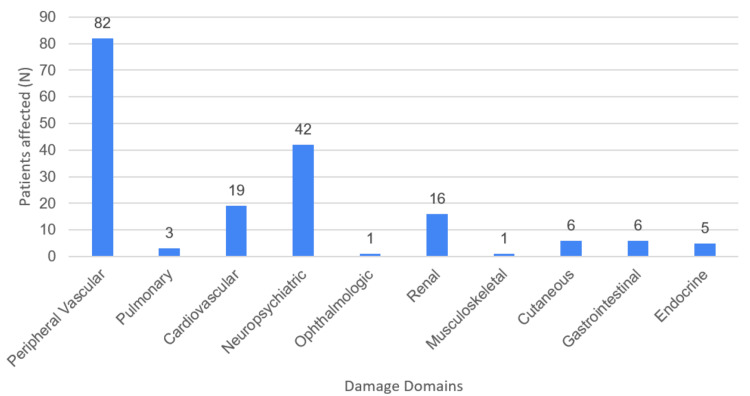 Figure 3
Figure 3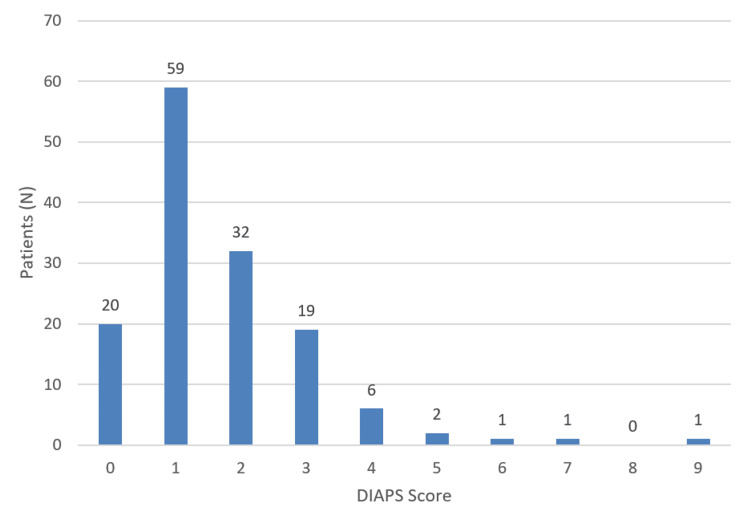 Figure 4
Figure 4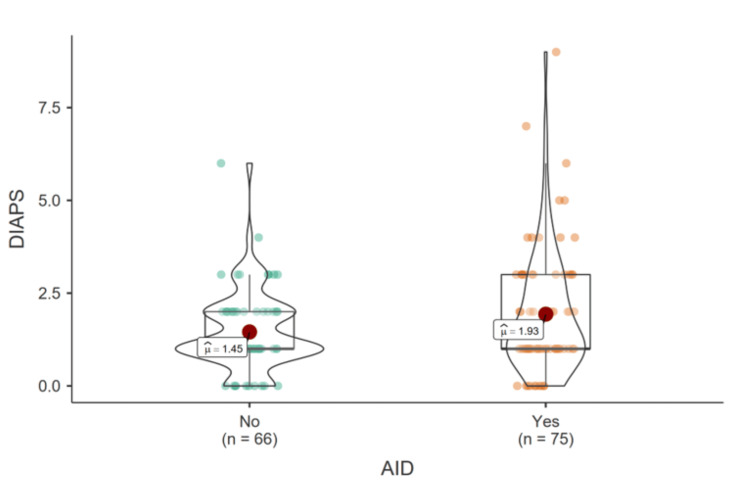 Figure 5
Figure 5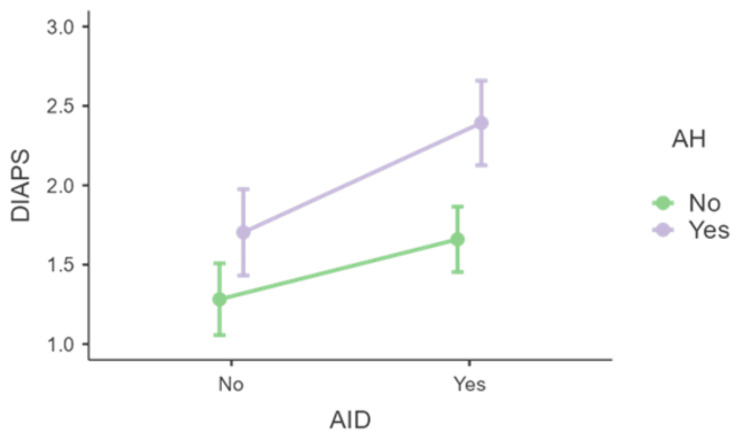 Figure 6
Figure 6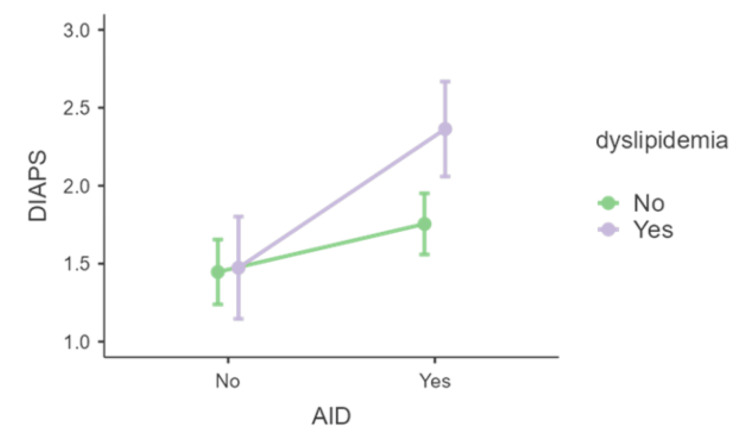 Figure 7
Figure 7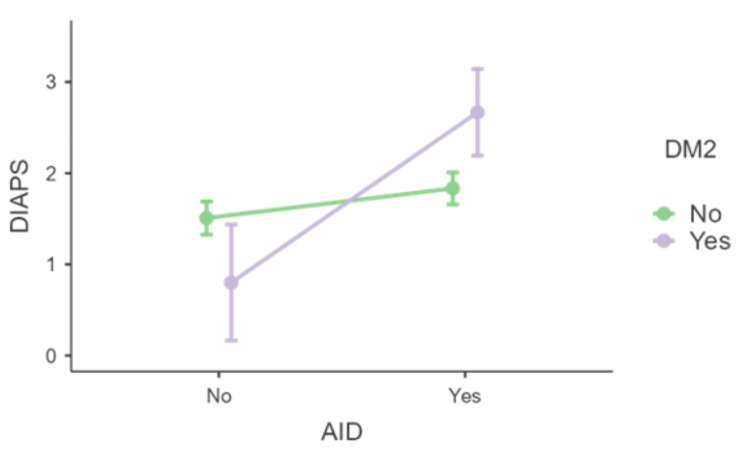 Figure 8
Figure 8| Autoimmune disease (AID) | n | % |
| Systemic lupus erythematosus | 69 | 92 |
| Sjögren's syndrome | 2 | 2.7 |
| Rheumatoid arthritis | 2 | 2.7 |
| Systemic sclerosis | 1 | 1.3 |
| Autoimmune hepatitis | 1 | 1.3 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsSystemic Lupus Erythematosus Research · Liver Diseases and Immunity · Systemic Sclerosis and Related Diseases
Introduction
Background
Antiphospholipid syndrome (APS) is a complex autoimmune disorder characterized by the persistent presence of antiphospholipid antibodies (aPL) and a wide spectrum of clinical manifestations, such as venous and arterial thrombosis, recurrent miscarriages, and organ damage [1,2]. In severe cases, APS may progress to catastrophic APS (CAPS), leading to multiorgan failure and increased mortality, thereby significantly compromising patients' quality of life [3,4].
