Spontaneous ruptured congenital bronchial diverticulum presenting with total lung collapse and chronic empyema thoracic
Padungkiat Tangpiroontham

TL;DR
A rare case of a ruptured congenital bronchial diverticulum causing lung collapse and chronic infection is successfully treated with surgery.
Contribution
The paper presents a successful surgical approach combining repair and decortication for a rare condition.
Findings
Spontaneous rupture of a congenital bronchial diverticulum can lead to total lung collapse and chronic empyema.
Accurate imaging and bronchoscopy are essential for diagnosis and surgical planning.
Primary repair with decortication is an effective treatment for this rare condition.
Abstract
Spontaneous rupture of a congenital bronchial diverticulum resulting in total lung collapse and chronic empyema thoracis is a rare condition that presents considerable challenges in preoperative diagnosis and perioperative management. Thorough interpretation of imaging studies and bronchoscopy is crucial for effective surgical planning. This article describes a successful surgical intervention employing primary repair in conjunction with decortication. Tracheobronchial diverticula are rare anatomical entities that can be classified into two subtypes: (i) congenital diverticula, which consist of all layers of the tracheobronchial wall, and (ii) acquired diverticula, which are limited to the mucosal layer.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
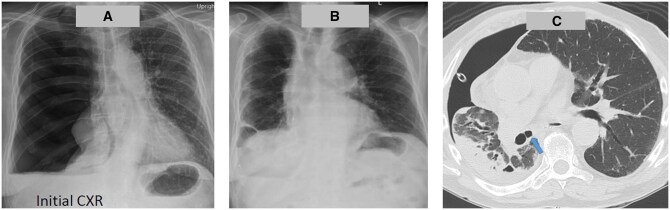 Figure 1
Figure 1 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsTracheal and airway disorders · Congenital Diaphragmatic Hernia Studies · Medical Imaging and Pathology Studies
BACKGROUND
Tracheobronchial diverticula are rare anatomical entities that can be classified into two subtypes: (i) congenital diverticula, which consist of all layers of the tracheobronchial wall, and (ii) acquired diverticula, which are limited to the mucosal layer. Bronchial diverticula are often discovered incidentally through computed tomography (CT) scans and are more prevalent in smokers, typically located in the subcarinal area [1]. These diverticula can mimic other conditions, such as pneumomediastinum [2]. The occurrence of ruptured bronchial diverticula is extremely rare, with few reports documenting a ruptured tracheal diverticulum resulting from barotrauma [3, 4]. We present a case of successful surgical repair of a spontaneously ruptured congenital bronchial diverticulum in a patient who experienced total lung collapse and chronic empyema thoracis.
PATIENTS AND METHODS
A 65-year-old male patient presented to a local hospital with a 6-week history of dry cough, low-grade fever and weight loss, initially treated for bronchitis. A subsequent chest X-ray (CXR) revealed total lung collapse (Fig. 1A), leading to a preliminary diagnosis of a ruptured lung bleb. An intercostal drain was placed, which revealed an air leak and turbid yellow fluid. Follow-up CXR showed partial lung expansion. He was then referred for surgical management. Upon arrival, CT imaging of the chest indicated trapped right lower lobe, right middle lobe and residual pleural effusion. The surgical plan included fibre-optic bronchoscopy, video-assisted thoracoscopic surgery exploration, chest washout and repair of the air leak.
Operative finding and postoperative course: initial CXR (A), 3-month postoperative CXR (B) and bronchial diverticulum on CT chest (C)
Fibre-optic bronchoscopy revealed multiple bronchial diverticula located at the bronchus intermedius, right upper lobe, and right lower lobe, varying in size from 3 to 10 mm (Fig. 2A). Uniportal video-assisted thoracoscopic surgery exploration uncovered diffusely thickened visceral and parietal pleura, with foul-smelling greenish fibrin primarily in the basilar region. Upon removal of the fibrin, a ruptured cartilaginous bronchial diverticulum was identified (Fig. 2B), along with infected material in the diverticulum adjacent to the right lower pulmonary vein, presenting a significant air leak during right lung ventilation. A hybrid minithoracotomy was performed for primary repair using three horizontal mattress sutures of Prolene 4/0 with pledget reinforcement (Fig. 2B). Decortication was subsequently carried out. No air leak was observed at the sutured site under 25 cmH2O lung reinflation. The patient had an uneventful postoperative course, with the intercostal drain removed on postoperative day 11. At 3 months post-discharge, CXR indicated full lung expansion (Fig. 1B). Retrospective analysis revealed bronchial diverticula, which were identifiable on preoperative CT imaging (Fig. 1C).
Intraoperative finding. Red arrow marked diverticulum in BI, yellow arrow marked diverticulum in RLL bronchus (A), green arrow marked bronchial diverticulum pre and post repair (B). BI: bronchus intermedius; RLL: right lower lobe
DISCUSSION
To the best of our knowledge, this is the first case report of spontaneous ruptured congenital bronchial diverticulum combined with chronic empyema thoracis; it made the operation very challenging. The possible cause is believed to be the chronic accumulation of infected material within the diverticulum. We considered primary repair with suture, and decortication were the best option at that moment. If primary repair had failed, we would have planned to proceed with muscle flap with or without Clagett window. Shin et al. [5] described successful management of complicated empyema with BPF using bronchial block, Watanabe spigot and embolization under Venovenous ECMO support during respiratory failure. With increasing Low dose CT [1], tracheobronchial diverticulum may be found more frequent, risk of rupture and infection need to be explained to the patient.
CONCLUSION
Spontaneous rupture of a congenital bronchial diverticulum, resulting in total lung collapse and chronic empyema thoracis, is a rare condition. Primary repair combined with decortication effectively controlled the air leak and led to successful lung re-expansion. Further cases are necessary to better understand optimal management strategies for similar presentations.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Sverzellati N , Ingegnoli A, CalabròE et al Bronchial diverticula in smokers on thin-section CT. Eur Radiol 2010;20:88–94.19597819 10.1007/s 00330-009-1515-2 · doi ↗ · pubmed ↗
- 2Thibodeau R , Warn K, Jafroodifar A, Goel A, Scalzetti E, Deshmane S. Tracheal and main bronchial diverticula simulating pneumomediastinum following a motor vehicle collision. Radiol Case Rep 2021;16:3250–4.34484526 10.1016/j.radcr.2021.08.003PMC 8405918 · doi ↗ · pubmed ↗
- 3O'Leary CN , Ryan JW, Corbett G, Ridge CA. Barotrauma induced tracheal diverticulum rupture: imaging findings. BMJ Case Rep 2016;2016:bcr 2016217518. doi:10.1136/bcr-2016-217518.PMC 505141327677578 · doi ↗ · pubmed ↗
- 4Chakraborty A , Vaish R, Chatterjee A, Sable N, Chaukar D. Tracheal diverticulum: rare presentation of known entity: a case report. A A Pract 2020;14:e 01262.32909716 10.1213/XAA.0000000000001262 · doi ↗ · pubmed ↗
- 5Shin K , Hifumi T, Tsugitomi R et al Empyema with fistula successfully treated with a comprehensive approach including bronchial blocker and embolization receiving veno-venous extracorporeal membrane oxygenation. Acute Med Surg 2021;8:e 621.33604054 10.1002/ams 2.621PMC 7871201 · doi ↗ · pubmed ↗