Clinical results of combined aortic valve-sparing root replacement and mitral valve repair
Veronica Lorenz, Jama Jahanyar, Stefano Mastrobuoni, Antonio Segreto, Luca Zanella, Gaby Aphram, Matteo Pettinari, Gebrine El Khoury, Laurent De Kerchove

TL;DR
This study evaluates the long-term outcomes of combining aortic valve-sparing surgery with mitral valve repair, showing high survival and durability.
Contribution
The study provides novel long-term clinical data on combined valve-sparing root replacement and mitral valve repair.
Findings
10-year survival rate was 90% with no hospital mortality.
Freedom from reoperation at 10 years was 84%.
Patients with connective tissue disorders had significantly lower freedom from reoperation (63% vs 91%).
Abstract
Aortic valve-sparing root replacement using the reimplantation technique and mitral valve (MV) repair are well-established surgical approaches for the treatment of aortic root pathologies and mitral valve insufficiency. However, the management of concomitant diseases with a dual valve-preserving strategy remains poorly described. Therefore, the aim of this study is to evaluate the long-term outcomes of concomitant valve-sparing surgery and MV repair. This case series includes all the patients who underwent combined valve-sparing root replacement and MV repair at Cliniques Universitaires Saint-Luc (Brussels, Belgium) between January 2000 and June 2022. Actual survival rate and freedom from reoperation were calculated by the Kaplan–Meier method, and the log rank test was used for statistical evaluation. Forty-five patients were included in the study; they were divided into two groups…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
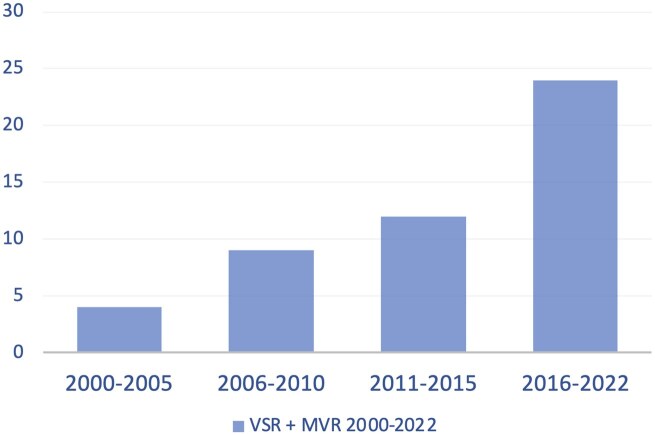 Figure 1
Figure 1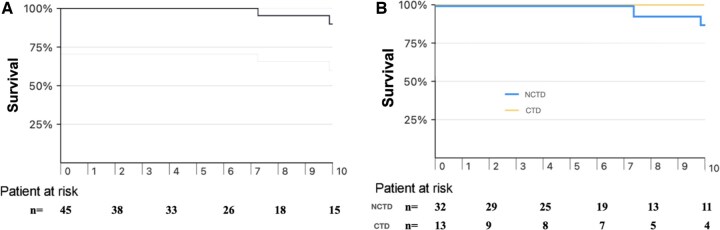 Figure 2
Figure 2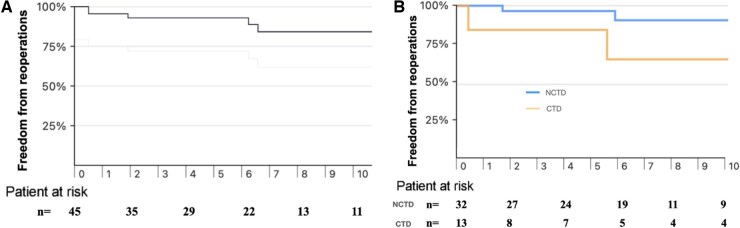 Figure 3
Figure 3| Variables | All ( | NCTD ( | CTD ( |
|
|---|---|---|---|---|
| Age, years, median [IQR] | 55 [35–65] | 58 [54–66] | 30 [18–39] | <0.001 |
| Male sex, % | 40 (89) | 30 (94) | 10 (77) | 0.104 |
| BMI, median [IQR] | 24 [22–27] | 25 [23–28] | 21 [17–23] | <0.001 |
| Previous cardiac surgery | 6 (13) | 4 (13) | 2 (15) | 0.796 |
| Hypertension | 10 (22) | 8 (25) | 2 (15) | 0.482 |
| Renal failure (creat >1.3 mg/dl) | 5 (11) | 5 (16) | 0 | 0.131 |
| Diabetes mellitus | 0 | 0 | 0 | |
| Hyperlipidaemia | 7 (16) | 6 (19) | 1 (8) | 0.354 |
| COPD | 4 (9) | 3 (9) | 1 (8) | 0.857 |
| NYHA | ||||
| I–II | 37 (82) | 27 (84) | 10 (77) | 0.553 |
| III–IV | 8 (18) | 5 (16) | 3 (23) | 0.553 |
| Aortic insufficiency | ||||
| 1 | 20 (44) | 11 (34) | 9 (69) | 0.033 |
| 2 | 9 (20) | 5 (16) | 4 (31) | 0.250 |
| ≥3 | 16 (36) | 16 (50) | 0 | 0.001 |
| Bicuspid aortic valve | 5 (11) | 5 (16) | 0 | 0.131 |
| Aortic root diameter, median [IQR] | 50 [47–54] | 51 [47–54] | 49 [47–57] | 0.486 |