Given the chronic and progressive nature of APS, quantifying cumulative organ damage is essential for effective long‐term management. In response to this need, the Damage Index for Antiphospholipid Syndrome (DIAPS) was developed as a comprehensive tool to assess irreversible damage resulting from both thrombotic and non‐thrombotic manifestations of APS [5,6]. Derived from the Systemic Lupus International Collaborating Clinics/American College of Rheumatology Damage Index (SLICC/ACRDI) used in systemic lupus erythematosus (SLE), DIAPS incorporates additional criteria tailored specifically to the unique clinical profile of APS [7]. This index evaluates damage across multiple organ systems (including cardiovascular, renal, pulmonary, neurological, and others) and has shown potential as a robust marker of disease progression over extended time periods. Initially validated in Latin American cohorts, subsequent studies have confirmed its utility in more diverse populations [5-6,8-9].
Objectives
Although DIAPS is available, the literature offers limited direct comparisons between primary APS (PAPS) and secondary APS (SAPS) associated with other autoimmune diseases, and the influence of traditional cardiovascular risk factors (CVRF), such as arterial hypertension, dyslipidemia, and type 2 diabetes mellitus on long‐term damage remains unclear. Previous studies have examined DIAPS in various contexts; however, a gap exists in understanding how these factors interact to affect irreversible organ damage. Therefore, our study addresses the following research question: Do APS patients with secondary autoimmune conditions exhibit significantly higher DIAPS scores compared to those with primary APS, and is this difference further exacerbated by the presence of cardiovascular risk factors? In other words, we hypothesize that SAPS patients will demonstrate greater cumulative organ damage than PAPS patients, particularly when concomitant CVRF are present. By testing this hypothesis, our study aims to provide novel insights that can enhance risk stratification, inform treatment decisions, and improve long‐term surveillance in APS management.
Materials and methods
Study design and population
This retrospective, descriptive, single-center study was conducted in a specialized tertiary care hospital with a dedicated autoimmune disease (AID) clinic. Electronic medical records of patients with confirmed or suspected antiphospholipid syndrome were analyzed according to the Revised Sapporo Classification Criteria (Sydney, 2006) [1]. The study period encompassed all available records from as early as 1987 until December 2023. Patients with thrombotic APS (APS-T) who were alive at the time of analysis were included. Exclusion criteria were as follows: patients not meeting the Revised Sapporo Classification Criteria, patients with isolated obstetric APS manifestations, patients with incomplete clinical data, deceased patients (to prevent survival bias).
Data collection
Data were extracted from electronic medical records by three independent investigators following a standardized protocol. Predefined criteria were used to ensure consistency, and any discrepancies were resolved by consensus. The variables collected included demographic data, associated autoimmune diseases, cardiovascular risk factors, and organ damage assessed using the Damage Index for Antiphospholipid Syndrome. DIAPS was calculated according to the recommendations of Amigo et al. [5] and comprises 37 items across various organ systems (e.g., cardiovascular, renal, pulmonary, neurological), with a total score ranging from 0 (no damage) to 37 points.
Statistical analysis
Statistical analyses were performed using R software (version 4.3.3; R Foundation for Statistical Computing, Vienna, Austria). The normality of continuous variables was assessed using the Shapiro-Wilk test. Welch's t-test was used to compare mean DIAPS scores between patients with PAPS and SAPS. Effect sizes were expressed using Hedge's g with a 95% confidence interval. Additionally, linear regression models were employed to assess the association between DIAPS scores and the presence of CVRF. Simple effects analyses were conducted to evaluate the moderating effect of CVRF on the relationship between DIAPS and associated autoimmune diseases. A significance level of p<0.05 was used for all tests.