| Left ventricular ejection fraction | ||||
| ≥50% | 36 (80) | 26 (81) | 10 (77) | 0.742 |
| 31–50% | 9 (20) | 6 (19) | 3 (23) | 0.742 |
| Mitral insufficiency | ||||
| Moderate | 7 (16) | 3 (9) | 4 (31) | 0.073 |
| Severe | 38 (84) | 29 (91) | 9 (69) | 0.073 |
| Connective tissue disease | ||||
| Marfan | 11 (24) | |||
| Loeys–Dietz | 1 (2) | |||
| Ehlers–Danlos | 6 (13) |
| Variables | All ( | NCTD ( | CTD ( |
|
|---|---|---|---|---|
| Aortic repair | ||||
| Valve-sparing reimplantation | 45 (100) | 32 (100) | 13 (100) | |
|
| 4 (9) | 4 (13) | 0 | 0.182 |
|
| 41 (91) | 28 (88) | 13 (100) | 0.182 |
| Aortic leaflet repair | 27 (60) | 21 (66) | 6 (46) | 0.227 |
|
| 16 (36) | 14 (44) | 2 (15) | 0.072 |
|
| 7 (16) | 5 (16) | 2 (15) | 0.984 |
|
| 8 (18) | 6 (19) | 2 (15) | 0.789 |
|
| 1 (2) | 1 (3) | 0 | 0.519 |
| Mitral repair | ||||
|
| 12 (27) | 10 (31) | 2 (15) | 0.275 |
|
| 3 (7) | 3 (9) | 0 | 0.253 |
|
| 17 (38) | 10 (31) | 7 (54) | 0.156 |
|
| 4 (9) | 3 (9) | 1 (8) | 0.857 |
|
| 2 (4) | 2 (6) | 0 | 0.356 |
|
| 2 (4) | 2 (6) | 0 | 0.356 |
|
| 5 (11) | 2 (6) | 3 (23) | 0.104 |
| Concomitant procedures | 11 (24) | 10 (31) | 1 (8) | 0.096 |
|
| 2 (4) | 2 (6) | 0 | 0.356 |
|
| 4 (9) | 4 (13) | 0 | 0.182 |
|
| 2 (4) | 2 (6) | 0 | 0.356 |
|
| 1 (2) | 1 (3) | 0 | 0.519 |
| Cross-clamp time, median [IQR] min | 145 [131–165] | 145 [138–165] | 134 [118–154] | 0.089 |
| Cardiopulmonary bypass time, median [IQR] min | 170 [151–202] | 176 [156–203] | 170 [137–193] | 0.444 |
| Variables | All ( | NCTD ( | CTD ( |
|
|---|---|---|---|---|
| Mortality | 0 | 0 | 0 | |
| Postoperative new AF | 8 (18) | 7 (22) | 1 (8) | 0.259 |
| Pacemaker implantation | 3 (7) | 2 (6) | 1 (8) | 0.860 |
| Stroke | 1 (2) | 1 (3) | 0 | 0.519 |
| Hospital stay (days), median [IQR] | 11 [8–15] | 11 [8–15] | 13 [11–13] | 0.350 |
| Discharge echo | ||||
| Aortic insufficiency | ||||
|
| 44 (98) | 31 (97) | 13 (100) | 0.519 |
|
| 1 (2) | 1 (3) | 0 | 0.519 |
|
| 0 | 0 | 0 | |
| Mitral insufficiency | ||||
|
| 44 (98) | 32 (100) | 12 (92) | 0.113 |
|
| 1 (2) | 0 | 1 (8) | 0.113 |
|
| 0 | 0 | 0 |
| Outcome | All ( | NCTD ( | CTD ( |
|---|---|---|---|
| Late death | 5 (11) | 5 (16) | 0 |
| Reoperations | 7 (16) | 3 (10) | 4 (31) |
|
| 2 (5) | 1 (3) | 1 (8) |
|
| 3 (7) | 1 (3) | 2 (15) |
|
| 2 (5) | 1 (3)b,d | 1 (8) |
| Last echocardiography |
| NCTD = 27 | CTD = 7 |
|
| |||
| | 31 (91) | 24 (89) | 7 (100) |
| | 3 (9) | 3 (11) | 0 |
|
| 0 | 0 | 0 |
|
| |||
|
| 28 (82) | 22 (82) | 6 (86) |
|
| 5 (15) | 5 (19) | 0 |
|
| 1 (3) | 0 | 1 (14) |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCardiac Valve Diseases and Treatments · Cardiac Structural Anomalies and Repair · Aortic Disease and Treatment Approaches
INTRODUCTION
Aortic valve-sparing root replacement with the reimplantation technique (VSRR) and mitral valve (MV) repair are well-established surgical interventions for the management of aortic root pathologies and mitral insufficiency (MI) [1, 2]. Although these procedures are frequently performed individually, the simultaneous occurrence of both pathologies in a single patient presents a complex clinical challenge. This is particularly evident in patients with connective tissue disorders (CTD), such as Marfan syndrome and Loeys–Dietz syndrome, in which the coexistence of AV and MV abnormalities is more prevalent [3, 4].
While valve-sparing procedures have demonstrated superior outcomes compared to valve replacement—specifically in terms of long-term survival and avoidance of lifelong anticoagulation—there is a paucity of data regarding the combined use of MV repair and VSRR. Current literature on the concomitant performance of these two procedures is limited, with most studies being small-scale [5–9].
This study aims to evaluate our experience with concomitant MV repair and VSRR in a high-volume centre, focusing on the feasibility, safety and clinical outcomes of this combined approach.
MATERIALS AND METHODS
Ethical statement
This study was approved by the Ethics Committee of the Cliniques Universitaires Saint-Luc, Brussels, Belgium (2013/03JUI/356). Written informed consent was obtained from all participants. The Ethics Committee approved the establishment for stored data and monitor ongoing use of database.
Study population
Patients included in this study were selected based on two primary criteria: aortic root dilatation with indication for VSRR [10], who were found to have moderate to severe mitral insufficiency (MI), or patients indicated for mitral repair due to severe MI, who also presented aortic root dilatation during preoperative evaluation.
The underlying mitral pathology was predominantly degenerative, associated with mitral leaflet prolapse, with or without annular dilatation.
Preoperative and operative information were extracted from our prospectively collected institutional clinical and echocardiographic database containing all cardiac procedures performed in our institution.
The primary outcome of the study was survival including in-hospital and late deaths. In-hospital death was defined as any death occurring during the first 30 days after surgery; any other death was considered a late death. Secondary outcomes included AV or MV reoperation. Outcomes were reported for the entire cohort and for different subgroups, according to the presence or absence of connective tissue disorders (CTD vs NCTD).
Operative data are complete, as well as pre- and postoperative characteristics.
Postoperative echocardiograms were performed before discharge from the hospital and annually or every 1–2 years after the first year post-surgery.
Perioperative data were retrospectively reviewed. Clinical and echocardiographic follow-up was collected from hospital and cardiologist reports.