Ethical considerations
This study adhered to the ethical principles outlined in the Declaration of Helsinki. Due to the retrospective nature of the analysis, informed consent was waived, and all data were anonymized to ensure participant privacy.
Results
Out of the initial cohort of 304 patients followed at the AID clinic, 134 were excluded because they did not meet the Sapporo classification criteria for APS, did not present APS-T, or had incomplete clinical data. Among the remaining 170 patients diagnosed with APS-T, an additional 29 were excluded due to mortality (Figure 1).
Flow diagram of patient selectionAID - autoimmune disease; APS-T - thrombotic antiphospholipid syndrome
Demographic characteristics and associated autoimmune conditions
In this cohort of 141 APS patients, 121 (86%) were female, with an average age of 52 years. Among these patients, 75 (53%) had an AID, with systemic lupus erythematosus (SLE) being the most common, affecting 69 out of the 75 patients (92%). Table 1 summarizes the other AIDs associated with APS in the study population.
Regarding CVRF, the most prevalent were arterial hypertension (AH), found in 55 patients (39%), dyslipidemia (DLP) in 39 patients (28%), and type 2 diabetes mellitus (DM2) in 14 patients (10%). These three CVRF were the primary ones evaluated in the present study. The distribution of these CVRF is visually represented in Figure 2.
Distribution of CVRF in APS patientsAPS - antiphospholipid syndrome; AH - arterial hypertension; CVRF - cardiovascular risk factors; DLP - dyslipidemia; DM2 - type 2 diabetes mellitus
Overall assessment of DIAPS
The DIAPS assessment revealed a heterogeneous distribution of damage across various organ systems. Peripheral vascular damage was the most commonly affected domain, observed in 82 patients. Neuropsychiatric damage was the second most frequent, affecting 42 patients, followed by cardiovascular and renal damage, affecting 19 and 16 patients, respectively. Other forms of damage, including pulmonary, musculoskeletal, endocrine and ophthalmologic, were less prevalent. A summary of the distribution across organ systems is presented in Figure 3.
Organ-specific damage distribution
The overall damage quantification in the cohort, based on DIAPS, yielded a mean score of 1.71 (range: 0-9). The lowest recorded score was 0, observed in 20 patients, indicating no irreversible damage in these cases. The highest recorded score was 9, with only one patient reaching this level of cumulative damage. The distribution of DIAPS scores is presented in Figure 4. The most common damage score was 1, observed in 59 patients, followed by a score of 2 in 32 patients. Higher scores were less frequent, with one patient each scoring 6, 7, and 9.
DIAPS score distributionDIAPS - Damage Index for Antiphospholipid Syndrome
Correlation between DIAPS in PAPS, SAPS, and CVRF
Welch's t-test was performed to assess the relationship between DIAPS in the presence of AID associated with APS-T. The test revealed a significantly higher mean DIAPS in patients with SAPS compared to those with PAPS (Welch t(127.99)=-2.03, p=0.044, Hedge's g=-0.34, 95% CI: -0.67,-0.01; see Figure 5). The renal domain showed the greatest difference between groups, with higher renal damage observed in the SAPS group.
Distribution of DIAPS in the presence and absence of AIDAID - autoimmune disease; DIAPS - Damage Index for Antiphospholipid Syndrome
Subsequently, linear models were employed to assess whether the presence of CVRF also predicted higher DIAPS, whether the effect of AID remained significant, and whether CVRF moderated the relationship between AID and DIAPS.
The presence of AH was associated with an increase in DIAPS (F(1,137)=5.599, p=0.019, η²p=0.039). Although the effect of AID remained significant, further analysis of the simple effects of AID with AH as a moderator revealed that the significant difference in DIAPS between the presence and absence of AID was only observed when AH was present (F(1,137)=3.279, p=0.052; see Figure 6).