Operative techniques
All patients underwent surgery via full sternotomy with cardiopulmonary bypass. Warm blood cardioplegia to arrest the heart was given into the aortic root, or directly into the coronary ostia in case of aortic insufficiency (AI). MV was repaired through a standard left atrial approach with posterior leaflet resection techniques, artificial chordae and complete semi-rigid ring annuloplasty. Occasionally, in selected patients with moderate MI and MV disease type 1 or 2 limited to (A2-) P2 segment and to save on operative time, the MV was repaired with an edge-to-edge (Alfieri stitch) performed through the AV. After MV repair, the VSRR was carried out in a standard fashion as previously described by our group using straight tube during early period of the study and Valsalva graft since 2002 (Gelweave and Gelweave Valsalva, Vascutek Ltd, Terumo Company, Renfrewshire, Scotland) [2–15]. There were no differences in outcome when using one or the other prosthesis. Aortic valve lesions, such as cusp prolapse, thickening or large fenestrations were repaired utilizing, respectively, central cusp plication or running suture (Gore-Tex CV-7), shaving and pericardial patch. Occasionally, addition annuloplasty technique (Cabrol Stitch or polytetrafluoroethylene [PTFE] suture annuloplasty) was associated with the reimplantation procedure. PTFE suture annuloplasty (Gore-Tex CV-2, WL Gore and Associates, Flagstaff, AR) was placed around the Dacron graft at the level of the proximal suture line. Suture annuloplasty was tied on the beating heart and under echocardiographic guidance.
All patients were evaluated with a transoesophageal echocardiography to assess the degree of residual AI or MI.
Statistical analyses
Continuous data are presented as median and interquartile range (IQR). Data for categorical variables are reported as frequency and percentage. Actual survival rate and freedom from reoperation were calculated by the Kaplan–Meier method, and the log rank test was used for statistical evaluation. Patients were censored at the last available follow-up entry. In the survival analysis for recurrence of AI or MI, patients were censored at the last available follow-up echo. Statistical analysis was generated utilizing SPSS (IBM Corporation, Armonk, NY). A P value <0.05 was considered statistically significant.
RESULTS
From January 2000 to June 2022, 652 patients underwent VSRR at the Cliniques Universitaires Saint Luc (Brussels, Belgium). Of these, 45 (7%) patients underwent combined VSRR and MV repair. None of the patients underwent an MV replacement. Patients with other concomitant operations, such as coronary artery bypass grafting (CABG) or tricuspid valve repairs, were also included in the final dataset. Figure 1 shows the rate of interventions based on the year of surgery. Most of the patients (n = 32, 71%) were treated in the past decade.
Patients received concomitant VSRR and MV repair between 2000 and 2022.
Patient characteristics
Baseline characteristics and preoperative echocardiographic data are summarized in Table 1.
Forty (89%) patients were male, and median age was 55 (IQR: 35–65) years. Thirteen patients (29%) had a genetic diagnosis of CTD, of which the majority (n = 11) had Marfan syndrome (one Loeys–Dietz and one Ehlers-Danlos syndrome). In addition, six patients had previously undergone cardiac surgery.
The median aortic root diameter was 50 (47–54) mm. The aortic valve (AV) was bicuspid in five patients (11%). Precisely, 36% of patients had an associated AI greater than moderate. Severe MI was found in 86% of patients (14% had moderate MI).
As shown in Table 2, all patients underwent aortic root valve-sparing surgery with the reimplantation technique (David procedure). Valsalva graft was used in majority of the patients (n = 41, 91%). Twenty-seven patients (60%) needed aortic leaflet repair. Cabrol annuloplasty stitches were applied in three (7%) patients and PTFE suture annuloplasty in two patients (4%).
Regarding the MV repair, a complete annuloplasty ring was used in 36 patients (80%). Neochords were used in 7 (16%) patients, and posterior leaflet resection techniques were performed in 23 (51%) patients. Transaortic edge-to-edge MV repair was performed in five (11%) patients, whose diagnosis of moderate MI was made in the operating room before the operation.
Other additional procedures and operative parameters are summarized in Table 2.
Early postoperative outcomes
There was no hospital mortality during index procedure. Postoperative complications are presented in Table 3. One patient had a stroke, and three (7%) patients underwent permanent pacemaker implantation. Precisely, 98% of patients were discharged with a trivial-mild mitral and AI after an average of 8 days of hospital stay.
Late outcomes
The median follow-up duration was 6.5 years, and 15 patients were still at risk at 10 years. A total of five deaths occurred during the follow-up period, three after 10 years (at 11, 14 and 16 years, respectively). One patient died from mitral endocarditis 14 years after surgery; another patient died from unknown cause (by the age of 85), and the remaining three patients died from non-cardiac causes (one pneumonia, one Covid infection, one car accident). Overall survival at 10 years was 90% (95% confidence interval [CI]: 64–97%) (Fig. 2A). Analysing the two subgroups, the 10 years survival was 100% for CTD and 86% (95% CI: 54–96%) for NCTD, with no statistically significant difference (log rank P = 0.393) (Fig. 2B).
(A) Survival following concomitant VSR and MV repair. Estimated survival at 10 years was 89.6% (95% CI: 64.3–97.3%). (B) Survival following concomitant VSRR and MVR in NCTD vs CTD. Estimated survival at 10 years was 86% (95% CI: 54–96%) for NCTD and 100% for CTD (log rank P = 0.393).
During the follow-up period, seven patients required reintervention: two patients on the AV, three on the MV and two patients had reoperation on both AV and MV (Table 4). The linearized risk of reintervention was 2.1%.
Regarding the four patients needing AV reintervention, one was reoperated for stenosis 13 years after bicuspid aortic valve (BAV) repair and the three others for AI. Two of them had had three cusps repaired with running suture, and the last one had right coronary cusp prolapse treated with a running suture (Table 4). In recent years, we have avoided the use of free-edge running sutures because we found to be a risk factor for stenosis and failure of aortic repair [16]. Aortic valve re-repair was performed in one patient, while the remaining three received AV replacement.
Regarding the patients needing MV reintervention, Table 4 shows the causes of recurrence of MI. All five patients were reoperated for severe recurrent MI. Three of them had as initial MV repair technique a transaortic edge-to-edge, one had a commissural edge-to-edge without annuloplasty ring and one had a P2 resection plus annuloplasty ring. At reoperation, all patients underwent successful re-repair with posterior leaflet resection or artificial chordae and annuloplasty ring. All seven patients survived their reoperation.
Freedom from AV and MV reoperations at 10 years for the entire cohort was 84% (95% CI: 64–93%) (Fig. 3A). At 10 years, freedom from reoperation was significantly lower in the CTD group (63% [95% CI: 17–88%]) compared to the NCTD group (91% [95% CI: 66–98%]) (log rank P = 0.031) (Fig. 3B).
(A) Freedom from reoperation following concomitant VSR and MV repair at 10 years was 84% (95% CI: 64–93%). (B) Freedom from reoperation after VSRR and MVR at 10 years was 91% (95% CI: 66–98%) for NCTD and 63% (95% CI: 17–88%) for CTD (log rank P = 0.031).
Competing risk curves are reported in the Supplementary Material (Supplementary Fig. S1).
On last echocardiographic follow-up, one patient (transaortic edge-to-edge MV repair) had developed severe MI and has not been reoperated yet by the patient’s decision. In the whole cohort, also considering the patients who underwent reintervention, 10 years freedom from moderate to severe AI was 90% (95% CI: 70–97%) and freedom from moderate to severe MI was 86% (95% CI: 68–95%) (Kaplan–Meier curves are reported as Supplementary Figs S2 and S3).
During follow-up, one patient had a thromboembolic event, another had endocarditis. Linearized rates were 0.3% for both events. Major bleeding occurred in two patients with a linearized rate of 0.6%.
DISCUSSION
This study evaluates the early and long-term outcomes of patients who underwent concomitant VSRR and MV repair. Valve-preserving operations, especially of the AV, are technically demanding and less frequently performed compared to traditional AV replacement. This is largely due to the intricate nature of maintaining a functional AV while addressing root dilation, as well as concerns about potential postoperative valve dysfunction. In a similar fashion, the decision to also repair the MV adds complexity and requires specialized techniques, although nowadays it is the gold standard at many cardiac surgery centres worldwide [2, 17, 18].