Distribution of DIAPS in the presence or absence of AID and AHAID - autoimmune disease; AH - arterial hypertension; DIAPS - Damage Index for Antiphospholipid Syndrome
Regarding DLP, its presence did not significantly alter DIAPS values (p>0.233). However, an analysis of the simple effects of AID with DLP as a moderator indicated that the significant difference in DIAPS between the presence and absence of AID was only observed when DLP was present (F(1,137)=3.98, p=0.048), and not when it was absent (F(1,137)=1.159, p=0.284, see Figure 7).
Distribution of DIAPS in the presence or absence of AID and dyslipidemiaAID - autoimmune disease; DIAPS - Damage Index for Antiphospholipid Syndrome
Lastly, for the presence of DM2, the analysis of simple effects revealed that the pattern observed with other risk factors not only persisted but was amplified, with a significant difference in DIAPS between the presence and absence of AID only occurring in the presence of DM2 (F(1,137)=3.98, p=0.048, see Figure 8).
Distribution of DIAPS in the presence or absence of AID and DM2AID - autoimmune disease; DIAPS - Damage Index for Antiphospholipid Syndrome; DM2 - type 2 diabetes mellitus
Discussion
The present study aimed to investigate the relationship between the DIAPS and various clinical factors, with particular emphasis on cardiovascular risk factors and associated autoimmune diseases in patients with thrombotic APS. Our findings indicate that patients with secondary APS exhibit significantly higher DIAPS scores than those with primary APS, a result that is in line with previous studies [8,10-12]. This suggests that the cumulative burden of additional autoimmune conditions, notably systemic lupus erythematosus, exacerbates irreversible organ damage in APS.
One of the key findings was that arterial hypertension (AH) emerged as a strong predictor of increased DIAPS scores. Our analysis demonstrated that the significant difference in damage between patients with and without AID was apparent only in the presence of AH. This observation supports the notion that hypertension may interact with APS pathophysiology to accelerate vascular injury. Similar observations have been reported in earlier studies [13,14], and our results reinforce the potential benefit of stricter blood pressure control in APS patients.
Additionally, while dyslipidemia did not independently alter DIAPS values, its presence moderated the relationship between AID and organ damage. Similarly, type 2 diabetes mellitus showed a pronounced moderating effect, with significant differences in DIAPS observed predominantly in diabetic patients with coexisting AID. These findings suggest possible mechanisms whereby dyslipidemia may enhance oxidative stress and endothelial dysfunction, and diabetes may contribute to vascular injury through chronic hyperglycemia, both of which are known factors in the progression of organ damage [15,16].
Clinically, these results underscore the importance of comprehensive CVRF management in APS patients, especially in those with secondary APS. Current guidelines for APS primarily focus on immunomodulatory and anticoagulant therapies; however, our findings advocate for an integrated approach that includes aggressive management of hypertension, dyslipidemia, and diabetes. This is particularly critical in SAPS patients, who are often managed primarily for their autoimmune disease while CVRF control might be underestimated. Notably, since the renal domain was one of the most affected in SAPS patients, future studies should also evaluate the role of chronic kidney disease (CKD) in exacerbating APS-related damage.
When comparing our findings with previous research, it is evident that our study extends the literature by including both PAPS and SAPS populations and by utilizing DIAPS, a tool that validated across diverse cohorts, to capture cumulative damage. Earlier studies focusing solely on PAPS have provided valuable insights into the impact of CVRF on APS [17]; however, our inclusion of SAPS patients offers novel perspectives on how underlying autoimmune conditions compound the risk.
Despite the strengths of our study, several limitations must be acknowledged. The single-center, retrospective design may limit the generalizability of our results due to potential selection bias and variability in clinical management across different institutions. Additionally, our reliance on electronic medical records raises the possibility of incomplete or missing data, which could affect the accuracy of DIAPS calculations. The exclusion of deceased patients to avoid survival bias may also lead to an underrepresentation of more severe cases, and the lack of longitudinal follow-up data restricts our understanding of how damage accrues over time.