Historically, replacement of the aortic root with a composite valve graft utilizing a mechanical prosthesis has been the go-to procedure for young patients, with or without CTD [19–21]. These facts explain that few studies to date have reported the outcome of large series of combined VSRR and MV repair. The results we show in this nearly unique cohort of patients are favourably compared to literature data regarding several outcomes. Specifically, we report 100% survival at 1 and 5 years, and 90% at 10 years, which is comparable to prior studies that focused on double valve preservation. In a study by David et al. [7], 123 patients underwent combined aortic root replacement with MV surgery. Although in this cohort the AV was only preserved in 21 patients and MV repair was performed in 67 patients, the authors demonstrated that the lowest mortality rate occurred in patients with a first-time VSRR combined with MV repair.
Nicolini et al. published a series of 1167 double AV and MV replacements in 2014. Of these, 443 underwent double mechanical valve replacements and hospital mortality for patients younger than 70 years was 4.8% and 1-year mortality was 7.6%. Interestingly, survival for the entire cohort at 5 years was only 75.1% [22].
In another study, Coutinho et al. [23], reported a 6-year survival of 76.7% after aortic and mitral replacement (45.6% of the cohort had a double mechanical valve).
Finally, in another study by Caus et al. [24], the authors analysed long-term follow-up in a matched population of patients treated with double biological or mechanical prosthesis. For the mechanical group, the results were statistically better compared to biological valves. The mean age was 60-year-old, and survival was 78.9% and 62.3% at 5- and 10 years, respectively. The 10-year freedom from reoperation was 80.6%. The cumulative incidence of thromboembolic and haemorrhagic events was 8% at 5 years, 23.6% at 10 years and 70.6% at 15 years. Overall, disappointing results with prosthetic double valve replacements. This explains that, in recent decades, VSRR has become increasingly popular and affords us the ability to avoid prosthetic AVs with its prosthesis-related complications and its need for chronic anticoagulation [13, 25–28].
Herein, we are sharing one of the largest experiences reported to date with combined VSRR and MV repair including almost 30% of the patients with CTD. The Stanford group has previously reported that 15–20% of patients with aortic root dilation in Marfan patients also presented with significant MV disease requiring surgical correction [29].
In patients with CTD, we found no mortality up to 10 years, likely attributable to the younger age of this cohort.
However, the reoperation rate in this cohort was substantial, with 16% requiring a reoperation at 10 years. This was particularly notable in the CTD group, where the incidence of reoperation was higher, likely due to the progressive nature of the underlying disease [30]. These findings are in line with prior studies on double valve replacements, where reoperation rates increase over time, particularly in patients who underwent mechanical valve replacement [22–24].
Analysing reintervention in detail, our study suggests that the long-term outcomes of combined VSRR and MV repair can be optimized by employing more durable mitral repair techniques. In our study, most patients who failed MV repair and required reoperation underwent initial repair without ring or with the edge-to-edge technique. This highlights the notion that, for each patient, a repair of the MV following the basic principles set forth by Alan Carpentier is crucial. Although sometimes the pathology allows to approach the MV repair through the AV with a simple edge-to-edge repair, we have learned that this approach is not as durable in this patient population and leads to failure early on. Hence, performing a suboptimal repair to limit cardiopulmonary bypass time comes with its own price. Therefore, we now approach these patients with standard MV repair with a complete or incomplete semi-rigid ring. The more complex repairs did not add to mortality or postoperative complications, and our freedom from moderate MI rates at mid-term follow-up was totally acceptable. Importantly, every patient who had an MV valve reoperation underwent a successful re-repair using standard Carpentier techniques.
Regarding AV sparing procedures, more than 50% of the patients in this cohort also required leaflets repairs. During reoperation for recurrent AI, we noted that three patients had undergone one or multiple leaflet prolapse repair with running suture. This technique, however, is rarely used today; leaflet prolapse being principally repaired with central plication.
Interestingly, the fourth patient in this cohort developed aortic stenosis one decade after VSRR, which is consistent with the known long-term progression of AV disease, especially in the context of BAV pathology [16, 31].
Recent interest has been increased in alternative techniques such as the personalized external aortic root support (PEARS), for the management of moderate root aneurysm [32–35]. In 2016, Benedetto et al. [34] described the concomitant use of PEARS and MV repair in two patients. In a multicentre cohort study evaluating 200 consecutive patients treated with PEARS, the most frequent concomitant procedure was mitral repair (10%) [32]. The follow-up is still short, and the authors do not provide information about mitral function during follow-up. Compared to PEARS, we believe that VSRR is a more versatile intervention, because it allows for the repair of the aortic leaflets as well what is often needed especially in case of significant preoperative AI [36].
Finally, we have to mention that, in patients with CTD, the reimplantation technique is also more durable than the remodelling technique [13, 37], which has also been supported by the Toronto group [38]. The remodelling technique leaves areas of weakness in the functional aortic annulus, which are prone to disease recurrence. These areas however, become functionally excluded with the Reimplantation technique.
Study limitations
Although data were gathered in a prospective manner, the retrospective nature of the analysis introduces some limitations, including the potential for selection bias and confounding factors, which may affect the strength of causal conclusions. Moreover, this study is limited by the relatively small sample size and the long study period, which covers 20 years, though most patients were treated in the past decade. The median follow-up period was relatively short, and both follow-up and the last echocardiographic follow-up were not standardized in terms of timing, which could impact consistency in outcome assessment. Additionally, the two study groups were analysed primarily for descriptive purposes due to the limited number of patients. Finally, since all surgeries were performed at a single centre by a limited number of highly experienced surgeons, the results may not be easily generalizable to all institutions or surgical teams.
CONCLUSIONS
In conclusion, our study supports the safety and effectiveness of concomitant VSRR and MV repair. However, reoperation remains a concern, especially in patients with connective tissue disorders. The use of classic Carpentier repair techniques with annular stabilization is crucial, while methods like the edge-to-edge repair should be avoided, as they may offer short-term competence but jeopardize long-term valve durability.
Supplementary Material
ivaf067_Supplementary_Data
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Mastrobuoni S , de Kerchove L, Navarra E et al Long-term experience with valve-sparing reimplantation technique for the treatment of aortic aneurysm and aortic regurgitation. J Thorac Cardiovasc Surg 2019;158:14–23.30635185 10.1016/j.jtcvs.2018.10.155 · doi ↗ · pubmed ↗
- 2David TE , David CM, Tsang W, Lafreniere-Roula M, Manlhiot C. Long-term results of mitral valve repair for regurgitation due to leaflet prolapse. J Am Coll Cardiol 2019;74:1044–53.31439213 10.1016/j.jacc.2019.06.052 · doi ↗ · pubmed ↗
- 3Koda Y , Kawamoto T, Yokawa K et al Mid-term outcomes of simultaneous mitral valve repair in patients with miral regurgitation and concomitant annulo-aortic ectasia. Gen Thorac Cardiovasc Surg 2019;67:1014–20.31041727 10.1007/s 11748-019-01129-z · doi ↗ · pubmed ↗
- 4Kunkala MR , Schaff HV, Li Z et al Mitral valve disease in patients with Marfan syndrome undergoing aortic root replacement.Circulation 2013;128:S 243–724030414 10.1161/CIRCULATIONAHA.112.000113 · doi ↗ · pubmed ↗
- 5Imielski BR , Soletti G, Rahouma M et al The impact of concomitant mitral valve intervention on outcomes of aortic root replacement. J Card Surg 2022;37:4662–9.36273410 10.1111/jocs.17056 · doi ↗ · pubmed ↗
- 6Javadikasgari H , Roselli EE, Aftab M et al Combined aortic root replacement and mitral valve surgery: the quest to preserve both valves. J Thorac Cardiovasc Surg 2017;153:1023–30.e 1.28262292 10.1016/j.jtcvs.2017.01.006 · doi ↗ · pubmed ↗
- 7David TE , Armstrong S, Maganti M, Ihlberg L. Clinical outcomes of combined aortic root replacement with mitral valve surgery. J Thorac Cardiovasc Surg 2008;136:82–7.18603058 10.1016/j.jtcvs.2008.02.038 · doi ↗ · pubmed ↗
- 8Beyersdorf F. Special considerations in mitral valve repair during aortic root surgery. Ann Cardiothorac Surg 2015;4:487–91.26539359 10.3978/j.issn.2225-319X.2014.12.08PMC 4598466 · doi ↗ · pubmed ↗