In summary, our study provides compelling evidence that SAPS patients experience greater cumulative organ damage compared to PAPS patients and that CVRF - particularly, hypertension, dyslipidemia, and diabetes - play a significant role in moderating this damage. These findings highlight the need for a multidisciplinary approach that integrates rigorous CVRF management into the standard care of APS patients. Future prospective studies are warranted to confirm these associations and to determine whether targeted interventions for CVRF can improve long-term clinical outcomes in this population.
Conclusions
The results of this study highlight the significant impact of autoimmune comorbidities and cardiovascular risk factors on the Damage Index for Antiphospholipid Syndrome in patients with thrombotic APS. Patients with secondary APS exhibited higher DIAPS scores compared to those with primary APS, suggesting a more severe disease course when additional autoimmune conditions are present. Moreover, traditional CVRF, such as arterial hypertension, dyslipidemia, and type 2 diabetes, were associated with increased long-term damage, underscoring the importance of managing these risk factors alongside APS treatment.
These findings reinforce the need for a multidisciplinary approach to APS management that addresses both autoimmune and cardiovascular aspects of the disease. In particular, our data suggest that more stringent control of CVRF may improve patient outcomes, which could prompt revisions to current management guidelines. Future research should prioritize multicenter and longitudinal studies to validate these findings across diverse populations and to elucidate the underlying biological mechanisms linking autoimmune diseases, CVRF, and cumulative organ damage. In the interim, clinicians are encouraged to integrate aggressive CVRF management into routine APS care, potentially leading to reduced irreversible damage and improved long-term outcomes.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1International consensus statement on an update of the classification criteria for definite antiphospholipid syndrome (APS)J Thromb Haemost Miyakis S Lockshin MD Atsumi T 295306420061642055410.1111/j.1538-7836.2006.01753.x · doi ↗ · pubmed ↗
- 2EULAR recommendations for the management of antiphospholipid syndrome in adults Ann Rheum Dis Tektonidou MG Andreoli L Limper M 129613047820193109240910.1136/annrheumdis-2019-215213 PMC 11034817 · doi ↗ · pubmed ↗
- 3High impact of antiphospholipid syndrome on irreversible organ damage and survival of patients with systemic lupus erythematosus Arch Intern Med Ruiz-Irastorza G Egurbide MV Ugalde J Aguirre C 778216420041471832610.1001/archinte.164.1.77 · doi ↗ · pubmed ↗
- 4Morbidity and mortality in the antiphospholipid syndrome during a 10-year period: a multicentre prospective study of 1000 patients Ann Rheum Dis Cervera R Serrano R Pons-Estel GJ 101110187420152446496210.1136/annrheumdis-2013-204838 · doi ↗ · pubmed ↗
- 5Development and initial validation of a damage index (DIAPS) in patients with thrombotic antiphospholipid syndrome (APS)Lupus Amigo MC Goycochea-Robles MV Espinosa-Cuervo G Medina G Barragán-Garfias JA Vargas A Jara LJ 9279342420152576707110.1177/0961203315576858 · doi ↗ · pubmed ↗
- 6Assessing disease activity and damage in antiphospholipid syndrome Clin Immunol Andrade D Tektonidou MG 10972725520233755814910.1016/j.clim.2023.109727 · doi ↗ · pubmed ↗
- 7The development and initial validation of the Systemic Lupus International Collaborating Clinics/American College of Rheumatology damage index for systemic lupus erythematosus Arthritis Rheum Gladman D Ginzler E Goldsmith C 363369391996860788410.1002/art.1780390303 · doi ↗ · pubmed ↗
- 8Antiphospholipid syndrome damage index (DIAPS): distinct long-term kinetic in primary antiphospholipid syndrome and antiphospholipid syndrome related to systemic lupus erythematosus Lupus Torricelli AK Ugolini-Lopes MR BonfáE Andrade D 2562622920203198696210.1177/0961203320901598 · doi ↗ · pubmed ↗